The large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoidSigmoidA segment of the colon between the rectum and the descending colon.Volvulus segments), rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy and anal canal. The colon also contains many mucus-secreting glands to lubricate the stool passing through it. The colon receives its blood supply from colic branches of the superior and inferior mesenteric arteriesArteriesArteries are tubular collections of cells that transport oxygenated blood and nutrients from the heart to the tissues of the body. The blood passes through the arteries in order of decreasing luminal diameter, starting in the largest artery (the aorta) and ending in the small arterioles. Arteries are classified into 3 types: large elastic arteries, medium muscular arteries, and small arteries and arterioles. Arteries: Histology, which form an important anastomosis along the transverse colon. The colon is regulated by the ANSANSThe ans is a component of the peripheral nervous system that uses both afferent (sensory) and efferent (effector) neurons, which control the functioning of the internal organs and involuntary processes via connections with the CNS. The ans consists of the sympathetic and parasympathetic nervous systems.Autonomic Nervous System: Anatomy and receives both sympathetic (inhibitory) and parasympathetic (stimulatory) input.
Connected to the posterior abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen by the dorsal mesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomy
Blood supply located within mesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomy
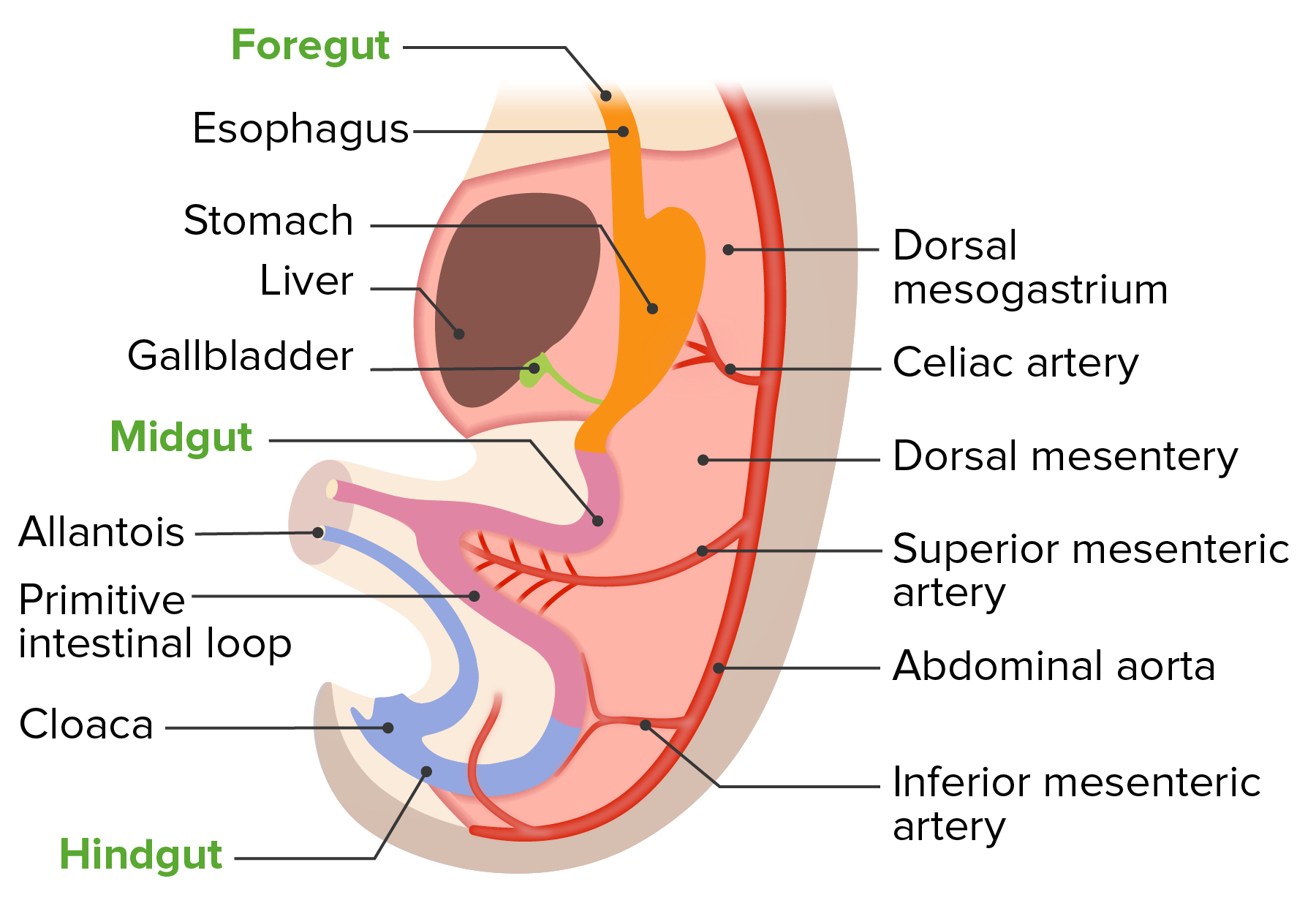
Development of the gut tube
Image by Lecturio.
