GoutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or "gout flare," followed later by chronic deforming arthritis. Gout is a heterogeneous metabolic disease associated with elevated serum uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis, or “goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or "gout flare," followed later by chronic deforming arthritis. Gout flare,” followed later by chronic deforming arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis. The kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy can also be affected, and urate crystals can precipitate as chalkstone-like deposits (“tophiTophiMsu deposit in the soft tissue and synovium.Gout”) in the soft tissues, synovial tissues, or in bones near the joints. HyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout is due to overproduction and/or underexcretion of uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis and is a necessary but insufficient precondition to developing urate crystal deposition disease (most hyperuricemic individuals never experience clinical goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or "gout flare," followed later by chronic deforming arthritis. Gout). The most commonly involved joint is the first metatarsophalangeal jointMetatarsophalangeal JointFoot: Anatomy. The identificationIdentificationDefense Mechanisms of urate crystals in joint aspirate or tophiTophiMsu deposit in the soft tissue and synovium.Gout is diagnostic. Effective therapies to relieve the painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways of a goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or "gout flare," followed later by chronic deforming arthritis. Gout flare include nonsteroidal anti-inflammatory drugs (NSAIDsNSAIDSPrimary vs Secondary Headaches), colchicineColchicineA major alkaloid from colchicum autumnale l. And found also in other colchicum species. Its primary therapeutic use is in the treatment of gout.Gout Drugs, and glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids; the choice of therapy depends on the individual and if there are any contraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation.
In the United States, the general prevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency is approximately 3%.
Risk increases with higher body mass indexBody mass indexAn indicator of body density as determined by the relationship of body weight to body height. Bmi=weight (kg)/height squared (m2). Bmi correlates with body fat (adipose tissue). Their relationship varies with age and gender. For adults, bmi falls into these categories: below 18. 5 (underweight); 18. 5-24. 9 (normal); 25. 0-29. 9 (overweight); 30. 0 and above (obese).Obesity (BMIBMIAn indicator of body density as determined by the relationship of body weight to body height. Bmi=weight (kg)/height squared (m2). Bmi correlates with body fat (adipose tissue). Their relationship varies with age and gender. For adults, bmi falls into these categories: below 18. 5 (underweight); 18. 5-24. 9 (normal); 25. 0-29. 9 (overweight); 30. 0 and above (obese).Obesity): prevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency is 1%–2% in those with normal body mass indexBody mass indexAn indicator of body density as determined by the relationship of body weight to body height. Bmi=weight (kg)/height squared (m2). Bmi correlates with body fat (adipose tissue). Their relationship varies with age and gender. For adults, bmi falls into these categories: below 18. 5 (underweight); 18. 5-24. 9 (normal); 25. 0-29. 9 (overweight); 30. 0 and above (obese).Obesity (BMIBMIAn indicator of body density as determined by the relationship of body weight to body height. Bmi=weight (kg)/height squared (m2). Bmi correlates with body fat (adipose tissue). Their relationship varies with age and gender. For adults, bmi falls into these categories: below 18. 5 (underweight); 18. 5-24. 9 (normal); 25. 0-29. 9 (overweight); 30. 0 and above (obese).Obesity), and 5%–7% with class II or class III obesityObesityObesity is a condition associated with excess body weight, specifically with the deposition of excessive adipose tissue. Obesity is considered a global epidemic. Major influences come from the western diet and sedentary lifestyles, but the exact mechanisms likely include a mixture of genetic and environmental factors. Obesity
Middle-aged to elderly men and postmenopausal women are most often affected.
Rare in childhood unless there is an inherited enzyme defect or a malignancyMalignancyHemothorax
Etiology[1,3,15]
HyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout (plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products urate > 6.8 mg/dL) is necessary but not sufficient for the development of goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout.
Only 10% of individuals with hyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout develop goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout.
Elevated uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis (UA) can result from reduced excretion (90%), overproduction, or both.
GoutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout can occur in primary or secondary forms:
Unknown enzyme defects: usually due to decreased excretion of UA
Known enzyme defects: e.g., Lesch-Nyhan syndromeLesch-Nyhan syndromeAn inherited disorder transmitted as a sex-linked trait and caused by a deficiency of an enzyme of purine metabolism; hypoxanthine phosphoribosyltransferase. Elevation of uric acid in the serum leads to the development of renal calculi and gouty arthritis.Purine Salvage Deficiencies and variants of hypoxanthine-guanine phosphoribosyltransferase deficiency (due to increased purine production), glycogen storage diseasesGlycogen Storage DiseasesA group of inherited metabolic disorders involving the enzymes responsible for the synthesis and degradation of glycogen. In some patients, prominent liver involvement is presented. In others, more generalized storage of glycogen occurs, sometimes with prominent cardiac involvement.Benign Liver Tumors (due to decreased excretion of UA)
Increased nucleic acid turnover (e.g., leukemia), due to increased UA production
Chronic renal disease (due to decreased excretion of UA)
Risk factors that increase UA levels[2,3,15,20]
Diets:
Rich in meat and seafood
Beverages containing fruit sugar (fructose), alcohol
ObesityObesityObesity is a condition associated with excess body weight, specifically with the deposition of excessive adipose tissue. Obesity is considered a global epidemic. Major influences come from the western diet and sedentary lifestyles, but the exact mechanisms likely include a mixture of genetic and environmental factors. Obesity
Medical conditions: untreated high blood pressure, diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus, metabolic syndromeMetabolic syndromeMetabolic syndrome is a cluster of conditions that significantly increases the risk for several secondary diseases, notably cardiovascular disease, type 2 diabetes, and nonalcoholic fatty liver. In general, it is agreed that hypertension, insulin resistance/hyperglycemia, and hyperlipidemia, along with central obesity, are components of the metabolic syndrome. Metabolic Syndrome, heart and kidney diseases
Certain medications
ThiazideThiazideHeterocyclic compounds with sulfur and nitrogen in the ring. This term commonly refers to the benzothiadiazines that inhibit sodium-potassium-chloride symporters and are used as diuretics.HyponatremiadiureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication
Low-dose aspirinAspirinThe prototypical analgesic used in the treatment of mild to moderate pain. It has anti-inflammatory and antipyretic properties and acts as an inhibitor of cyclooxygenase which results in the inhibition of the biosynthesis of prostaglandins. Aspirin also inhibits platelet aggregation and is used in the prevention of arterial and venous thrombosis.Nonsteroidal Antiinflammatory Drugs (NSAIDs)
Anti-rejection/immunosuppressive drugsImmunosuppressive drugsAgents that suppress immune function by one of several mechanisms of action. Classical cytotoxic immunosuppressants act by inhibiting DNA synthesis. Others may act through activation of T-cells or by inhibiting the activation of helper cells. While immunosuppression has been brought about in the past primarily to prevent rejection of transplanted organs, new applications involving mediation of the effects of interleukins and other cytokines are emerging.Organ Transplantation used in organ transplantationOrgan TransplantationTransplantation is a procedure that involves the removal of an organ or living tissue and placing it into a different part of the body or into a different person. Organ transplantations have become the therapeutic option of choice for many individuals with end-stage organ failure. Organ Transplantation
Family historyFamily HistoryAdult Health Maintenance of goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout
Age and sexSexThe totality of characteristics of reproductive structure, functions, phenotype, and genotype, differentiating the male from the female organism.Gender Dysphoria: higher prevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency in middle-aged and older men, but UA levels in postmenopausal women approach those of men
Drugs causing acute precipitation of goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout: FACT
C: Anti-Cancer drugs (e.g., cyclosporineCyclosporineA cyclic undecapeptide from an extract of soil fungi. It is a powerful immunosupressant with a specific action on T-lymphocytes. It is used for the prophylaxis of graft rejection in organ and tissue transplantation.Immunosuppressants)
Purine compounds, whether they are synthesized in the body or come from eating high-purine foods, can ↑ uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis levels.[1,16,18]
Uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis is excreted mainly through the kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy.
Overproduction or underexcretion (more common) of uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis can lead to hyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout → supersaturation → deposition of monosodium urate (MSU) crystals in the tissues
Can erode the boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types and damage other tissues such as tendons and cartilageCartilageCartilage is a type of connective tissue derived from embryonic mesenchyme that is responsible for structural support, resilience, and the smoothness of physical actions. Perichondrium (connective tissue membrane surrounding cartilage) compensates for the absence of vasculature in cartilage by providing nutrition and support. Cartilage: Histology
The precise relationship between hyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout and goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout is unclear:
The majority (90%) of people with hyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout do not have goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout.
Normal or ↓ serum uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis levels do not rule out goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout.
However, all patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout will have hyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout (> 6.8 mg/dL) at some point, although levels may fluctuate.
Commonly occurs in the lower extremities, most often at the base of the great toe (first metatarsophalangeal [MTP] joint, or podagra) or the knee
Intensely inflammatory, causing severe painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, rednessRednessInflammation, warmth, swellingSwellingInflammation, and disabilityDisabilityDetermination of the degree of a physical, mental, or emotional handicap. The diagnosis is applied to legal qualification for benefits and income under disability insurance and to eligibility for social security and workman’s compensation benefits.ABCDE Assessment
Peaking within 12–24 hours and resolving within 3–10 days even without treatment
Upon resolution of an acute goutAcute GoutGout flare, patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship enter an intercritical (between-flares) period.
Most often entirely asymptomatic
VariableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables in duration
Most patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship left untreated will develop a recurrent flare within 2 years.
Monosodium urate crystalsMonosodium Urate CrystalsGout may continue to deposit as tophiTophiMsu deposit in the soft tissue and synovium.Gout in various tissues.
