Achalasia is an esophageal motility disorder that is due to degeneration of the myenteric plexus; it results in failure of the lower esophageal sphincter to relax and a lack of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids, along with regurgitation. Diagnosis is established by high-resolution manometry. Upper endoscopy is performed to rule out malignancy as a cause. Barium swallow study helps evaluate the esophageal morphology. Management options include pneumatic balloon dilation, surgical myotomy, and botulinum toxin injection. Choice of treatment is dependent on the type of achalasia and surgical risk. Medications are available for those for whom initial intervention fails but provide the least benefit.
Primary esophageal motilityEsophageal MotilityGastrointestinal Motility disorder due to degeneration of the myenteric plexusMyenteric plexusOne of two ganglionated neural networks which together form the enteric nervous system. The myenteric (Auerbach’s) plexus is located between the longitudinal and circular muscle layers of the gut. Its neurons project to the circular muscle, to other myenteric ganglia, to submucosal ganglia, or directly to the epithelium, and play an important role in regulating and patterning gut motility.Gastrointestinal Neural and Hormonal Signaling
Absence of normal esophageal peristalsisPeristalsisA movement, caused by sequential muscle contraction, that pushes the contents of the intestines or other tubular organs in one direction.Gastrointestinal Motility
Anatomy and physiology[1,9]
EsophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy:
Made up of an outer longitudinal muscle layer and an inner circular muscle layer
Circular muscle fibers: allow peristalsisPeristalsisA movement, caused by sequential muscle contraction, that pushes the contents of the intestines or other tubular organs in one direction.Gastrointestinal Motility
Upper ⅓ of esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy: predominantly skeletal musclesSkeletal musclesA subtype of striated muscle, attached by tendons to the skeleton. Skeletal muscles are innervated and their movement can be consciously controlled. They are also called voluntary muscles.Muscle Tissue: Histology
Lower ⅔ of esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy: Smooth musclesSmooth musclesUnstriated and unstriped muscle, one of the muscles of the internal organs, blood vessels, hair follicles, etc. Contractile elements are elongated, usually spindle-shaped cells with centrally located nuclei. Smooth muscle fibers are bound together into sheets or bundles by reticular fibers and frequently elastic nets are also abundant.Muscle Tissue: Histology become more dominant from the middle to the distal esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy.
Myenteric plexusMyenteric plexusOne of two ganglionated neural networks which together form the enteric nervous system. The myenteric (Auerbach’s) plexus is located between the longitudinal and circular muscle layers of the gut. Its neurons project to the circular muscle, to other myenteric ganglia, to submucosal ganglia, or directly to the epithelium, and play an important role in regulating and patterning gut motility.Gastrointestinal Neural and Hormonal Signaling (Auerbach plexusAuerbach plexusOne of two ganglionated neural networks which together form the enteric nervous system. The myenteric (Auerbach’s) plexus is located between the longitudinal and circular muscle layers of the gut. Its neurons project to the circular muscle, to other myenteric ganglia, to submucosal ganglia, or directly to the epithelium, and play an important role in regulating and patterning gut motility.Gastrointestinal Neural and Hormonal Signaling):
Group of ganglia between the circular and longitudinal muscle layers
Part of the enteric nervous systemEnteric nervous systemTwo ganglionated neural plexuses in the gut wall which form one of the three major divisions of the autonomic nervous system. The enteric nervous system innervates the gastrointestinal tract, the pancreas, and the gallbladder. It contains sensory neurons, interneurons, and motor neurons. Thus the circuitry can autonomously sense the tension and the chemical environment in the gut and regulate blood vessel tone, motility, secretions, and fluid transport. The system is itself governed by the central nervous system and receives both parasympathetic and sympathetic innervation.Autonomic Nervous System: Anatomy
Function: controls the peristalsisPeristalsisA movement, caused by sequential muscle contraction, that pushes the contents of the intestines or other tubular organs in one direction.Gastrointestinal Motility of the gastrointestinal tract
Type of neuronsNeuronsThe basic cellular units of nervous tissue. Each neuron consists of a body, an axon, and dendrites. Their purpose is to receive, conduct, and transmit impulses in the nervous system.Nervous System: Histology or ganglion cellsGanglion CellsThe Visual Pathway and Related Disorders in the myenteric plexusMyenteric plexusOne of two ganglionated neural networks which together form the enteric nervous system. The myenteric (Auerbach’s) plexus is located between the longitudinal and circular muscle layers of the gut. Its neurons project to the circular muscle, to other myenteric ganglia, to submucosal ganglia, or directly to the epithelium, and play an important role in regulating and patterning gut motility.Gastrointestinal Neural and Hormonal Signaling:
Excitatory: secrete acetylcholineAcetylcholineA neurotransmitter found at neuromuscular junctions, autonomic ganglia, parasympathetic effector junctions, a subset of sympathetic effector junctions, and at many sites in the central nervous system.Receptors and Neurotransmitters of the CNS → muscle contraction
Inhibitory: secrete nitrous oxideNitrous oxideNitrogen oxide (N2O). A colorless, odorless gas that is used as an anesthetic and analgesic. High concentrations cause a narcotic effect and may replace oxygen, causing death by asphyxia.Inhaled Anesthetics and vasoactive peptide → muscle relaxation
Epidemiology[1,4,7,10]
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency: 2–3 cases per 100,000 individuals
PrevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency: approximately 10–30 cases per 100,000 individuals
Seen mostly in adults between 25 and 60 years of age
Caused by diseases that lead to esophageal abnormalities, similar to primary achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia
MalignancyMalignancyHemothorax (esophageal, gastric, or other extraesophageal cancers) by massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast effect or as part of paraneoplastic syndrome
Chagas diseaseChagas diseaseInfection with the protozoan parasite trypanosoma cruzi, a form of trypanosomiasis endemic in central and south america. It is named after the brazilian physician carlos chagas, who discovered the parasite. Infection by the parasite (positive serologic result only) is distinguished from the clinical manifestations that develop years later, such as destruction of parasympathetic ganglia; chagas cardiomyopathy; and dysfunction of the esophagus or colon.Trypanosoma cruzi/Chagas disease:
Infection with the parasite Trypanosoma cruziTrypanosoma cruziChagas disease is an infection caused by the American trypanosome Trypanosoma cruzi. This parasitic protozoan is transmitted in the feces of reduviid bugs in South and Central America. Acute infection may present with inflammation at the inoculation site (chagoma), fever, and lymphadenopathy. Untreated, chronic infection can progress to severe complications.Trypanosoma cruzi/Chagas disease
Commonly found in South and Central America
Infiltrative disorders: amyloidosisAmyloidosisAmyloidosis is a disease caused by abnormal extracellular tissue deposition of fibrils composed of various misfolded low-molecular-weight protein subunits. These proteins are frequently byproducts of other pathological processes (e.g., multiple myeloma). Amyloidosis, sarcoidosisSarcoidosisSarcoidosis is a multisystem inflammatory disease that causes noncaseating granulomas. The exact etiology is unknown. Sarcoidosis usually affects the lungs and thoracic lymph nodes, but it can also affect almost every system in the body, including the skin, heart, and eyes, most commonly. Sarcoidosis
Genetic diseases: neurofibromatosis, multiple endocrine neoplasia type 2BMultiple endocrine neoplasia type 2bSimilar to MEN2a, it is also caused by mutations of the MEN2 gene, also known as the ret proto-oncogene. Its clinical symptoms include medullary carcinoma of thyroid gland and pheochromocytoma of adrenal medulla (50%). Unlike MEN2a, MEN2b does not involve parathyroid neoplasms. It can be distinguished from MEN2a by its neural abnormalities such as mucosal neuromas on eyelids; lip; and tongue, and ganglioneuromatosis of gastrointestinal tract leading to megacolon. It is an autosomal dominant inherited disease.Multiple Endocrine Neoplasia, Fabry diseaseFabry diseaseFabry disease (FD), also known as Anderson-Fabry disease, is an X-linked recessive lysosomal storage disorder and the 2nd most common of the lysosomal storage disorders. Fabry disease is caused by a deficiency in the alpha-galactosidase enzyme (alpha-Gal A), resulting in the accumulation of the glycosphingolipid globotriaosylceramide (Gb3) in lysosomes. Fabry Disease, Allgrove syndrome
Others: eosinophilic esophagitisEosinophilic esophagitisChronic esophagitis characterized by esophageal mucosal eosinophilia. It is diagnosed when an increase in eosinophils are present over the entire esophagus. The reflux symptoms fail to respond to proton pump inhibitors treatment, unlike in gastroesophageal reflux disease. The symptoms are associated with ige-mediated hypersensitivity to food or inhalant allergens.Esophagitis, juvenile Sjögren syndromeSjögren SyndromeRheumatoid Arthritis, chronic idiopathicIdiopathicDermatomyositisintestinal pseudo-obstructionIntestinal pseudo-obstructionA type of ileus, a functional not mechanical obstruction of the intestines. This syndrome is caused by a large number of disorders involving the smooth muscles or the nervous system.Large Bowel Obstruction
Degeneration of Auerbach’s plexus, where there is selective loss of inhibitory ganglion cellsGanglion CellsThe Visual Pathway and Related Disorders in the distal esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy
Unopposed excitatory activity → failure of smooth muscle relaxation at LES → increase in LES pressure → progressive loss of peristaltic function
Proposed factors that contribute to the pathogenesis[3,9,10]
Genetic predisposition
AchalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia is associated with genetic mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations (Allgrove’s syndrome).