Gross Anatomy
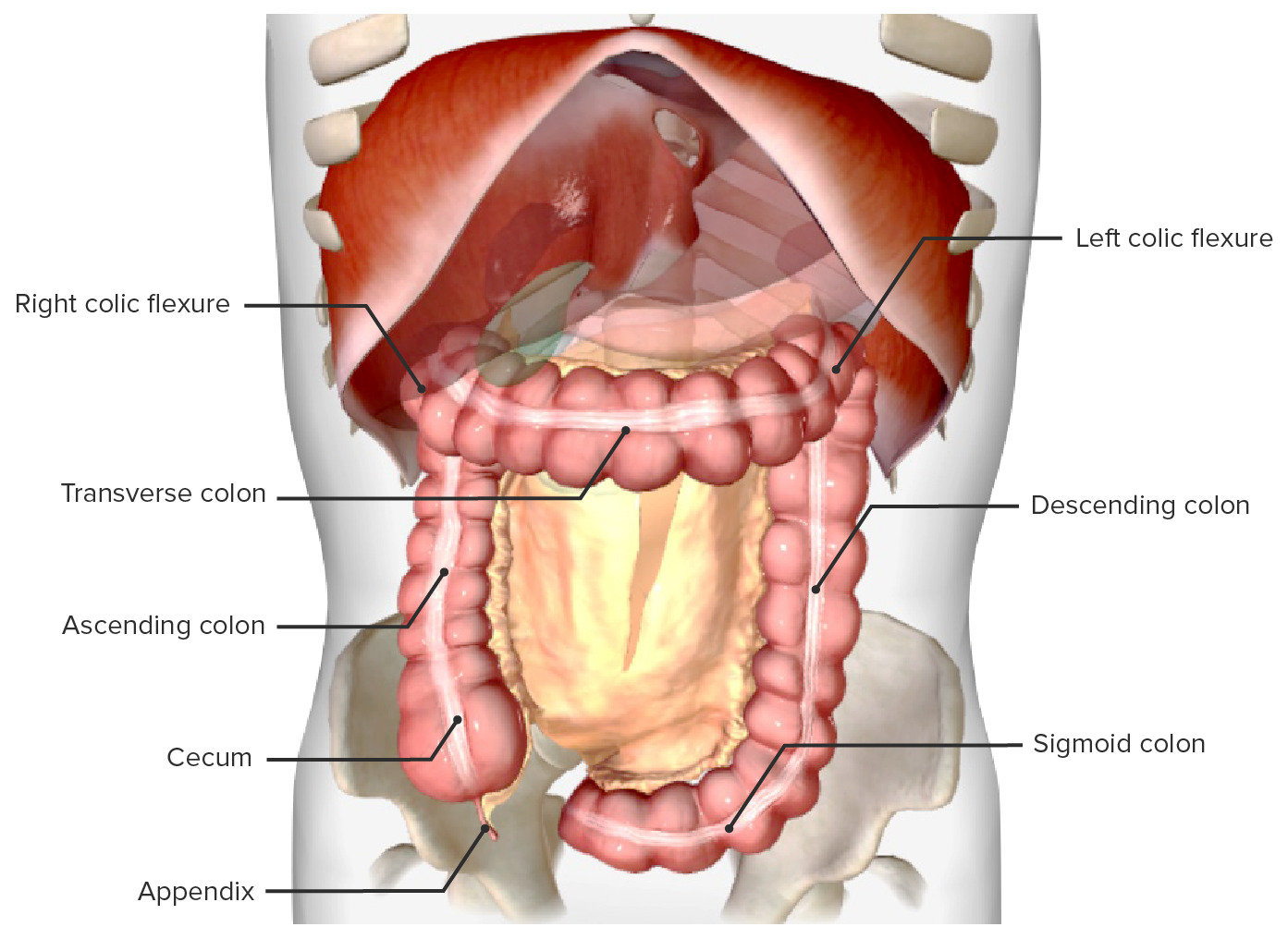
Parts of the large intestine
Cecum
Vermiform appendix
Ascending colon
Transverse colon
Descending colon
SigmoidSigmoidA segment of the colon between the rectum and the descending colon.Volvulus colon
RectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy
Intestinal mesenteries are folds of peritoneumPeritoneumThe peritoneum is a serous membrane lining the abdominopelvic cavity. This lining is formed by connective tissue and originates from the mesoderm. The membrane lines both the abdominal walls (as parietal peritoneum) and all of the visceral organs (as visceral peritoneum).Peritoneum: Anatomy that connect these organs to the posterior abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen.