Tophaceous goutTophaceous goutNodular deposit of monosodium urate crystals associated with chronic inflammation with a foreign-body giant cell reaction.Gout[3,4]
Found in cartilageCartilageCartilage is a type of connective tissue derived from embryonic mesenchyme that is responsible for structural support, resilience, and the smoothness of physical actions. Perichondrium (connective tissue membrane surrounding cartilage) compensates for the absence of vasculature in cartilage by providing nutrition and support. Cartilage: Histology, subcutaneous and periarticular tissues, tendons (e.g., Achilles tendon), olecranonOlecranonA prominent projection of the ulna that articulates with the humerus and forms the outer protuberance of the elbow joint.Arm: Anatomy bursae, ear helix, kidney, and elsewhere
Can cause destruction of boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types and soft tissueSoft TissueSoft Tissue Abscess
Associated renal complications[3,4,12]
NephrolithiasisNephrolithiasisNephrolithiasis is the formation of a stone, or calculus, anywhere along the urinary tract caused by precipitations of solutes in the urine. The most common type of kidney stone is the calcium oxalate stone, but other types include calcium phosphate, struvite (ammonium magnesium phosphate), uric acid, and cystine stones.Nephrolithiasis
Image: “Tophaceous gout affecting the right great toe and finger interphalangeal joints” by Arthritis Research UK Primary Care Centre, Primary Care Sciences, Keele University, Keele, UK. License: CC BY 2.0
Gouty tophi affecting the hand
Image: “Gouty tophus” by Service de Dermatologie, Chu Hassan II, Fès, Maroc. License: CC BY 2.0
26-year-old man with tophaceous gout that has manifested as tophi in the ear
Image: “Gouty Tophi in the Helix of the Ear” by Michael McCullough. License: CC BY 2.0
Ability to mobilize; impact on work and activities of daily living
Family historyFamily HistoryAdult Health Maintenance of goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout, hyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout, nephrolithiasisNephrolithiasisNephrolithiasis is the formation of a stone, or calculus, anywhere along the urinary tract caused by precipitations of solutes in the urine. The most common type of kidney stone is the calcium oxalate stone, but other types include calcium phosphate, struvite (ammonium magnesium phosphate), uric acid, and cystine stones.Nephrolithiasis, or renal disease
ComorbiditiesComorbiditiesThe presence of co-existing or additional diseases with reference to an initial diagnosis or with reference to the index condition that is the subject of study. Comorbidity may affect the ability of affected individuals to function and also their survival; it may be used as a prognostic indicator for length of hospital stay, cost factors, and outcome or survival.St. Louis Encephalitis Virus and risk factors (see above)
Examine, paying particular attentionAttentionFocusing on certain aspects of current experience to the exclusion of others. It is the act of heeding or taking notice or concentrating.Psychiatric Assessment to:
Warm, red, swollen joints
TophiTophiMsu deposit in the soft tissue and synovium.Gout
Always rule out the possibility of septic arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis:
Refer immediately to relevant specialists, typically trauma and orthopedics
Evaluation[3,4,11,20]
Diagnosis is established via microscopic analysis of the joint aspirate, which shows:
Crystals of MSU, which are negatively birefringent (yellow when parallel to compensator filter) and needle-shaped
WBC > 2,000/μL with > 50% neutrophilsNeutrophilsGranular leukocytes having a nucleus with three to five lobes connected by slender threads of chromatin, and cytoplasm containing fine inconspicuous granules and stainable by neutral dyes.Innate Immunity: Phagocytes and Antigen Presentation (an acute inflammatory synovial fluid)
Note: MSU crystalsMSU crystalsGout can also be seen on aspirates of tophiTophiMsu deposit in the soft tissue and synovium.Gout.
Laboratory studies may show:
↑ Serum urate:
HyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout is defined as a concentration > 6.8 mg/dL (405 µmol/L)
X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests:
Shows no changes early in the disease
As the disease progresses, punched-out erosionsErosionsCorneal Abrasions, Erosion, and Ulcers with an overhanging rim of cortical boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types develop.
HyperechoicHyperechoicA structure that produces a high-amplitude echo (lighter grays and white)Ultrasound (Sonography) enhancement of the surface of articular cartilageCartilageCartilage is a type of connective tissue derived from embryonic mesenchyme that is responsible for structural support, resilience, and the smoothness of physical actions. Perichondrium (connective tissue membrane surrounding cartilage) compensates for the absence of vasculature in cartilage by providing nutrition and support. Cartilage: Histology → MSU crystal deposition
MSU crystalsMSU crystalsGout may also appear as hyperechoicHyperechoicA structure that produces a high-amplitude echo (lighter grays and white)Ultrasound (Sonography) foci floating within the joint space
Monosodium urate crystals, negatively birefringent (appearing as needle-like yellow crystals when parallel to the polarizing light with a red compensator, and blue when perpendicular), from a patient’s joint aspirate. This finding is diagnostic of gout.
Image: “Monosodium Urate Crystals in Elbow Joint Fluid” by Ed Uthman. License: CC BY 2.0
American College of Rheumatology (ACR) criteria[11,14]
Entry criterion: ≥ 1 episode of painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, swellingSwellingInflammation, and/or tenderness in a peripheral joint or bursa
Characteristics of episodes (e.g., erythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion, unable to bear touch/pressure, difficulty using joint)
Number of episodes meeting time-course criteria
Evidence of tophiTophiMsu deposit in the soft tissue and synovium.Gout
The goal of management is to reduce inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation. Acute episodes should be treated as soon as possible.
Management can vary depending on practice location. The following information is based on US, European, and UK literature and guidelines.
General measures
Symptom relief:[6,9]
Consider acetaminophenAcetaminophenAcetaminophen is an over-the-counter nonopioid analgesic and antipyretic medication and the most commonly used analgesic worldwide. Despite the widespread use of acetaminophen, its mechanism of action is not entirely understood.Acetaminophen (paracetamolparacetamolAcetaminophen is an over-the-counter nonopioid analgesic and antipyretic medication and the most commonly used analgesic worldwide. Despite the widespread use of acetaminophen, its mechanism of action is not entirely understood.Acetaminophen) as an adjunct for painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways relief.
Ice packs can provide relief from painful, swollen joints.
Rest and elevate painful limb.
Patient education:[6,9,10,17,21]
Offer lifestyle advice:
Lose weight, if overweight.
Reduce intake of:
Alcohol
Sugary or high-fructose corn syrup–containing drinks
Explain that goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout is a lifelong disease that will progress without treatment.