Familial cases point to a possible inherited pattern.
Viral infection
Varicella zoster, measlesMeaslesMeasles (also known as rubeola) is caused by a single-stranded, linear, negative-sense RNA virus of the family Paramyxoviridae. It is highly contagious and spreads by respiratory droplets or direct-contact transmission from an infected person. Typically a disease of childhood, measles classically starts with cough, coryza, and conjunctivitis, followed by a maculopapular rash. Measles Virus, and Herpes simplexHerpes SimplexA group of acute infections caused by herpes simplex virus type 1 or type 2 that is characterized by the development of one or more small fluid-filled vesicles with a raised erythematous base on the skin or mucous membrane. It occurs as a primary infection or recurs due to a reactivation of a latent infection.Congenital TORCH Infections (type 1Type 1Spinal Muscular Atrophy) virusVirusViruses are infectious, obligate intracellular parasites composed of a nucleic acid core surrounded by a protein capsid. Viruses can be either naked (non-enveloped) or enveloped. The classification of viruses is complex and based on many factors, including type and structure of the nucleoid and capsid, the presence of an envelope, the replication cycle, and the host range. VirologyantibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions have been noted in affected patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship.
A causal relationship, however, has not been established.
InflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation and autoimmune process
AutoantibodiesAutoantibodiesAntibodies that react with self-antigens (autoantigens) of the organism that produced them.Blotting Techniques to enteric neuronsNeuronsThe basic cellular units of nervous tissue. Each neuron consists of a body, an axon, and dendrites. Their purpose is to receive, conduct, and transmit impulses in the nervous system.Nervous System: Histology have been found in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia.
In affected esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy: Inflammatory T-cell infiltrates surround the inhibitory neuronsNeuronsThe basic cellular units of nervous tissue. Each neuron consists of a body, an axon, and dendrites. Their purpose is to receive, conduct, and transmit impulses in the nervous system.Nervous System: Histology, with relative sparing of the excitatory neuronsNeuronsThe basic cellular units of nervous tissue. Each neuron consists of a body, an axon, and dendrites. Their purpose is to receive, conduct, and transmit impulses in the nervous system.Nervous System: Histology.
Clinical Presentation and Complications
Clinical presentation[3,4,9]
Insidious onset
DysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia to solids and liquids
Retrosternal painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Increased risk of esophageal cancerEsophageal cancerEsophageal cancer is 1 of the most common causes of cancer-related deaths worldwide. Nearly all esophageal cancers are either adenocarcinoma (commonly affecting the distal esophagus) or squamous cell carcinoma (affecting the proximal two-thirds of the esophagus). Esophageal Cancer
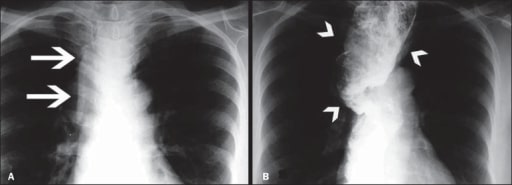
Image of megaesophagus (loss of esophageal motility and diffuse esophageal dilation) A: Posteroanterior (PA) chest X-ray showing widening of the superior mediastinum (arrows) B: Barium swallow study demonstrating a dilated and tortuous esophagus (arrowheads)
Image: “Grade IV megaesophagus” by US National Library of Medicine. License: CC BY 4.0
Diagnostic testing for achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia is indicated in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with:
DysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia (and other symptoms as above)
Symptoms of gastroesophageal reflux diseaseGastroesophageal Reflux DiseaseGastroesophageal reflux disease (GERD) occurs when the stomach acid frequently flows back into the esophagus. This backwash (acid reflux) can irritate the lining of the esophagus, causing symptoms such as retrosternal burning pain (heartburn). Gastroesophageal Reflux Disease (GERD) (GERDGERDGastroesophageal reflux disease (GERD) occurs when the stomach acid frequently flows back into the esophagus. This backwash (acid reflux) can irritate the lining of the esophagus, causing symptoms such as retrosternal burning pain (heartburn). Gastroesophageal Reflux Disease (GERD)) unresponsive to proton-pump inhibitor treatment after 4 weeks
Endoscopic findings (if done for other reasons):
Retained food in the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy
ResistanceResistancePhysiologically, the opposition to flow of air caused by the forces of friction. As a part of pulmonary function testing, it is the ratio of driving pressure to the rate of air flow.Ventilation: Mechanics of Breathing to passage of the endoscope
High-resolution esophageal manometryManometryMeasurement of the pressure or tension of liquids or gases with a manometer.Achalasia[4,7]
Test of choice to diagnose achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia:
Diagnostic if there is incomplete relaxation of the esophagogastric junctionEsophagogastric junctionThe area covering the terminal portion of esophagus and the beginning of stomach at the cardiac orifice.Esophagus: Anatomy (EGJ) and absence of organized peristalsisPeristalsisA movement, caused by sequential muscle contraction, that pushes the contents of the intestines or other tubular organs in one direction.Gastrointestinal Motility
If manometryManometryMeasurement of the pressure or tension of liquids or gases with a manometer.Achalasia is normal, achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia is ruled out.
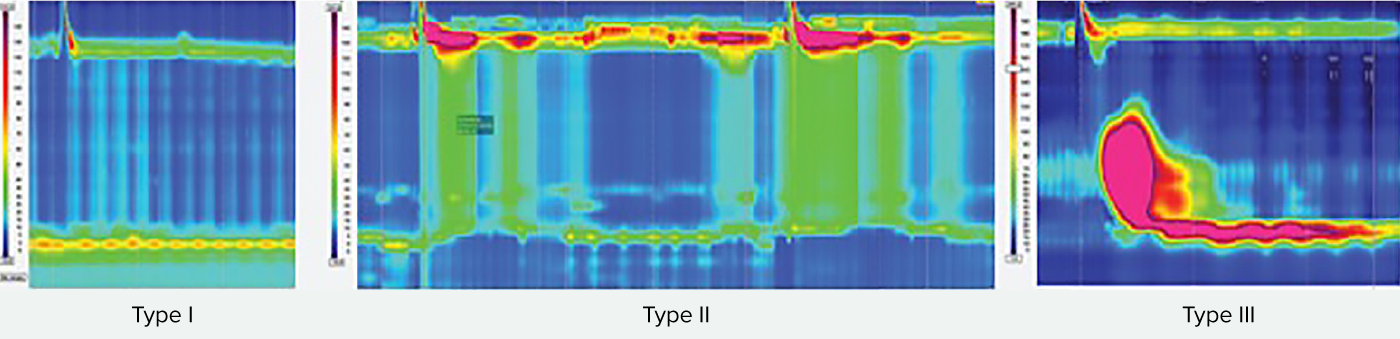
Pressure is represented by color: ↑ intensity of color = ↑ pressure:
Demonstrates:
Resting pressure of the EGJ
Swallowing-triggered esophageal activity
Chicago classification: tool to define relevant phenotypes to guide treatment:
Type I classic achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia (due to aganglionosis): 100% failed peristalsisPeristalsisA movement, caused by sequential muscle contraction, that pushes the contents of the intestines or other tubular organs in one direction.Gastrointestinal Motility in the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy (poor esophageal emptying)
Type II achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia (less aganglionosis): intermittent panesophageal pressurization without proper peristalsisPeristalsisA movement, caused by sequential muscle contraction, that pushes the contents of the intestines or other tubular organs in one direction.Gastrointestinal Motility
Type III achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia (spastic distal contractions): imbalance of excitatory and inhibitory influence, mostly intact ganglion cellsGanglion CellsThe Visual Pathway and Related Disorders → prematurePrematureChildbirth before 37 weeks of pregnancy (259 days from the first day of the mother’s last menstrual period, or 245 days after fertilization).Necrotizing Enterocolitis or spastic contractions which are not coordinated → abnormal peristalsisPeristalsisA movement, caused by sequential muscle contraction, that pushes the contents of the intestines or other tubular organs in one direction.Gastrointestinal Motility
All types exhibit impaired EGJ relaxation with swallowing.