Some parts of the large intestine have a mesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomy → intraperitonealIntraperitonealPeritoneum: Anatomy
Some parts do not have a mesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomy and are located beneath parietalParietalOne of a pair of irregularly shaped quadrilateral bones situated between the frontal bone and occipital bone, which together form the sides of the cranium.Skull: AnatomyperitoneumPeritoneumThe peritoneum is a serous membrane lining the abdominopelvic cavity. This lining is formed by connective tissue and originates from the mesoderm. The membrane lines both the abdominal walls (as parietal peritoneum) and all of the visceral organs (as visceral peritoneum).Peritoneum: Anatomy → retroperitonealRetroperitonealPeritoneum: Anatomy
Secondarily retroperitonealRetroperitonealPeritoneum: Anatomy: organs that had a mesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomyin utero and that regressed early in development, leaving the organ retroperitonealRetroperitonealPeritoneum: Anatomy in its mature position
General characteristics of the colon
Forms an inverted U shape in the abdomen
About 1.5–2 m long
At the inferior margins of stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy and liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy
Surrounds the small intestineSmall intestineThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum. Small Intestine: Anatomy
Begins at the ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy
Receives chymeChymeSmall Intestine: Anatomy from the ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy through the ileocecal valves
Intestinal pouch between the terminal ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy (at the ileocecal junction) and the ascending colon
Located in the iliac fossa of the RLQ of the abdomen
Covered on all sides by peritoneumPeritoneumThe peritoneum is a serous membrane lining the abdominopelvic cavity. This lining is formed by connective tissue and originates from the mesoderm. The membrane lines both the abdominal walls (as parietal peritoneum) and all of the visceral organs (as visceral peritoneum).Peritoneum: Anatomy (= intraperitonealIntraperitonealPeritoneum: Anatomy), though has no mesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomy (↓ mobility)
Contains the opening into the appendix (appendiceal orifice)
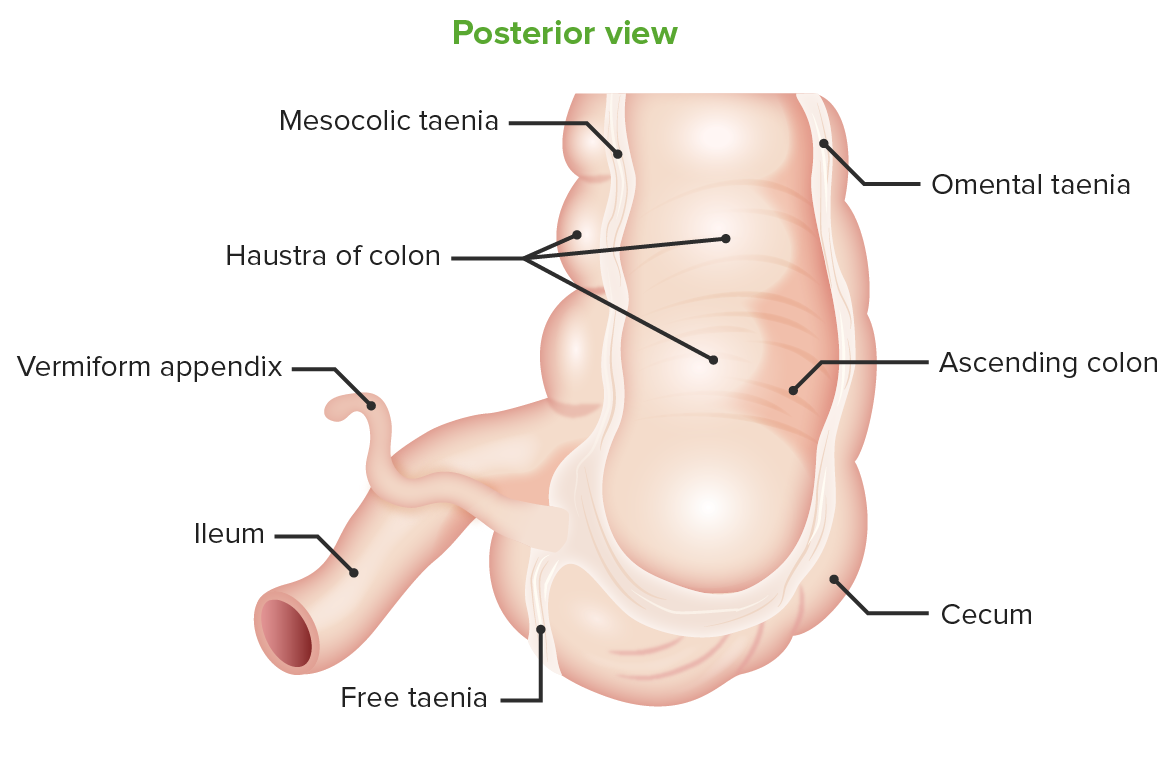
Posterior view of the cecum: Location of the vermiform appendix at the taenia confluence
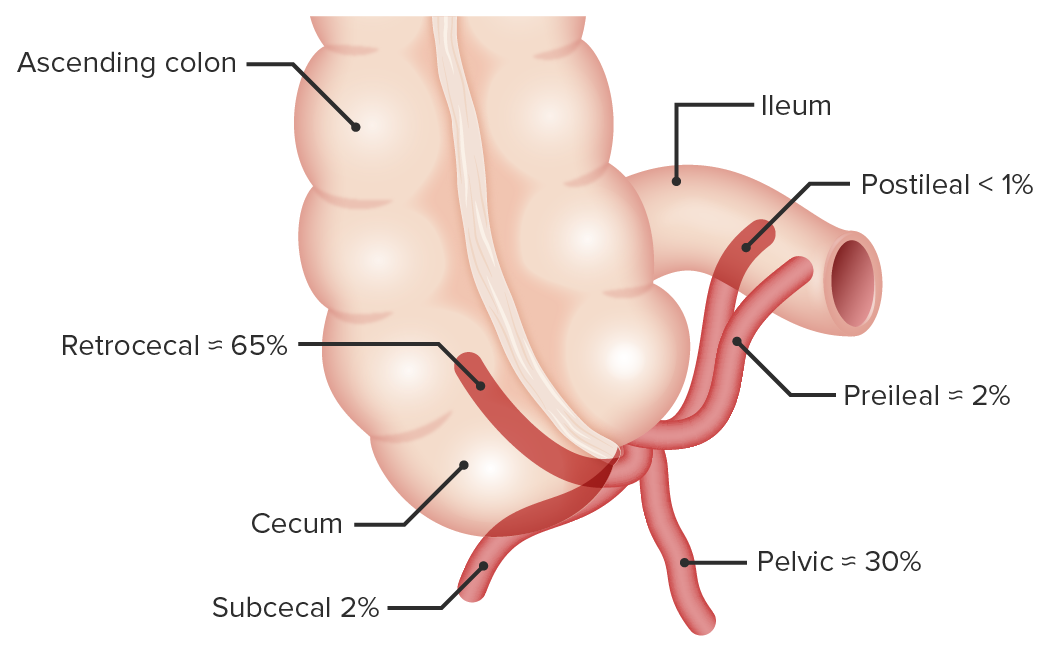
Base arises from the posteromedial aspect of the cecum, inferior to the ileocecal junction.
