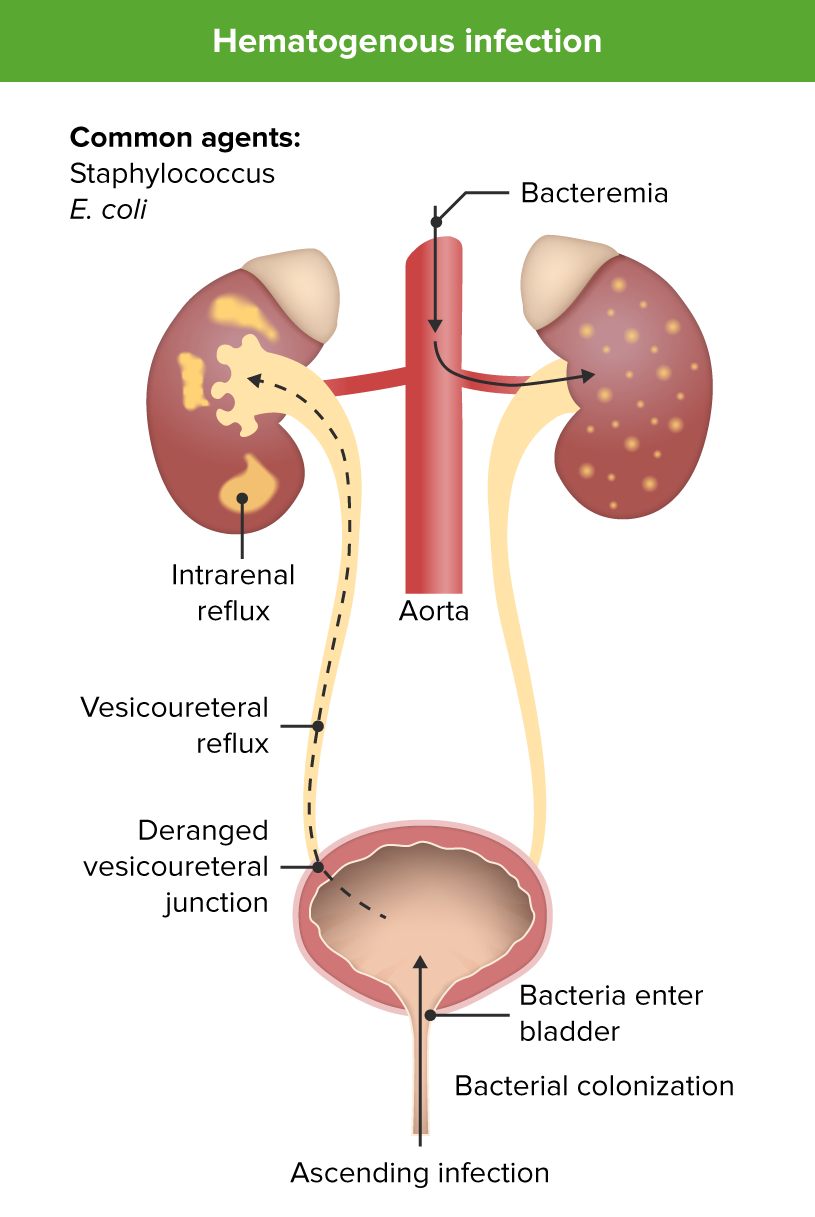
Urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: AnatomyinfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease (UTIs) are commonly seen in children. Urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: AnatomyinfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease may present as cystitisCystitisInflammation of the urinary bladder, either from bacterial or non-bacterial causes. Cystitis is usually associated with painful urination (dysuria), increased frequency, urgency, and suprapubic pain.Urinary Tract Infections (UTIs), pyelonephritisPyelonephritisPyelonephritis is infection affecting the renal pelvis and the renal parenchyma. This condition arises mostly as a complication of bladder infection that ascends to the upper urinary tract. Pyelonephritis can be acute or chronic (which results from persistent or chronic infections). Typical acute symptoms are flank pain, fever, and nausea with vomiting. TPyelonephritis and Perinephric Abscess, or asymptomatic bacteriuria, and their clinical presentation may vary widely depending on the age of the patient. Fecal E. coli is the most common pathogen. Routes of infection may be ascending (most common) or hematogenousHematogenousHepatocellular Carcinoma (HCC) and Liver Metastases. Urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy infection is suspected based on lower UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs) symptoms (dysuriaDysuriaPainful urination. It is often associated with infections of the lower urinary tract.Urinary Tract Infections (UTIs), frequency) or upper UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs) symptoms (feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever) and positive urinalysis findings. Urine cultureUrine cultureUrinary Tract Infections (UTIs) confirms the diagnosis. Most cases respond to oral antibiotics. Further investigation through imaging and, at times, hospital admission is required in refractory or recurrent cases.
Aurinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy infection (UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)) is an infection (most commonly bacterial, but, rarely, also viral and fungal) of any part of the urinary system, including the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy, bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess, uretersUretersOne of a pair of thick-walled tubes that transports urine from the kidney pelvis to the urinary bladder.Urinary Tract: Anatomy, or kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy.
Classification
PyelonephritisPyelonephritisPyelonephritis is infection affecting the renal pelvis and the renal parenchyma. This condition arises mostly as a complication of bladder infection that ascends to the upper urinary tract. Pyelonephritis can be acute or chronic (which results from persistent or chronic infections). Typical acute symptoms are flank pain, fever, and nausea with vomiting. TPyelonephritis and Perinephric Abscess (upper UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)): infection involving the uretersUretersOne of a pair of thick-walled tubes that transports urine from the kidney pelvis to the urinary bladder.Urinary Tract: Anatomy and kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy
CystitisCystitisInflammation of the urinary bladder, either from bacterial or non-bacterial causes. Cystitis is usually associated with painful urination (dysuria), increased frequency, urgency, and suprapubic pain.Urinary Tract Infections (UTIs) (lower UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)): infection of the urinary bladderUrinary BladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters (ureter), and is held there until urination.Urinary Tract: Anatomy without renal involvement
PrevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency of UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs):
Age dependent: Infants (boys < 1; girls < 4) have a higher prevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency of UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs) than older children.
GenderGenderGender Dysphoria dependent: Male:female ratio is 1:2 in the 1st year, increases to 1:10 beyond 1–2 years.
Anatomy dependent: PrevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency is 8 times lower in circumcised boys than in uncircumcised boys.
Ethnicity dependent: White children have a higher prevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency than Black children.
Risk factors
Acquired:
Recent antibiotic therapy
Sexual activity (consider in adolescents)
Bowel dysfunction (pediatric constipationPediatric constipationConstipation is a common complaint in children that is relatively defined for individual age groups based on the frequency and difficulty of defecation and stool consistency. The majority of constipation cases are functional or non-organic. Clinical presentation may vary, from insufficient evacuation noted by the parents, to complaints of abdominal pain, to secondary incontinence.Pediatric Constipation)
Urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy structural anomalies leading to obstruction
Dysfunctional voiding (neurogenic bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess)
GeneticsGeneticsGenetics is the study of genes and their functions and behaviors.Basic Terms of Genetics (children with 1st-degree relatives with a history of pediatric UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs) are more likely to have UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs))
Etiology and Pathophysiology
Etiology
Bacterial:
Escherichia coliEscherichia coliThe gram-negative bacterium Escherichia coli is a key component of the human gut microbiota. Most strains of E. coli are avirulent, but occasionally they escape the GI tract, infecting the urinary tract and other sites. Less common strains of E. coli are able to cause disease within the GI tract, most commonly presenting as abdominal pain and diarrhea. Escherichia coli(75%–90%)
KlebsiellaKlebsiellaKlebsiella are encapsulated gram-negative, lactose-fermenting bacilli. They form pink colonies on MacConkey agar due to lactose fermentation. The main virulence factor is a polysaccharide capsule. Klebsiella pneumoniae is the most important pathogenic species.Klebsiella
ProteusProteusProteus spp. are gram-negative, facultatively anaerobic bacilli. Different types of infection result from Proteus, but the urinary tract is the most common site. The majority of cases are caused by Proteus mirabilis (P. mirabilis). The bacteria are part of the normal intestinal flora and are also found in the environment. Proteus
EnterococcusEnterococcusEnterococcus is a genus of oval-shaped gram-positive cocci that are arranged in pairs or short chains. Distinguishing factors include optochin resistance and the presence of pyrrolidonyl arylamidase (PYR) and Lancefield D antigen. Enterococcus is part of the normal flora of the human GI tract.Enterococcus faecalis
Staphylococcus saprophyticusStaphylococcus saprophyticusA species of gram-positive bacteria in the family staphylococcaceae. It commonly causes urinary tract infections in humans.Staphylococcus
Group BstreptococcusStreptococcusStreptococcus is one of the two medically important genera of gram-positive cocci, the other being Staphylococcus. Streptococci are identified as different species on blood agar on the basis of their hemolytic pattern and sensitivity to optochin and bacitracin. There are many pathogenic species of streptococci, including S. pyogenes, S. agalactiae, S. pneumoniae, and the viridans streptococci.Streptococcus(neonates)
PseudomonasPseudomonasPseudomonas is a non-lactose-fermenting, gram-negative bacillus that produces pyocyanin, which gives it a characteristic blue-green color. Pseudomonas is found ubiquitously in the environment, as well as in moist reservoirs, such as hospital sinks and respiratory equipment. Pseudomonas
Fungal (especially with instrumentation):
CandidaCandidaCandida is a genus of dimorphic, opportunistic fungi. Candida albicans is part of the normal human flora and is the most common cause of candidiasis. The clinical presentation varies and can include localized mucocutaneous infections (e.g., oropharyngeal, esophageal, intertriginous, and vulvovaginal candidiasis) and invasive disease (e.g., candidemia, intraabdominal abscess, pericarditis, and meningitis). Candida/Candidiasis spp
Asperigillus spp
CryptococcusCryptococcusCryptococcosis is an opportunistic, fungal infection caused by the Cryptococcus species. The principal pathogens in humans are C. neoformans (primary) and C. gattii. Cryptococcus neoformans is typically found in pigeon droppings and acquired by inhaling dust from contaminated soil. The majority of affected patients are immunocompromised. Cryptococcus/Cryptococcosis neoformans
Viral: adenovirusAdenovirusAdenovirus (member of the family Adenoviridae) is a nonenveloped, double-stranded DNA virus. Adenovirus is transmitted in a variety of ways, and it can have various presentations based on the site of entry. Presentation can include febrile pharyngitis, conjunctivitis, acute respiratory disease, atypical pneumonia, and gastroenteritis. Adenovirus and other virusesVirusesMinute infectious agents whose genomes are composed of DNA or RNA, but not both. They are characterized by a lack of independent metabolism and the inability to replicate outside living host cells.Virology (seen in cystitisCystitisInflammation of the urinary bladder, either from bacterial or non-bacterial causes. Cystitis is usually associated with painful urination (dysuria), increased frequency, urgency, and suprapubic pain.Urinary Tract Infections (UTIs) with gross hematuriaHematuriaPresence of blood in the urine.Renal Cell Carcinoma)