Type I: upper esophageal sphincter relaxes, but there is 100% failure of contractions and no esophageal pressurization (absent peristalsis)
Type II: panesophageal pressurization in at least 20% of swallows
Type III: preserved fragments of distal peristalsis or premature spastic contractions for at least 20% of swallows
Image: “Achalasia types” by US National Library of Medicine. License: CC BY 4.0, edited by Lecturio.
Other diagnostic testsDiagnostic testsDiagnostic tests are important aspects in making a diagnosis. Some of the most important epidemiological values of diagnostic tests include sensitivity and specificity, false positives and false negatives, positive and negative predictive values, likelihood ratios, and pre-test and post-test probabilities. Epidemiological Values of Diagnostic Tests[2,4,7]
Performed if manometryManometryMeasurement of the pressure or tension of liquids or gases with a manometer.Achalasia is equivocal
If any of the following findings is noted, then endoscopic ultrasonography with fine-needle aspiration biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma is indicated.
Esophageal dilation terminating in a “beak-like” narrowing (dilated esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy due to lack of peristalsisPeristalsisA movement, caused by sequential muscle contraction, that pushes the contents of the intestines or other tubular organs in one direction.Gastrointestinal Motility)
Narrow EGJ
Aperistalsis
Delayed barium emptying
If normal, achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia is unlikely (but up to 30% false negatives)
Upper GI endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD): indicated in all patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia to exclude malignancyMalignancyHemothorax
Endoscopic ultrasonography:
Evaluates esophageal wall thickness
Significant or asymmetric wall thickening is suspicious for malignancyMalignancyHemothorax.
If barium swallowBarium SwallowImaging of the Intestines or endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD) shows suspicious features (e.g., significant or asymmetric wall thickening, especially in older patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship), then EUS with fine-needle aspiration is indicated to rule out malignancyMalignancyHemothorax.
EndoFLIP (functional lumen imaging probeProbeA device placed on the patient’s body to visualize a targetUltrasound (Sonography)):
May be performed if other tests are equivocal, but a high clinical suspicion remains
ProbeProbeA device placed on the patient’s body to visualize a targetUltrasound (Sonography) passes through the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy and displays the diameter of esophageal segments.
Helps assess esophageal emptying by the distensibility of the EGJ
AchalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia = low distensibility
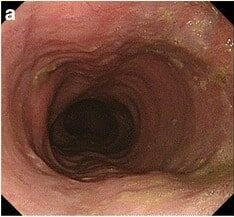
Esophagogastroduodenoscopy showcasing a dilated esophagus with food residue in a patient presenting with achalasia
Image: “Gastrointestinal endoscopy findings” by US National Library of Medicine. License: CC BY 4.0
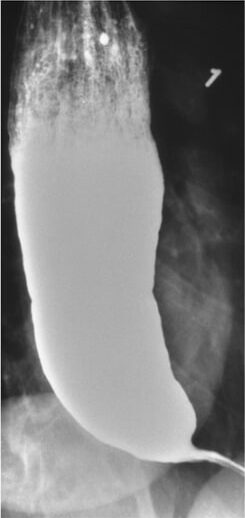
Achalasia seen on a barium swallow study: Narrowing is seen at the distal esophagus (“bird’s beak”) due to inadequate relaxation of the lower esophageal sphincter.
Image: “Barium swallow” by Department of Internal Medicine, Nashville, TN, USA. License: CC BY 4.0
Management
Management guidelines may vary depending on practice location. The following information is based on US and UK guidelines and literature.
The loss of ganglion cellsGanglion CellsThe Visual Pathway and Related Disorders is irreversible in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia; treatment is aimed at decreasing lower esophageal sphincterLower Esophageal SphincterEsophagus: AnatomyhypertonicityHypertonicityVolume Depletion and Dehydration and improving esophageal emptying. Among the types of achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia:
Type II: best response to treatment options
Type III: most difficult to manage
Management options[4–8,11]
Pneumatic dilation (PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease) of thelower esophageal sphincterLower Esophageal SphincterEsophagus: Anatomy:
Risk of esophageal perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis; patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship must also be surgical candidates, in case perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis needing repair occurs (approximately 2%)
For type I or type II achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia; equally effective to laparoscopic Heller myotomyHeller myotomySurgical incision of the lower esophageal sphincter near the cardia often used to treat esophageal achalasia.Achalasia
Provides good to excellent symptom relief in 50%–93% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
Reassessment is needed in 4–6 weeks.