Location of tail may be:
Retrocecal (65%)
Pelvic (30%)
Subcecal (2%)
Preileal (2%)
Postileal (1%)
Mesoappendix:
Short triangular mesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomy that contains the appendicular vessels
Passes superiorly from the cecum to the right lobe of the liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy
Right colic flexure (also known as the hepatic flexure): end of the ascending colon where it makes a 90-degree turn toward the midline and becomes the transverse colon
Secondarily retroperitonealRetroperitonealPeritoneum: Anatomyorgan → no mesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomy → less mobility
Transverse colon
The 3rd, longest, and most mobile part of the large intestine
Runs transversely across the mid-upper abdomen
Begins at the liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy/right colic flexure (hepatic flexure)
Ends at the spleenSpleenThe spleen is the largest lymphoid organ in the body, located in the LUQ of the abdomen, superior to the left kidney and posterior to the stomach at the level of the 9th-11th ribs just below the diaphragm. The spleen is highly vascular and acts as an important blood filter, cleansing the blood of pathogens and damaged erythrocytes. Spleen: Anatomy/left colic flexure (also known as the splenic flexureSplenic flexureSmall Intestine: Anatomy), where it makes a 90-degree turn inferiorly and becomes the descending colon
Divides the greater sac of the peritoneal cavityPeritoneal CavityThe space enclosed by the peritoneum. It is divided into two portions, the greater sac and the lesser sac or omental bursa, which lies behind the stomach. The two sacs are connected by the foramen of winslow, or epiploic foramen.Peritoneum: Anatomy into supracolic and infracolic compartments
Transverse mesocolon:
MesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomy for the transverse colon
Runs between the left colic (splenic) flexure and the left iliac fossa, where it is continuous with the sigmoidSigmoidA segment of the colon between the rectum and the descending colon.Volvulus colon
Secondarily retroperitonealRetroperitonealPeritoneum: Anatomy organ → no mesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomy → less mobility
SigmoidSigmoidA segment of the colon between the rectum and the descending colon.Volvulus colon
S-shaped loop of variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables lengths
Runs between the descending colon and the rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy
SigmoidSigmoidA segment of the colon between the rectum and the descending colon.Volvulus mesocolon:
MesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomy of the sigmoidSigmoidA segment of the colon between the rectum and the descending colon.Volvulus colon
Several anatomic features distinguish the large intestine from the small intestineSmall intestineThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum. Small Intestine: Anatomy and rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy, including:
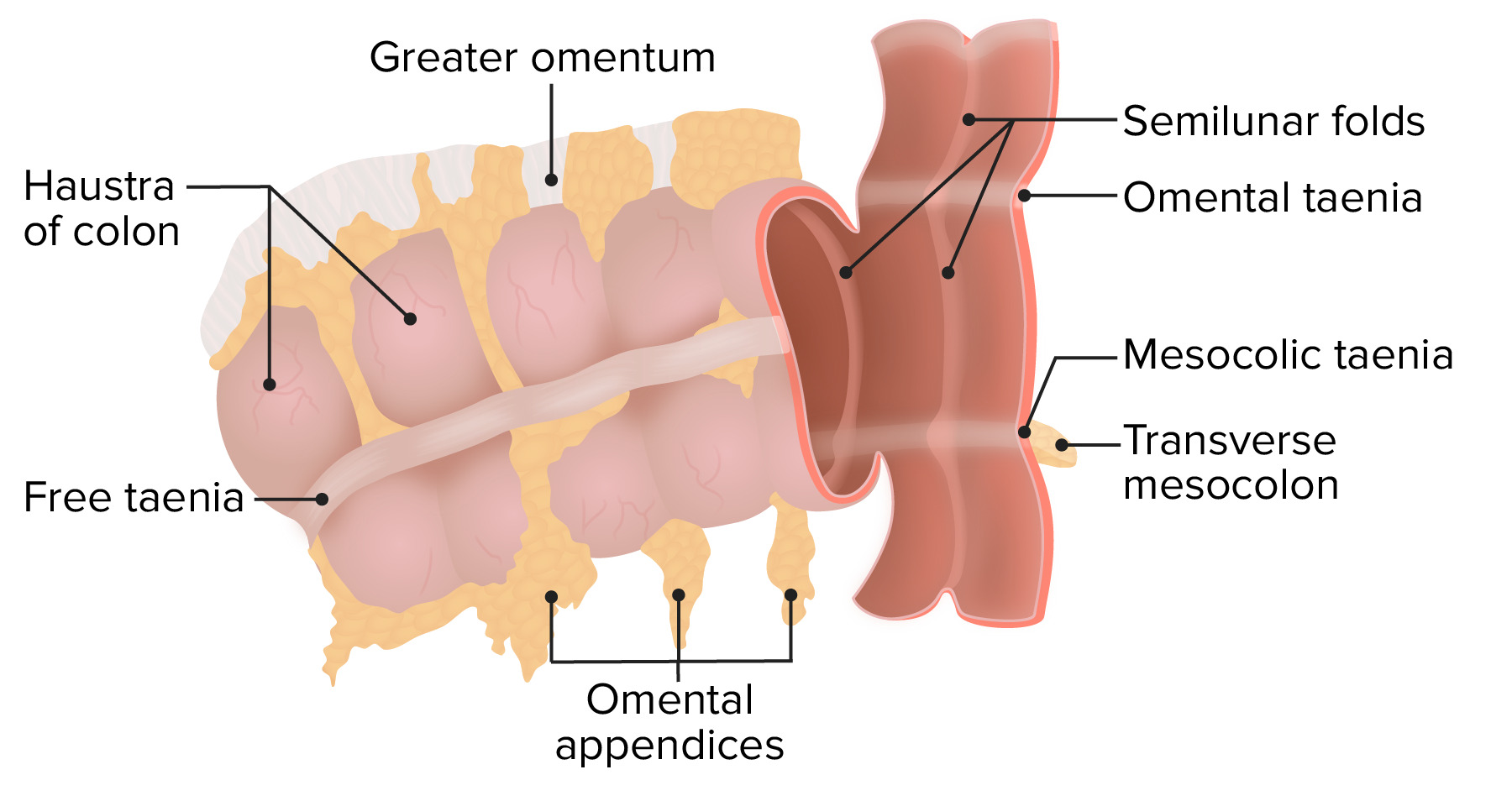
TaeniaTaeniaTaenia belong to the Cestoda class of helminths. Humans are infected with these tapeworms by eating undercooked beef (T. saginata) or pork (T. solium and T. asiatica). Taeniasis is often asymptomatic, but the ingestion of larvae can cause abdominal discomfort, nausea, and constipation or diarrhea.Taenia/Taeniasis coli:
3 discrete bands of longitudinal muscle in the colonic wall (rather than a continuous longitudinal layer in the muscularis as seen in the small intestineSmall intestineThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum. Small Intestine: Anatomy):
Omental taeniaTaeniaTaenia belong to the Cestoda class of helminths. Humans are infected with these tapeworms by eating undercooked beef (T. saginata) or pork (T. solium and T. asiatica). Taeniasis is often asymptomatic, but the ingestion of larvae can cause abdominal discomfort, nausea, and constipation or diarrhea.Taenia/Taeniasis: attaches to the greater omentumOmentumPeritoneum: Anatomy
Mesocolic taeniaTaeniaTaenia belong to the Cestoda class of helminths. Humans are infected with these tapeworms by eating undercooked beef (T. saginata) or pork (T. solium and T. asiatica). Taeniasis is often asymptomatic, but the ingestion of larvae can cause abdominal discomfort, nausea, and constipation or diarrhea.Taenia/Taeniasis: attaches to the transverse mesocolon (which anchors the transverse colon to the posterior abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen)
Free taeniaTaeniaTaenia belong to the Cestoda class of helminths. Humans are infected with these tapeworms by eating undercooked beef (T. saginata) or pork (T. solium and T. asiatica). Taeniasis is often asymptomatic, but the ingestion of larvae can cause abdominal discomfort, nausea, and constipation or diarrhea.Taenia/Taeniasis coli: not attached to other structures
Contract to form the haustra
Haustra:
Sacculations in the colon created by contraction of the longitudinal taeniaTaeniaTaenia belong to the Cestoda class of helminths. Humans are infected with these tapeworms by eating undercooked beef (T. saginata) or pork (T. solium and T. asiatica). Taeniasis is often asymptomatic, but the ingestion of larvae can cause abdominal discomfort, nausea, and constipation or diarrhea.Taenia/Taeniasis coli
Internally, these sacculations are separated by semilunar folds (protrusions of mucosa into the lumen)
Omental appendices (also called epiploic appendages): small, fatty, omentum-like projections
Diagram depicting taenia coli, haustra, and the omental appendices: Note how the transverse mesocolon attaches to the mesocolic taenia.
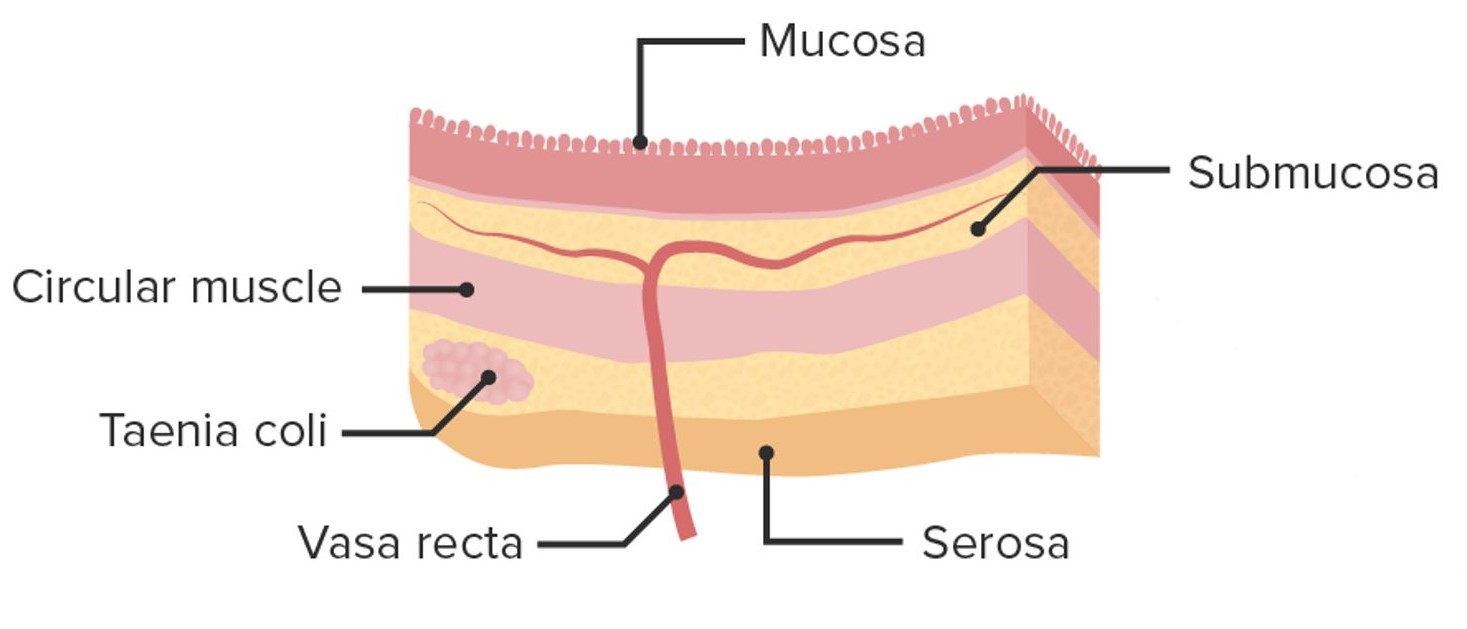
The walls of the large intestine arethinner than those of the small intestineSmall intestineThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum. Small Intestine: Anatomy.