Pathophysiology
Normal urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy anatomy and/or urinary dynamics:
Ascending infection
Uropathogens (most commonly fecal flora) colonize periurethral area → ascend to bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess via urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy
If pathogen reaches kidney via ureter → pyelonephritisPyelonephritisPyelonephritis is infection affecting the renal pelvis and the renal parenchyma. This condition arises mostly as a complication of bladder infection that ascends to the upper urinary tract. Pyelonephritis can be acute or chronic (which results from persistent or chronic infections). Typical acute symptoms are flank pain, fever, and nausea with vomiting. TPyelonephritis and Perinephric Abscess or upper UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)
Infection may occasionally enter blood → septicemia
Septicemia → UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)
Rarely seen, usually in immunocompromisedimmunocompromisedA human or animal whose immunologic mechanism is deficient because of an immunodeficiency disorder or other disease or as the result of the administration of immunosuppressive drugs or radiation.GastroenteritispatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
Abnormal urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy anatomy and/or urinary dynamics:
Stagnation of urine leads to pathogen growth and UTIs
Neurological abnormalities leading to delay in emptying
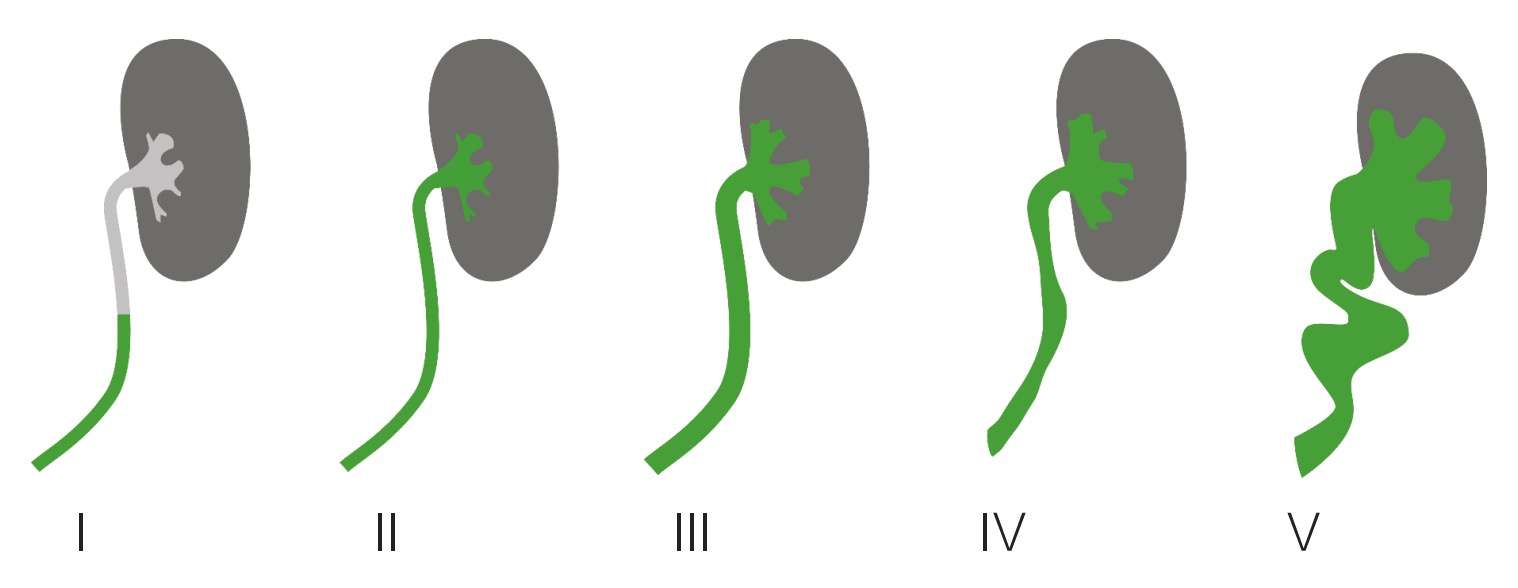
Vesicoureteral refluxVesicoureteral RefluxVesicoureteral reflux (VUR) is the retrograde flow of urine from the bladder into the upper urinary tract. Primary VUR often results from the incomplete closure of the ureterovesical junction, whereas secondary VUR is due to an anatomic or physiologic obstruction. Vesicoureteral Reflux (VUR): retrograde flowRetrograde flowVeins: Histology of urine from the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess along the uretersUretersOne of a pair of thick-walled tubes that transports urine from the kidney pelvis to the urinary bladder.Urinary Tract: Anatomy
Common and important cause of febrile UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs) leading to pyelonephritisPyelonephritisPyelonephritis is infection affecting the renal pelvis and the renal parenchyma. This condition arises mostly as a complication of bladder infection that ascends to the upper urinary tract. Pyelonephritis can be acute or chronic (which results from persistent or chronic infections). Typical acute symptoms are flank pain, fever, and nausea with vomiting. TPyelonephritis and Perinephric Abscess in children
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever (may be the sole symptom, especially feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever > 39℃ (101.2°F))
Irritability
Poor feeding
JaundiceJaundiceJaundice is the abnormal yellowing of the skin and/or sclera caused by the accumulation of bilirubin. Hyperbilirubinemia is caused by either an increase in bilirubin production or a decrease in the hepatic uptake, conjugation, or excretion of bilirubin. Jaundice
Presentation is similar to adults and clinical symptoms can be used to distinguish upper from lower UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs).