Direct patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship to (depends on location):
Sources of information
Local support groups
Online forums
National charities
Medical management
Prescribing principles:[6,9,17,21]
The decision about medication class must take into account:
Individual preferences
ComorbiditiesComorbiditiesThe presence of co-existing or additional diseases with reference to an initial diagnosis or with reference to the index condition that is the subject of study. Comorbidity may affect the ability of affected individuals to function and also their survival; it may be used as a prognostic indicator for length of hospital stay, cost factors, and outcome or survival.St. Louis Encephalitis Virus
Other medications
Consider combination therapy if response to monotherapy is inadequate.
Note on antihyperuricemic drugs (allopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs and febuxostatFebuxostatA thiazole derivative and inhibitor of xanthine oxidase that is used for the treatment of hyperuricemia in patients with chronic gout.Gout Drugs):
If already prescribed, then it is safe to continue during acute attacks.
UK: Never commence these during an acute attack, as they may worsen the flare.[9]
US: Per ACR, some patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may benefit from initiating therapy during a flare.[6]
NaproxenNaproxenAn anti-inflammatory agent with analgesic and antipyretic properties. Both the acid and its sodium salt are used in the treatment of rheumatoid arthritis and other rheumatic or musculoskeletal disorders, dysmenorrhea, and acute gout.Nonsteroidal Antiinflammatory Drugs (NSAIDs) at maximum dosageDosageDosage Calculation is suitable.
AspirinAspirinThe prototypical analgesic used in the treatment of mild to moderate pain. It has anti-inflammatory and antipyretic properties and acts as an inhibitor of cyclooxygenase which results in the inhibition of the biosynthesis of prostaglandins. Aspirin also inhibits platelet aggregation and is used in the prevention of arterial and venous thrombosis.Nonsteroidal Antiinflammatory Drugs (NSAIDs) is not indicated.
Continue treatment for 1–2 days after the attack has resolved.
Consider PPI for gastric protection.
Contraindicated in:
Active peptic ulcerPeptic ulcerPeptic ulcer disease (PUD) refers to the full-thickness ulcerations of duodenal or gastric mucosa. The ulcerations form when exposure to acid and digestive enzymes overcomes mucosal defense mechanisms. The most common etiologies include Helicobacter pylori (H. pylori) infection and prolonged use of non-steroidal anti-inflammatory drugs (NSAIDs). Peptic Ulcer Disease disease
Impaired kidney function
Heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR)
Coagulopathy
ColchicineColchicineA major alkaloid from colchicum autumnale l. And found also in other colchicum species. Its primary therapeutic use is in the treatment of gout.Gout Drugs:[6,9,17,21]
Dose:
0.5–0.6 mg 2–4 times daily until painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways relief achieved
Recommended regimen:
Start with 1–1.2 mg.
Follow with 0.5–0.6 mg after 1 hour.
Pause for 12 hours.
Resume treatment with 0.5–0.6 mg every 8 hours until symptoms are relieved.
Maximum dose per course: 6 mg
Course should not be repeated within 3 days.
Has a narrow therapeutic indexTherapeutic IndexAn indicator of the benefits and risks of treatment.Dosage Calculation and is extremely toxic in overdose
Contraindicated in severe renal or liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease (eGFR <10 mL/min)
Drug interactions:
P-glycoprotein inhibitors (macrolide antibiotics, ritonavirRitonavirAn HIV protease inhibitor that works by interfering with the reproductive cycle of HIV. It also inhibits cytochrome p-450 cyp3a.Anti-HIV Drugs, verapamilVerapamilA calcium channel blocker that is a class IV anti-arrhythmia agent.Pulmonary Hypertension Drugs)
CyclosporineCyclosporineA cyclic undecapeptide from an extract of soil fungi. It is a powerful immunosupressant with a specific action on T-lymphocytes. It is used for the prophylaxis of graft rejection in organ and tissue transplantation.Immunosuppressants
GlucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids:[6,9,17]
Example: oral prednisolonePrednisoloneA glucocorticoid with the general properties of the corticosteroids. It is the drug of choice for all conditions in which routine systemic corticosteroid therapy is indicated, except adrenal deficiency states.Immunosuppressants 30–50 mg once daily for 3–5 days
Can be given via IV, IM, oral, or intra-articular routes.
Consider if NSAIDsNSAIDSPrimary vs Secondary Headaches or colchicineColchicineA major alkaloid from colchicum autumnale l. And found also in other colchicum species. Its primary therapeutic use is in the treatment of gout.Gout Drugs are not tolerated or are contraindicated
Interleukin-1Interleukin-1A soluble factor produced by monocytes; macrophages, and other cells which activates T-lymphocytes and potentiates their response to mitogens or antigens. Interleukin-1 is a general term refers to either of the two distinct proteins, interleukin-1alpha and interleukin-1beta. The biological effects of il-1 include the ability to replace macrophage requirements for t-cell activation.Interleukins (IL-1) inhibitors:[6,9,21]
In the US, IL-1 inhibitors are conditionally recommended over no therapy (beyond supportive/analgesic management) in individuals in whom the above therapies are ineffective, not tolerated, or contraindicated.
CanakinumabCanakinumabImmunosuppressants is licensed in Europe by the European Medicines Agency but not in the US by the FDA owing to uncertainty about risks–benefits.
Not recommended by the National Institute for Health and Care Excellence (NICE); off-label prescriptions by a rheumatologist often require fundingFundingConflict of Interest applications.
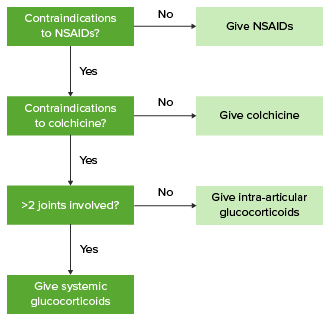
Algorithm for the management of acute gout
Image by Lecturio.