The general layers are the same: mucosa → submucosa → muscularis propria → serosa
Layers of the colon wall
Image by Lecturio.
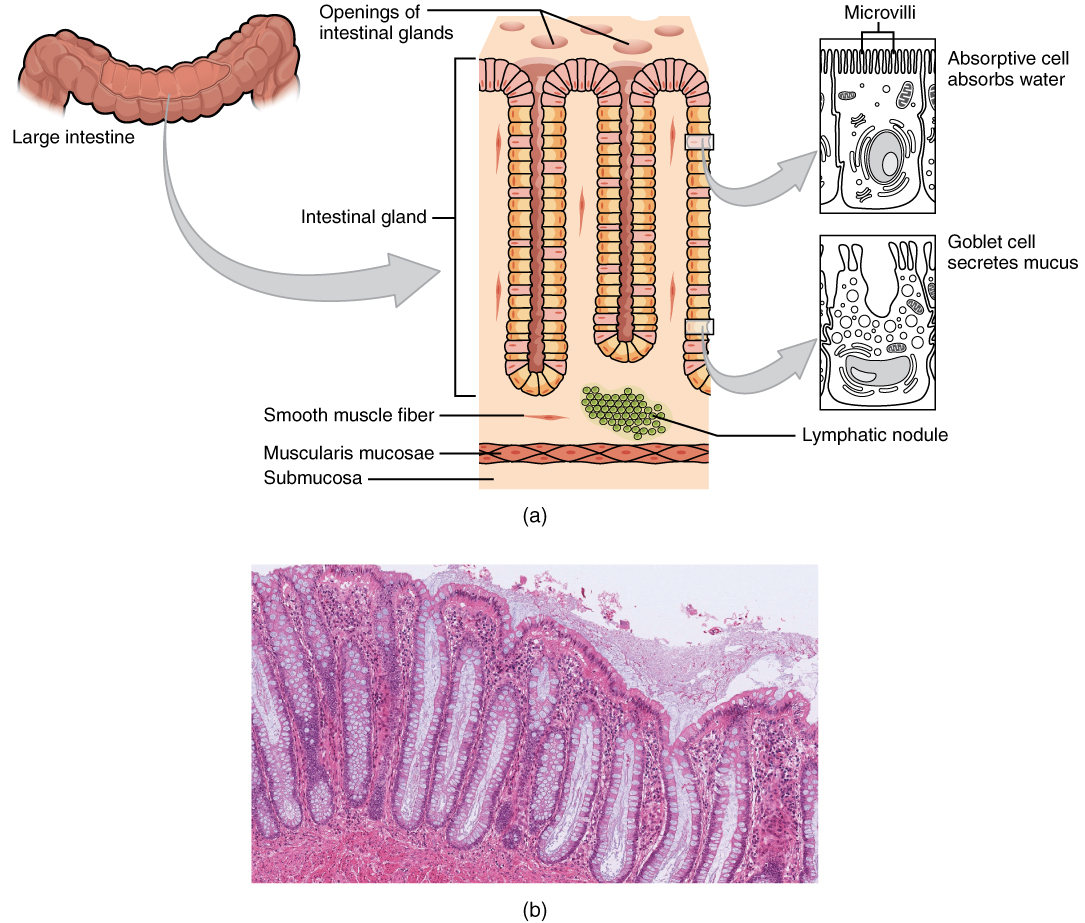
Mucosa
3 sublayers:
Columnar epitheliumEpitheliumThe epithelium is a complex of specialized cellular organizations arranged into sheets and lining cavities and covering the surfaces of the body. The cells exhibit polarity, having an apical and a basal pole. Structures important for the epithelial integrity and function involve the basement membrane, the semipermeable sheet on which the cells rest, and interdigitations, as well as cellular junctions. Surface Epithelium: Histology
Microvilli (also known as the brush borderBrush borderTubular System): present, but less abundant than in the small intestineSmall intestineThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum. Small Intestine: Anatomy
Intestinal glands (also called intestinal crypts):
Pores in the wall, which open into tube-like glands.