PyelonephritisPyelonephritisPyelonephritis is infection affecting the renal pelvis and the renal parenchyma. This condition arises mostly as a complication of bladder infection that ascends to the upper urinary tract. Pyelonephritis can be acute or chronic (which results from persistent or chronic infections). Typical acute symptoms are flank pain, fever, and nausea with vomiting. TPyelonephritis and Perinephric Abscess:
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways (abdominal, back, or flank)
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
DiarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea (occasionally)
CystitisCystitisInflammation of the urinary bladder, either from bacterial or non-bacterial causes. Cystitis is usually associated with painful urination (dysuria), increased frequency, urgency, and suprapubic pain.Urinary Tract Infections (UTIs):
Suprapubic painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and tenderness
Incontinence
Malodorous urine
HematuriaHematuriaPresence of blood in the urine.Renal Cell Carcinoma (caused by E. coli or adenovirusAdenovirusAdenovirus (member of the family Adenoviridae) is a nonenveloped, double-stranded DNA virus. Adenovirus is transmitted in a variety of ways, and it can have various presentations based on the site of entry. Presentation can include febrile pharyngitis, conjunctivitis, acute respiratory disease, atypical pneumonia, and gastroenteritis. Adenovirus)
Children 2–24 months: Decision is case dependent, based on height of feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever and risk factors.
Older children: only if symptoms are suggestive of UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)
How to obtain a sample:
Obtaining sterileSterileBasic Procedures urine is key to valid urinalysis results, but challenging with young children.
Toilet-trained children: Attempt clean catch (take care to avoid contamination with skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions flora).
Children 2–24 months without toilet training:
Place a bag over genital area (bag sample).
Catheterization or suprapubic aspiration may be necessary.
Urinalysis features
Urinalysis results may suggest UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs) but are not diagnostic alone.
Negative results in the presence of symptoms do not rule out UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs).
Nitrites and leukocyte esteraseLeukocyte esteraseKidney Function Tests usually positive with UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)
PyuriaPyuriaThe presence of white blood cells (leukocytes) in the urine. It is often associated with bacterial infections of the urinary tract. Pyuria without bacteriuria can be caused by tuberculosis, stones, or cancer.Urinary Tract Infections (UTIs) (leukocytesLeukocytesWhite blood cells. These include granular leukocytes (basophils; eosinophils; and neutrophils) as well as non-granular leukocytes (lymphocytes and monocytes).White Myeloid Cells: Histology in urine):
May be absent in UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)
SterileSterileBasic ProcedurespyuriaPyuriaThe presence of white blood cells (leukocytes) in the urine. It is often associated with bacterial infections of the urinary tract. Pyuria without bacteriuria can be caused by tuberculosis, stones, or cancer.Urinary Tract Infections (UTIs) (positive leukocytesLeukocytesWhite blood cells. These include granular leukocytes (basophils; eosinophils; and neutrophils) as well as non-granular leukocytes (lymphocytes and monocytes).White Myeloid Cells: Histology and negative culture) may be caused by:
Prior antibiotic therapy
Viral infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease, tuberculosisTuberculosisTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes. Tuberculosis, renal abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease
Urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy obstruction
InflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation outside the urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy
Interstitial nephritis
HematuriaHematuriaPresence of blood in the urine.Renal Cell Carcinoma (increased RBCsRBCsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology) may be seen.