Referrals[9,12]
Seek specialist advice for individuals:
In whom septic arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis is suspected
In whom underlying systemic illness (e.g., rheumatoid arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis or connective tissueConnective tissueConnective tissues originate from embryonic mesenchyme and are present throughout the body except inside the brain and spinal cord. The main function of connective tissues is to provide structural support to organs. Connective tissues consist of cells and an extracellular matrix.Connective Tissue: Histology disorder) is suspected
Who are pregnant
< 30 years of age
Who would benefit from intra-articular steroid injection but the facilities or expertise is not available
At risk of adverse effects of drug treatment
With complications of goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout:
Reduced health-related qualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement of life
Renal stones
TophiTophiMsu deposit in the soft tissue and synovium.Gout
Consider rheumatology referral:
Uncertain diagnosis
Response to treatment inadequate
Treatment not tolerated/contraindicated
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with chronic kidney diseaseChronic Kidney DiseaseChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease, stage 3b–5
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with organ transplants
Follow-up[9,17]
Should occur 4–6 weeks after a flare
Measure serum urate.
Reiterate patient education.
Discuss risk and benefits of urate-lowering therapies.
Assess comorbiditiesComorbiditiesThe presence of co-existing or additional diseases with reference to an initial diagnosis or with reference to the index condition that is the subject of study. Comorbidity may affect the ability of affected individuals to function and also their survival; it may be used as a prognostic indicator for length of hospital stay, cost factors, and outcome or survival.St. Louis Encephalitis Virus, including:
Cardiovascular risk factors
Chronic kidney diseaseChronic Kidney DiseaseChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease
The goal of management is to minimize urate deposition in tissues and to prevent disease flares.
General measures[10,17]
Weight lossWeight lossDecrease in existing body weight.Bariatric Surgery to achieve BMIBMIAn indicator of body density as determined by the relationship of body weight to body height. Bmi=weight (kg)/height squared (m2). Bmi correlates with body fat (adipose tissue). Their relationship varies with age and gender. For adults, bmi falls into these categories: below 18. 5 (underweight); 18. 5-24. 9 (normal); 25. 0-29. 9 (overweight); 30. 0 and above (obese).Obesity < 25
Avoid foods with a high purine content (e.g., seafood, meat, alcohol [varies among different beverages])
Avoid certain medications that cause hyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout
AllopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs is often administered to control goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout if a diuretic is necessary.
Medical treatment
Indications:[6,10,21]
Recurrent attacks (≥ 2 per year)
TophiTophiMsu deposit in the soft tissue and synovium.Gout
Radiographic evidence of boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types damage attributed to goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout
1st goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout flare and:
Chronic kidney diseaseChronic Kidney DiseaseChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease stage 3–5
Uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis level > 9 mg/dL
Urolithiasis
Mechanism of action for xanthine oxidaseOxidaseNeisseria inhibitors:[4,6]
↓ Uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis production by inhibiting xanthine oxidaseOxidaseNeisseria (an enzyme involved in endogenous purine synthesisSynthesisPolymerase Chain Reaction (PCR)).
Benefits:
Eliminate urate crystals
Prevent flares
Shrink tophiTophiMsu deposit in the soft tissue and synovium.Gout
Protect against joint damage
Dosing:[6,10,17,21]
AllopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs:
Typically, the preferred 1st-line agent
Start with 100 mg daily (taken after food).
Adjust in 100-mg increments every 4 weeks according to serum urate.
Amounts > 300 mg should be taken in divided doses.
In severe renal impairment, either:
Reduce daily dose below 100 mg, or
Increase dosing interval
FebuxostatFebuxostatA thiazole derivative and inhibitor of xanthine oxidase that is used for the treatment of hyperuricemia in patients with chronic gout.Gout Drugs:
Starting dose of 40–80 mg or less daily for 2–4 weeks
Increase dose every 2–5 weeks, up to a maximum dose of 120 mg daily
Dose adjustment to a maximum of 80 mg in hepatic impairment
Prescribe for ≥ 6 months
Considerations:[6,10,17]
Offer allopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs as 1st-line therapy in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with major cardiovascular disease (e.g., stroke, myocardial infarctionMyocardial infarctionMI is ischemia and death of an area of myocardial tissue due to insufficient blood flow and oxygenation, usually from thrombus formation on a ruptured atherosclerotic plaque in the epicardial arteries. Clinical presentation is most commonly with chest pain, but women and patients with diabetes may have atypical symptoms.Myocardial Infarction, unstable anginaUnstable anginaPrecordial pain at rest, which may precede a myocardial infarction.Stable and Unstable Angina)
Initiation recommendations vary:
US: ACR conditionally recommends initiating during the goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout flare for certain patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship.[6]
UK: Commence at least 2–4 weeks after goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout flare settles.[10]
Start with low doses and titrate up based on monthly serum urate concentration.
Monitor for hypersensitivity syndrome when starting allopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs.