Contain a large number of goblet cellsGoblet cellsA glandular epithelial cell or a unicellular gland. Goblet cells secrete mucus. They are scattered in the epithelial linings of many organs, especially the small intestine and the respiratory tract.Glandular Epithelium: Histology:
Mucin-producing epithelial cells
More prominent in large intestine than in small intestineSmall intestineThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum. Small Intestine: Anatomy
Produce copious amounts of mucus for lubrication of feces
Meissner nerve plexus (ganglia of the ANSANSThe ans is a component of the peripheral nervous system that uses both afferent (sensory) and efferent (effector) neurons, which control the functioning of the internal organs and involuntary processes via connections with the CNS. The ans consists of the sympathetic and parasympathetic nervous systems.Autonomic Nervous System: Anatomy): controls the muscularis mucosa (independent of the muscularis propria)
Muscularis propria
The primary muscular layer of the colon wall.
Inner circular layer
Outer longitudinal muscles:
Not a continuous layer
Present in only the 3 bands of tissue, known as taeniaTaeniaTaenia belong to the Cestoda class of helminths. Humans are infected with these tapeworms by eating undercooked beef (T. saginata) or pork (T. solium and T. asiatica). Taeniasis is often asymptomatic, but the ingestion of larvae can cause abdominal discomfort, nausea, and constipation or diarrhea.Taenia/Taeniasis coli:
Omental taeniaTaeniaTaenia belong to the Cestoda class of helminths. Humans are infected with these tapeworms by eating undercooked beef (T. saginata) or pork (T. solium and T. asiatica). Taeniasis is often asymptomatic, but the ingestion of larvae can cause abdominal discomfort, nausea, and constipation or diarrhea.Taenia/Taeniasis coli
Mesocolic taeniaTaeniaTaenia belong to the Cestoda class of helminths. Humans are infected with these tapeworms by eating undercooked beef (T. saginata) or pork (T. solium and T. asiatica). Taeniasis is often asymptomatic, but the ingestion of larvae can cause abdominal discomfort, nausea, and constipation or diarrhea.Taenia/Taeniasis coli
Free taeniaTaeniaTaenia belong to the Cestoda class of helminths. Humans are infected with these tapeworms by eating undercooked beef (T. saginata) or pork (T. solium and T. asiatica). Taeniasis is often asymptomatic, but the ingestion of larvae can cause abdominal discomfort, nausea, and constipation or diarrhea.Taenia/Taeniasis coli
Contains the myenteric (Auerbach) plexus:
Ganglia of the ANSANSThe ans is a component of the peripheral nervous system that uses both afferent (sensory) and efferent (effector) neurons, which control the functioning of the internal organs and involuntary processes via connections with the CNS. The ans consists of the sympathetic and parasympathetic nervous systems.Autonomic Nervous System: Anatomy, which controls the muscular layer.
Located between 2 layers of smooth muscle
Serosa
Made up of connective tissueConnective tissueConnective tissues originate from embryonic mesenchyme and are present throughout the body except inside the brain and spinal cord. The main function of connective tissues is to provide structural support to organs. Connective tissues consist of cells and an extracellular matrix.Connective Tissue: Histology
Connected to mesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomy or peritoneumPeritoneumThe peritoneum is a serous membrane lining the abdominopelvic cavity. This lining is formed by connective tissue and originates from the mesoderm. The membrane lines both the abdominal walls (as parietal peritoneum) and all of the visceral organs (as visceral peritoneum).Peritoneum: Anatomy
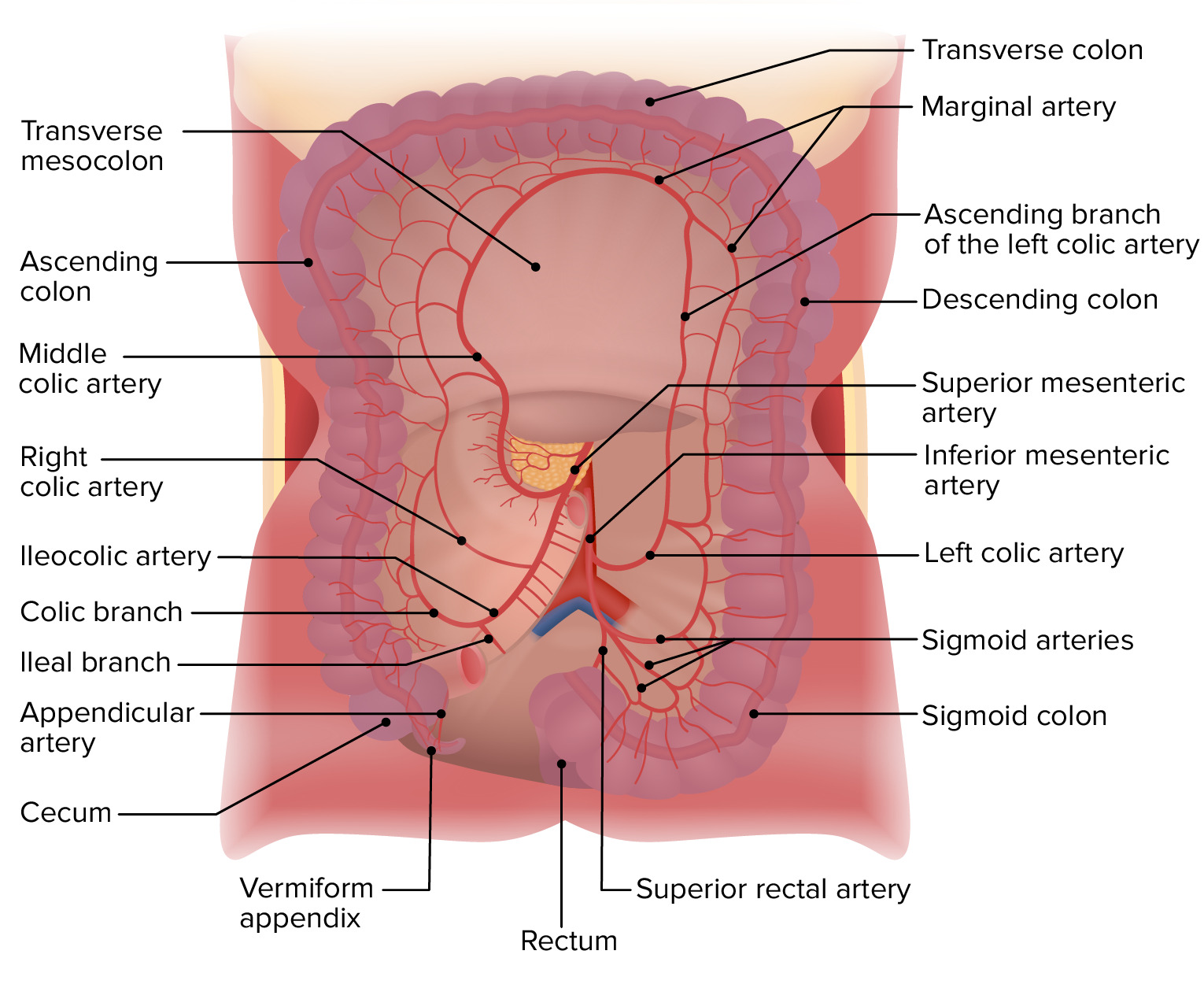
The arterial supply is via the superior mesenteric arterySuperior mesenteric arteryA large vessel supplying the whole length of the small intestine except the superior part of the duodenum. It also supplies the cecum and the ascending part of the colon and about half the transverse part of the colon. It arises from the anterior surface of the aorta below the celiac artery at the level of the first lumbar vertebra.Small Intestine: Anatomy (SMA) and the inferior mesenteric arteryInferior mesenteric arteryThe artery supplying nearly all the left half of the transverse colon, the whole of the descending colon, the sigmoid colon, and the greater part of the rectum. It is smaller than the superior mesenteric artery and arises from the aorta above its bifurcation into the common iliac arteries.Small Intestine: Anatomy (IMA).