Urinalyses suggestive of UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs) must be confirmed by urine cultureUrine cultureUrinary Tract Infections (UTIs).
Isolation of a single pathogen with one of the following criteria is diagnostic of UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs):
Colony count > 10,000 in a symptomatic child
Colony count > 50,000 from a suprapubic/catheter-obtained specimen
Colony count > 100,000 from a urine bag
Isolation of Lactobacillusspp., coagulase-negative staphylococciCoagulase-negative staphylococciStaphylococcus, and CorynebacteriumCorynebacteriumCorynebacteria are gram-positive, club-shaped bacilli. Corynebacteria are commonly isolated on tellurite or Loeffler’s media and have characteristic metachromatic granules. The major pathogenic species is Corynebacterium diphtheriae, which causes a severe respiratory infection called diphtheria.Corynebacteriumspp. are not suggestive of UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs) as these are normal skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions flora.
Blood culture
When to perform:
Very young children (< 2 months) who are at high risk for sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock
In suspected pyelonephritisPyelonephritisPyelonephritis is infection affecting the renal pelvis and the renal parenchyma. This condition arises mostly as a complication of bladder infection that ascends to the upper urinary tract. Pyelonephritis can be acute or chronic (which results from persistent or chronic infections). Typical acute symptoms are flank pain, fever, and nausea with vomiting. TPyelonephritis and Perinephric Abscess before antibiotic therapy
Imaging
Urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: AnatomyinfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease in children may be indicative of underlying renal anatomical abnormalities, so some must be further investigated with imaging.
Renal and bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess ultrasound (RBUS) should be performed:
After 1st febrile UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs) in all children 2–24 months
In all children with recurrent cases of UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)
Voiding cystourethrogram (VCUG): Dye visible on X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests is injected into the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess and urine flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure is visualized during voiding.
Goal is to confirm presence of vesicoureteral refluxVesicoureteral RefluxVesicoureteral reflux (VUR) is the retrograde flow of urine from the bladder into the upper urinary tract. Primary VUR often results from the incomplete closure of the ureterovesical junction, whereas secondary VUR is due to an anatomic or physiologic obstruction. Vesicoureteral Reflux (VUR).
Performed if:
Ultrasound findings suggestive of high-grade (III and above) VUR (majority of grade I or II VURs resolve spontaneously)
Evidence of obstruction, such as hydronephrosisHydronephrosisHydronephrosis is dilation of the renal collecting system as a result of the obstruction of urine outflow. Hydronephrosis can be unilateral or bilateral. Nephrolithiasis is the most common cause of hydronephrosis in young adults, while prostatic hyperplasia and neoplasm are seen in older patients. Hydronephrosis or scarringScarringInflammation
Recurrent febrile UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)
Late dimercaptosuccinic acid (DMSADMSAA mercaptodicarboxylic acid used as an antidote to heavy metal poisoning because it forms strong chelates with them.Metal Poisoning (Lead, Arsenic, Iron)) scan: no longer recommended by the American Academy of Pediatrics
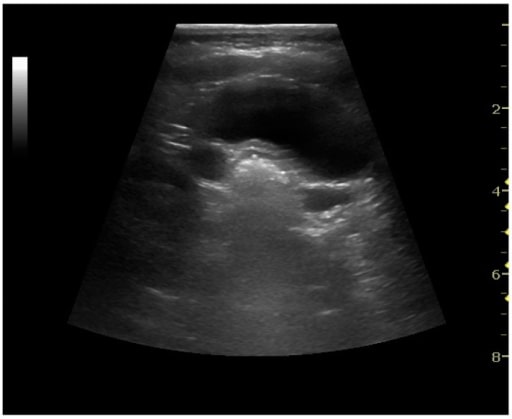
Bilateral dilatation of the ureters due to vesicoureteric reflux in a pediatric patient
Image: “Ultrasonography of the Kidney” by Department of Radiology, Copenhagen University Hospital, Blegdamsvej 9, Copenhagen 2100-DK, Denmark. License: CC BY 4.0
Management and Follow-up
Management
The main goal of treatment is prevention of renal complications, such as renal scarringScarringInflammation, hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension, and chronic kidney diseaseChronic Kidney DiseaseChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease.