Consider screeningScreeningPreoperative Care for HLA-BHLA-BClass I human histocompatibility (HLA) surface antigens encoded by more than 30 detectable alleles on locus B of the HLA complex, the most polymorphic of all the HLA specificities. Several of these antigens (e.g., hla-b27, -b7, -b8) are strongly associated with predisposition to rheumatoid and other autoimmune disorders. Like other class I HLA determinants, they are involved in the cellular immune reactivity of cytolytic T lymphocytes.Organ Transplantation*5801 before starting allopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs in subgroups with high prevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency of the alleleAlleleVariant forms of the same gene, occupying the same locus on homologous chromosomes, and governing the variants in production of the same gene product.Basic Terms of Genetics (e.g., Han Chinese, Thai, Korean)
Associated with risk of allopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs hypersensitivity, Stevens-Johnson syndromeStevens-Johnson syndromeStevens-Johnson syndrome (SJS) is a cutaneous, immune-mediated hypersensitivity reaction that is commonly triggered by medications, including antiepileptics and antibiotics. The condition runs on a spectrum with toxic epidermal necrolysis (TEN) based on the amount of body surface area (BSA) involved. Stevens-Johnson Syndrome, and toxic epidermal necrolysisToxic Epidermal NecrolysisStevens-Johnson Syndrome
Do not prescribe to people known to have this alleleAlleleVariant forms of the same gene, occupying the same locus on homologous chromosomes, and governing the variants in production of the same gene product.Basic Terms of Genetics.
Monitor liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy function periodically before and while taking febuxostatFebuxostatA thiazole derivative and inhibitor of xanthine oxidase that is used for the treatment of hyperuricemia in patients with chronic gout.Gout Drugs.
Monitor serum urate:
Aim for target serum urate < 360 µmol/L (6 mg/dL)
Consider lower target serum urate (< 300 µmol/L (5 mg/dL)) for people with:
TophiTophiMsu deposit in the soft tissue and synovium.Gout
Once target urate levels are reached, consider annual monitoring.
Other medication options:[6,10,17,21]
ProbenecidProbenecidThe prototypical uricosuric agent. It inhibits the renal excretion of organic anions and reduces tubular reabsorption of urate. Probenecid has also been used to treat patients with renal impairment, and, because it reduces the renal tubular excretion of other drugs, has been used as an adjunct to antibacterial therapy.Gout Drugs:
Uricosuric drug that inhibits tubular reabsorption of urate → ↑ urinary uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis excretion and ↓ serum urate concentration
Unlicensed in the UK and available only off-license to named patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship under the care of a rheumatologist.
In the US, a trial of probenecidProbenecidThe prototypical uricosuric agent. It inhibits the renal excretion of organic anions and reduces tubular reabsorption of urate. Probenecid has also been used to treat patients with renal impairment, and, because it reduces the renal tubular excretion of other drugs, has been used as an adjunct to antibacterial therapy.Gout Drugs can be started if allopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs and febuxostatFebuxostatA thiazole derivative and inhibitor of xanthine oxidase that is used for the treatment of hyperuricemia in patients with chronic gout.Gout Drugs are not tolerated or are contraindicated.
Note: This is not recommended for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with moderate-to-severe CKDCKDChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease (stage ≥ 3).
An initial dose of 500 mg 1–2 times daily is conditionally recommended.
A recombinant pegylated (i.e., linked to methoxy polyethylene glycolPolyethylene GlycolLaxatives) uricase → uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis metabolized to allantoin → less likely to precipitate
Not currently recommended by NICE
ACR and European League Against Rheumatism (EULAR) recommend pegloticasePegloticaseGout Drugs in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with severe, treatment-refractory goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout (> 2 flares per year or nonresolving tophiTophiMsu deposit in the soft tissue and synovium.Gout).
Concomitant therapy with antiinflammatory medications is recommended to prevent flares during initiation of urate-lowering therapy.
Choice should be based on patient factors, but may include:
ColchicineColchicineA major alkaloid from colchicum autumnale l. And found also in other colchicum species. Its primary therapeutic use is in the treatment of gout.Gout Drugs
GlucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids (e.g., prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants or prednisolonePrednisoloneA glucocorticoid with the general properties of the corticosteroids. It is the drug of choice for all conditions in which routine systemic corticosteroid therapy is indicated, except adrenal deficiency states.Immunosuppressants)
Recommended duration of 3–6 months after initiating urate-lowering therapy with ongoing reevaluation (continue prophylaxisProphylaxisCephalosporins if flares continue)
Patient education:[6,10]
Therapy is continued indefinitely, even after target serum urate level is achieved.