Predictors of favorable response:
Age > 45
Female sexSexThe totality of characteristics of reproductive structure, functions, phenotype, and genotype, differentiating the male from the female organism.Gender Dysphoria
Narrow, nondilated esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy
Lower esophageal sphincterLower Esophageal SphincterEsophagus: Anatomy pressure < 10 mm Hg after PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease
No evidence to support:
The necessity of routine gastrografinGastrografinComputed Tomography (CT) esophagography after PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease (per ACG) unless there are symptoms of perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
The use of PPIs as maintenance therapy after the procedure unless symptomatic or positive 24-hour pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance monitoring
Laparoscopic Heller myotomyHeller myotomySurgical incision of the lower esophageal sphincter near the cardia often used to treat esophageal achalasia.Achalasia (LHM):
Preferred initial therapy for type I or type II
More effective in Type II (92%) and Type I (81%) achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia than Type III (71%)
Risk of esophageal and gastric perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis
Simultaneous fundoplication is recommended to reduce the rate of GERDGERDGastroesophageal reflux disease (GERD) occurs when the stomach acid frequently flows back into the esophagus. This backwash (acid reflux) can irritate the lining of the esophagus, causing symptoms such as retrosternal burning pain (heartburn). Gastroesophageal Reflux Disease (GERD) after myotomy.
Efficacy decreases after more extended follow-up periods.
Good to excellent symptom relief in about:
89% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship at 6 months
57% at 6 years
Peroral endoscopic myotomy (POEM):
Longer myotomy: should include 6 cm into the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy and 2–3 cm into the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy from the GEJ
Procedure of choice for type III achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia
Higher incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency of GERDGERDGastroesophageal reflux disease (GERD) occurs when the stomach acid frequently flows back into the esophagus. This backwash (acid reflux) can irritate the lining of the esophagus, causing symptoms such as retrosternal burning pain (heartburn). Gastroesophageal Reflux Disease (GERD) than LHM or PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease
Higher success rate at 2 years than with pneumatic dilation[6]
Appropriate for persistent or recurrent symptoms after LHM
Botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism injection (BTI) into lower esophageal sphincterLower Esophageal SphincterEsophagus: Anatomy:
Botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism is injected to block the release of acetylcholineAcetylcholineA neurotransmitter found at neuromuscular junctions, autonomic ganglia, parasympathetic effector junctions, a subset of sympathetic effector junctions, and at many sites in the central nervous system.Receptors and Neurotransmitters of the CNS from excitatory ganglions → ↓ LES tone
Requires retreatment within 6–12 months; repeat injections are less effective
Reserved for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who are not surgical candidates or as a bridge to more effective therapies (surgery or endoscopic dilation)
Limited application in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship under 50
Pharmacologic options:
Least benefit
Considered only in poor surgical candidates and for those who fail botulinum injections
International Guidelines state there is no convincing evidence for symptomatic relief with:
NitratesNitratesNitrates are a class of medications that cause systemic vasodilation (veins > arteries) by smooth muscle relaxation. Nitrates are primarily indicated for the treatment of angina, where preferential venodilation causes pooling of blood, decreased preload, and ultimately decreased myocardial O2 demand.Nitrates
CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes channel blockers
Phosphodiesterase inhibitorsPhosphodiesterase inhibitorsPhosphodiesterase (PDE) inhibitors are a group of drugs that act by inhibiting PDE enzymes. Phosphodiesterase inhibitors have various mechanisms of action depending on the subtype of PDE targeted, but their main action is increasing the amount of intracellular cAMP or cGMP, which in turn results in physiologic effects such as reducing inflammation, promoting smooth muscle relaxation, and vasodilation.Phosphodiesterase Inhibitors
ACG guidelines still consider medications for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who are not candidates for definitive therapies (PDPDParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease, LHM, or POEM)
Insufficient evidence for retrievable stents and intrasphincteric injection with ethanolamine oleate or polidocanol
Post-therapy assessment[4,7]
Eckardt score: simple measure to assist achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia outcome
Symptom improvement is the best measure of success after treatment.