Should only be started after urine samples for testing have been collected
Should only be started for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with high likelihood of UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs):
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever > 39℃ (101.2)
Known immune deficiency or renal anomaly
Septic appearance
Antibiotic choice:
Should be tailored to bacterial species and sensitivity whenever possible
Aimed at treating the most likely causative pathogen (E. coli)
PyelonephritisPyelonephritisPyelonephritis is infection affecting the renal pelvis and the renal parenchyma. This condition arises mostly as a complication of bladder infection that ascends to the upper urinary tract. Pyelonephritis can be acute or chronic (which results from persistent or chronic infections). Typical acute symptoms are flank pain, fever, and nausea with vomiting. TPyelonephritis and Perinephric Abscess
Admit to hospital if:
Septic
Dehydrated
Nauseous & vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
< 1 month with suspected UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)
< 2 months with febrile UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)
Outpatient: oral 3rd-generation cephalosporinsCephalosporinsCephalosporins are a group of bactericidal beta-lactam antibiotics (similar to penicillins) that exert their effects by preventing bacteria from producing their cell walls, ultimately leading to cell death. Cephalosporins are categorized by generation and all drug names begin with “cef-” or “ceph-.” Cephalosporins (cefixime)
Inpatient: IV ceftriaxoneCeftriaxoneA broad-spectrum cephalosporin antibiotic and cefotaxime derivative with a very long half-life and high penetrability to meninges, eyes and inner ears.Cephalosporins, cefotaximeCefotaximeSemisynthetic broad-spectrum cephalosporin.Cephalosporins, or ampicillinAmpicillinSemi-synthetic derivative of penicillin that functions as an orally active broad-spectrum antibiotic.Penicillins with an aminoglycoside (gentamicinGentamicinAminoglycosides)
FluoroquinolonesFluoroquinolonesFluoroquinolones are a group of broad-spectrum, bactericidal antibiotics inhibiting bacterial DNA replication. Fluoroquinolones cover gram-negative, anaerobic, and atypical organisms, as well as some gram-positive and multidrug-resistant (MDR) organisms. Fluoroquinolones are effective antibiotics, but are best avoided in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship < 17 years of age.
Renal abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease, perirenal abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease, or urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy obstruction: surgical or percutaneous drainagePercutaneous DrainageEchinococcus/Echinococcosis + antibiotics
Follow-up
Children with history of only one uncomplicated UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs) do not need follow-up.
Nephrologist follow-up is recommended for children with:
Recurrent UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)
Severe VUR (grade III to V)
Anatomical renal abnormalities
Neurological disfunction of the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess
Millner, R., M.D., & Becknell, Brian,M.D., PhD. (2019). Urinary tract infections. Pediatric Clinics of North America, 66(1), 1-13. doi://dx.doi.org/10.1016/j.pcl.2018.08.002
Jerardi, K. E., & Jackson, E. C. (2020). Urinary tract infections. In R. M. Kliegman MD, J. W. St Geme MD, N. J. Blum MD, Shah, Samir S., MD,MSCE, Tasker, Robert C., MBBS,MD & Wilson, Karen M., MD,MPH (Eds.), Nelson textbook of pediatrics (pp. 278-2795.e1) https://www.clinicalkey.es/#!/content/3-s2.0-B9780323529501005538
Gupta, K., & Trautner, B. W. (2018). Urinary tract infections, pyelonephritis, and prostatitis. In J. L. Jameson et al. (Eds.), Harrison’s principles of internal medicine. New York, NY: McGraw-Hill Education. accessmedicine.mhmedical.com/content.aspx?aid=1159153646
Robinson J. Antibiotic prophylaxis in vesicoureteral reflux: A practice revisited. Can Pharm J (Ott). 2013;146(2):84-87. doi:10.1177/1715163513481570
Create your free account or log in to continue reading!