Usually requires lifelong treatment
Seek advice for acute flares
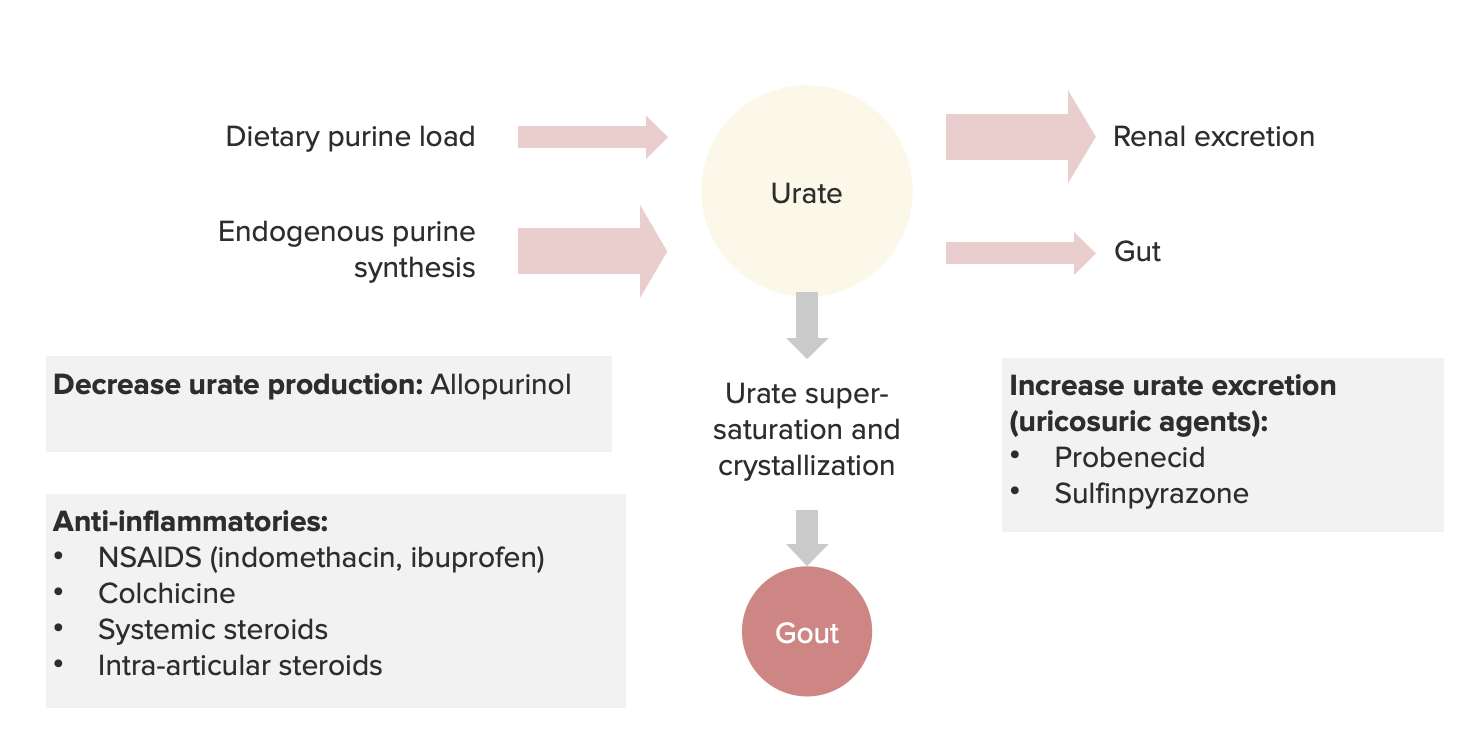
Summary of the pathophysiology and drugs used for gout
The following conditions are differential diagnoses of goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout:
Septic arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis: an infection of a joint with extremely high WBC counts in synovial fluid (> 100,000 cells/mL) are most supportive of a diagnosis of septic arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis. Gram stainGram stainKlebsiella and synovial fluid culture are performed for diagnosis.
CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes pyrophosphate crystal deposition disease (CPPD, pseudogout): positively birefringent crystals in synovial fluid. CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes pyrophosphate crystal deposition disease also has a characteristic radiographic appearance of chondrocalcinosisChondrocalcinosisPresence of calcium pyrophosphate in the connective tissues such as the cartilaginous structures of joints. When accompanied by gout-like symptoms, it is referred to as pseudogout.Gitelman Syndrome.
Trauma: a stress fractureFractureA fracture is a disruption of the cortex of any bone and periosteum and is commonly due to mechanical stress after an injury or accident. Open fractures due to trauma can be a medical emergency. Fractures are frequently associated with automobile accidents, workplace injuries, and trauma.Overview of Bone Fractures or traumatic process in the boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types or joint can mimic a goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout flare.
CellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis: a common and painful bacterial skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions infection that affects the deeper layers of the dermisDermisA layer of vascularized connective tissue underneath the epidermis. The surface of the dermis contains innervated papillae. Embedded in or beneath the dermis are sweat glands; hair follicles; and sebaceous glands.Skin: Structure and Functions and subcutaneous tissueSubcutaneous tissueLoose connective tissue lying under the dermis, which binds skin loosely to subjacent tissues. It may contain a pad of adipocytes, which vary in number according to the area of the body and vary in size according to the nutritional state.Soft Tissue Abscess. Typical signs of acute inflammationAcute InflammationInflammation (ruborRuborInflammation, dolorDolorInflammation, calorCalorInflammation, tumorTumorInflammation) are present but joint mobility is usually preserved.
Rheumatoid arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis: an autoimmune inflammatory polyarthritisPolyarthritisRheumatoid Arthritis. TophiTophiMsu deposit in the soft tissue and synovium.Gout may be mistaken for rheumatoid nodulesRheumatoid NodulesRheumatoid Arthritis but the clinicoradiological presentation and the lack of crystals in the nodular lesions can differentiate the 2 conditions.
DactylitisDactylitisAnkylosing Spondylitis: severe bacterial inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the finger and toe joints that can resemble tophaceous goutTophaceous goutNodular deposit of monosodium urate crystals associated with chronic inflammation with a foreign-body giant cell reaction.Gout with acute flare. The condition can usually be distinguished from goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout based on the history and physical examination.
OsteomyelitisOsteomyelitisOsteomyelitis is an infection of the bone that results from the spread of microorganisms from the blood (hematogenous), nearby infected tissue, or open wounds (non-hematogenous). Infections are most commonly caused by Staphylococcus aureus.Osteomyelitis: an infection (usually bacterial) of the boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types. Diagnosis is made by noting deep bony tenderness and clinical signs of acute systemic inflammationSystemic InflammationSurgical Site Infections; CBC and magnetic resonance imaging (MRI) are helpful if routine radiologic findings are not supportive.