Should be integrated with objective measures such as manometryManometryMeasurement of the pressure or tension of liquids or gases with a manometer.Achalasia
Used in both initial and follow-up assessments
Components:
DysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia
Retrosternal painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Weight lossWeight lossDecrease in existing body weight.Bariatric Surgery (a sign of a patient’s inability to maintain adequate nutrition)
Each symptom is attributed 0–3 points:
≤ 3: indicates a good outcome
> 3: indicates a poor outcome (requires further evaluation)
Esophageal spasm: also presents with dysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia to solids and liquids but is associated with sudden onset of chest painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways that is not exertion-related. There are 2 types of this condition: distal esophageal spasm and hypercontractile esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy. ManometryManometryMeasurement of the pressure or tension of liquids or gases with a manometer.Achalasia shows characteristic esophageal contractions with normal relaxation of the EGJ.
Gastroesophageal reflux diseaseGastroesophageal Reflux DiseaseGastroesophageal reflux disease (GERD) occurs when the stomach acid frequently flows back into the esophagus. This backwash (acid reflux) can irritate the lining of the esophagus, causing symptoms such as retrosternal burning pain (heartburn). Gastroesophageal Reflux Disease (GERD) (GERDGERDGastroesophageal reflux disease (GERD) occurs when the stomach acid frequently flows back into the esophagus. This backwash (acid reflux) can irritate the lining of the esophagus, causing symptoms such as retrosternal burning pain (heartburn). Gastroesophageal Reflux Disease (GERD)): symptoms of heartburnHeartburnSubsternal pain or burning sensation, usually associated with regurgitation of gastric juice into the esophagus.Gastroesophageal Reflux Disease (GERD) and regurgitationRegurgitationGastroesophageal Reflux Disease (GERD) caused by the reflux of stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy contents. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship usually complain of a burning epigastric painEpigastric painMallory-Weiss Syndrome (Mallory-Weiss Tear) radiating up the chest, with a sour or metallic taste in the mouth. GERDGERDGastroesophageal reflux disease (GERD) occurs when the stomach acid frequently flows back into the esophagus. This backwash (acid reflux) can irritate the lining of the esophagus, causing symptoms such as retrosternal burning pain (heartburn). Gastroesophageal Reflux Disease (GERD) symptoms are due to inappropriate relaxation of the LES. Dietary and lifestyle modification plus acid-reducing therapy with histamine 2 receptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors blockers (H2 blockers) or proton-pump inhibitors (PPIs) are used to control symptoms.
SystemicsclerosisSclerosisA pathological process consisting of hardening or fibrosis of an anatomical structure, often a vessel or a nerve.Wilms Tumor (sclerodermaSclerodermaScleroderma (systemic sclerosis) is an autoimmune condition characterized by diffuse collagen deposition and fibrosis. The clinical presentation varies from limited skin involvement to diffuse involvement of internal organs. Scleroderma): presents with dysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia to solids and liquids at the onset, accompanied by findings of skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions thickening and hardening (sclerosisSclerosisA pathological process consisting of hardening or fibrosis of an anatomical structure, often a vessel or a nerve.Wilms Tumor) and specific serum autoantibodiesAutoantibodiesAntibodies that react with self-antigens (autoantigens) of the organism that produced them.Blotting Techniques. The lower esophageal sphincterLower Esophageal SphincterEsophagus: Anatomy is weak or incompetent in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with sclerodermaSclerodermaScleroderma (systemic sclerosis) is an autoimmune condition characterized by diffuse collagen deposition and fibrosis. The clinical presentation varies from limited skin involvement to diffuse involvement of internal organs. Scleroderma, so manometryManometryMeasurement of the pressure or tension of liquids or gases with a manometer.Achalasia shows low or absent lower esophageal sphincterLower Esophageal SphincterEsophagus: Anatomy pressure.
Esophageal strictureStricturePrimary Sclerosing Cholangitis: narrowing of the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy that is frequently a sequela of gastroesophageal reflux. This narrowing can also result from malignancies. Esophageal strictureStricturePrimary Sclerosing Cholangitis presents with dysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia to solids, progressing to liquids. Barium swallowBarium SwallowImaging of the Intestines study shows a narrowed luminal diameter. Upper endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD) is performed for dual purposes, as it aids in diagnosis through visualization and biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma and also allows dilation when necessary for treatment.