Basic calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.ElectrolytesphosphatePhosphateInorganic salts of phosphoric acid.Electrolytes (BCP) crystal disease (hydroxyapatite (HAHAHemolytic anemia (HA) is the term given to a large group of anemias that are caused by the premature destruction/hemolysis of circulating red blood cells (RBCs). Hemolysis can occur within (intravascular hemolysis) or outside the blood vessels (extravascular hemolysis).Hemolytic Anemia) crystal deposition disease): painful and probably underdiagnosed periarthritis or arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis due to the deposition of BCP crystals in the synovium. The condition can cause severe joint damage, as in the Milwaukee shoulder syndrome seen in elderly women.
Billing and Coding
Diagnosis Codes:
GoutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout is coded by the affected site and can specify if it is with or without tophus (deposits of uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis crystals).
Coding System
Code
Description
ICD-10-CM
M10.9
GoutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout, unspecified
ICD-10-CM
M10.071
IdiopathicIdiopathicDermatomyositisgoutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout, right ankle and footFootThe foot is the terminal portion of the lower limb, whose primary function is to bear weight and facilitate locomotion. The foot comprises 26 bones, including the tarsal bones, metatarsal bones, and phalanges. The bones of the foot form longitudinal and transverse arches and are supported by various muscles, ligaments, and tendons.Foot: Anatomy
This CPT code is for an arthrocentesisArthrocentesisPuncture and aspiration of fluid (e.g., synovial fluid) from a joint cavity. It is used sometimes to irrigate or administer drugs into a joint cavity.Septic Arthritis, or joint fluid aspiration. Microscopic examination of the fluid to identify negatively birefringent, needle-shaped monosodium urate crystalsMonosodium Urate CrystalsGout is the definitive gold standard for diagnosing goutGoutGout is a heterogeneous metabolic disease associated with elevated serum uric acid levels (> 6.8 mg/dL) and abnormal deposits of monosodium urate in tissues. The condition is often familial and is initially characterized by painful, recurring, and usually monoarticular acute arthritis, or “gout flare,” followed later by chronic deforming arthritis. Gout.
Coding System
Code
Description
CPT
20600
ArthrocentesisArthrocentesisPuncture and aspiration of fluid (e.g., synovial fluid) from a joint cavity. It is used sometimes to irrigate or administer drugs into a joint cavity.Septic Arthritis, aspiration and/or injection, small joint or bursa; without ultrasound guidance
CPT
89060
Crystal identificationIdentificationDefense Mechanisms by light microscopy with or without polarizing lensLensA transparent, biconvex structure of the eye, enclosed in a capsule and situated behind the iris and in front of the vitreous humor (vitreous body). It is slightly overlapped at its margin by the ciliary processes. Adaptation by the ciliary body is crucial for ocular accommodation.Eye: Anatomy analysis, any body fluid
Medications:
These codes are for medications to treat an acute goutAcute GoutGout flare, such as colchicineColchicineA major alkaloid from colchicum autumnale l. And found also in other colchicum species. Its primary therapeutic use is in the treatment of gout.Gout Drugs or NSAIDsNSAIDSPrimary vs Secondary Headaches, and for long-term prevention of flares by lowering uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis levels, such as allopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs.
Coding System
Code
Description
RxNorm
2683
ColchicineColchicineA major alkaloid from colchicum autumnale l. And found also in other colchicum species. Its primary therapeutic use is in the treatment of gout.Gout Drugs (ingredient)
RxNorm
546
AllopurinolAllopurinolA xanthine oxidase inhibitor that decreases uric acid production. It also acts as an antimetabolite on some simpler organisms.Gout Drugs (ingredient)
References
Horvai, H. (2020). In Kumar, V., Abbas, A. K., Aster, J. C., (Eds.), Robbins & Cotran Pathologic Basis of Disease. (10th ed., pp. 1204–1206). Elsevier.
Juraschek, S. P., Miller, E. R. 3rd, Gelber, A. C. (2013). Body mass index, obesity, and prevalent gout in the United States in 1988–1994 and 2007–2010. Arthritis Care & Research (Hoboken), 65(1), 127–132. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3482278/
Schumacher, H. R., Chen, L. X. (2018). In Jameson, J. L., et al. (Eds.), Harrison’s Principles of Internal Medicine (20th ed., vol. 2, pp. 2631–2633).
Le, T., Bhusan, V., Sochat, M., et al. (Eds.) (2020). First aid for the USMLE Step 1 (30th ed., p. 467).
FitzGerald, J. D., Dalbeth, N. et al.(2020). 2020 American College of Rheumatology guideline for management of gout. Arthritis and Rheumatology, 72(6), 879–895. https://deepblue.lib.umich.edu/handle/2027.42/155484
Neogi, T., Jansen, T. L., et al.(2015). 2015 Gout classification criteria: an American College of Rheumatology/European League Against Rheumatism Collaborative Initiative. Arthritis and Rheumatology, 67(10), 2557–2568. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4566153/
Bursill, D., et al. (2019). Gout, hyperuricemia, and Crystal-Associated Disease Network consensus statement regarding labels and definitions for disease elements in gout. Arthritis Care & Research, 71(3), 427–434. https://onlinelibrary.wiley.com/doi/epdf/10.1002/acr.23607
Richette, P., et al. (2018). 2018 updated European League Against Rheumatism evidence-based recommendations for the diagnosis of gout. Annals of the Rheumatic Diseases, 79, 31–38. https://ard.bmj.com/content/79/1/31
Richette, P., et al. (2017). 2016 updated EULAR evidence-based recommendations for the management of gout. Annals of the Rheumatic Diseases, 76, 29–42. https://ard.bmj.com/content/76/1/29
Create your free account or log in to continue reading!