Esophageal ring and web: thin structures that produce partial occlusion of the esophageal lumen. Plummer-Vinson syndromePlummer-Vinson syndromeA syndrome of dysphagia with iron-deficiency anemia that is due to congenital anomalies in the esophagus (such as cervical esophageal webs). It is known as patterson-kelly syndrome in the united kingdom.Iron Deficiency Anemia is a rare disease characterized by ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements deficiency anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types, dysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia, and esophageal webs. Presentation includes dysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia to solids. A Schatzki ringSchatzki ringDysphagia, the most common type of lower esophageal ring, is also associated with intermittent dysphagiaDysphagiaDysphagia is the subjective sensation of difficulty swallowing. Symptoms can range from a complete inability to swallow, to the sensation of solids or liquids becoming “stuck.” Dysphagia is classified as either oropharyngeal or esophageal, with esophageal dysphagia having 2 sub-types: functional and mechanical. Dysphagia to solids. Diagnosis is by barium swallowBarium SwallowImaging of the Intestines study and upper endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD).
Billing and Coding
Diagnosis Codes:
This code is used to diagnose achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia, a rare esophageal motilityEsophageal MotilityGastrointestinal Motility disorder characterized by the failure of the lower esophageal sphincterLower Esophageal SphincterEsophagus: Anatomy (LES) to relax, causing difficulty swallowingSwallowingThe act of taking solids and liquids into the gastrointestinal tract through the mouth and throat.Gastrointestinal Motility.
Coding System
Code
Description
ICD-10-CM
K22.0
AchalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia of cardia
SNOMED CT
235123001
AchalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia (disorder)
Evaluation & Workup:
This CPT code is for high-resolution esophageal manometryManometryMeasurement of the pressure or tension of liquids or gases with a manometer.Achalasia, the gold standard for diagnosing achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia. It measures the pressure and coordinationCoordinationCerebellar Disorders of muscle contractions in the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy.
Radiologic examination; esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy (barium swallowBarium SwallowImaging of the Intestines)
Procedures/Interventions:
These codes represent the primary treatments for achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia, which aim to disrupt the non-relaxing LES. This includes a Heller myotomyHeller myotomySurgical incision of the lower esophageal sphincter near the cardia often used to treat esophageal achalasia.Achalasia (surgical cutting of the muscle) and pneumatic dilation (endoscopic stretching).
Coding System
Code
Description
CPT
43279
LaparoscopyLaparoscopyLaparoscopy is surgical exploration and interventions performed through small incisions with a camera and long instruments. Laparotomy and Laparoscopy, surgical, esophagomyotomy (Heller type)
CPT
43249
Esophagoscopy, flexible, transoral; with balloon dilation (less than 30 mm diameter)
Complications:
This code is used to document a common complication of achalasiaAchalasiaAchalasia is a primary esophageal motility disorder that develops from the degeneration of the myenteric plexus. This condition results in impaired lower esophageal sphincter relaxation and absence of normal esophageal peristalsis. Patients typically present with dysphagia to solids and liquids along with regurgitation. Achalasia, aspiration pneumoniaAspiration pneumoniaA type of lung inflammation resulting from the aspiration of food, liquid, or gastric contents into the upper respiratory tract.Pneumonia, which occurs when retained food and liquid in the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy are inhaled into the lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy.
Falk GW, Katzka DA. (2019). Diseases of the esophagus. Chapter 129 of Crow MK, et al. (Eds.), Goldman-Cecil Medicine, 26th ed., vol 1, pp. 860–870.
Pasricha PJ. (2019). GI endoscopy. Chapter 125 of Crow MK, et al. (Eds.), Goldman-Cecil Medicine, 26th ed., vol 1, pp. 834–836.
Furuzawa-Carballeda J, et al. (2016). New insights into the pathophysiology of achalasia and implications for future treatment. World Journal of Gastroenterology 22(35):7892–7907. doi: 10.3748/wjg.v22.i35.7892
Vaezi MF, Pandolfino JE, Yadlapati RH, Greer KB, Kavitt RT. (2020). ACG clinical guidelines: diagnosis and management of achalasia. American Journal of Gastroenterology 115(9):1393-411. doi: 10.14309/ajg.0000000000000731
Werner YB, Hakanson B, et al. (2019). Endoscopic or surgical myotomy in patients with idiopathic achalasia. New England Journal of Medicine, 381(23):2219–2229. doi: 10.1056/NEJMoa1905380
Ponds FA, Fockens P, et al. (2019). Effect of peroral endoscopic myotomy vs pneumatic dilation on symptom severity and treatment outcomes among treatment-naive patients with achalasia: a randomized clinical trial. JAMA 322(2):134-144. doi: 10.1001/jama.2019.8859
Zaninotto G, Bennett C, et al. (2018). The 2018 ISDE achalasia guidelines. Diseases of the Esophagus 31(9). https://doi.org/10.1093/dote/doy071