SMA branches (starting in the RLQ and moving clockwise):
Ileocolic artery:
Colic branch → cecum
Appendicular artery (off the colic branch) → appendix
Ileal branch → terminal ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy
Right colic artery → ascending colon
Middle colic artery:
Supplies the ascending and transverse colons
Continuous with the marginal artery
Marginal artery (of Drummond):
Supplies the transverse colon
Forms an important anastomosis between the middle colic artery (off the SMA) and the left colic artery (off the IMA)
Jejunal and ileal arteriesArteriesArteries are tubular collections of cells that transport oxygenated blood and nutrients from the heart to the tissues of the body. The blood passes through the arteries in order of decreasing luminal diameter, starting in the largest artery (the aorta) and ending in the small arterioles. Arteries are classified into 3 types: large elastic arteries, medium muscular arteries, and small arteries and arterioles. Arteries: Histology → jejunumJejunumThe middle portion of the small intestine, between duodenum and ileum. It represents about 2/5 of the remaining portion of the small intestine below duodenum.Small Intestine: Anatomy and ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy
IMA branches (starting in the LUQ and moving clockwise):
Left colic artery:
Supplies the descending colon
Anastomoses with the marginal artery, connecting circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment from the SMA and IMA
SigmoidSigmoidA segment of the colon between the rectum and the descending colon.VolvulusarteriesArteriesArteries are tubular collections of cells that transport oxygenated blood and nutrients from the heart to the tissues of the body. The blood passes through the arteries in order of decreasing luminal diameter, starting in the largest artery (the aorta) and ending in the small arterioles. Arteries are classified into 3 types: large elastic arteries, medium muscular arteries, and small arteries and arterioles. Arteries: Histology → sigmoidSigmoidA segment of the colon between the rectum and the descending colon.Volvulus colon
Superior rectal artery → upper rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy
The cecum, appendix, and colon drain via named veinsVeinsVeins are tubular collections of cells, which transport deoxygenated blood and waste from the capillary beds back to the heart. Veins are classified into 3 types: small veins/venules, medium veins, and large veins. Each type contains 3 primary layers: tunica intima, tunica media, and tunica adventitia. Veins: Histology that run parallel to their arteriesArteriesArteries are tubular collections of cells that transport oxygenated blood and nutrients from the heart to the tissues of the body. The blood passes through the arteries in order of decreasing luminal diameter, starting in the largest artery (the aorta) and ending in the small arterioles. Arteries are classified into 3 types: large elastic arteries, medium muscular arteries, and small arteries and arterioles. Arteries: Histology, which ultimately drain into the superior mesenteric vein (SMV) and the inferior mesenteric vein (IMVIMVInvasive mechanical ventilation (IMV) is an advanced airway modality used for individuals with immediate or impending respiratory failure and/or in preparation for surgery. The IMV technique involves positive pressure ventilation delivered to the lungs through an endotracheal tube via a ventilator.Invasive Mechanical Ventilation).
SMV:
Receives drainage from:
Right ½ of the large intestines
Via the ileocolic and right and middle colic veinsVeinsVeins are tubular collections of cells, which transport deoxygenated blood and waste from the capillary beds back to the heart. Veins are classified into 3 types: small veins/venules, medium veins, and large veins. Each type contains 3 primary layers: tunica intima, tunica media, and tunica adventitia. Veins: Histology
IMVIMVInvasive mechanical ventilation (IMV) is an advanced airway modality used for individuals with immediate or impending respiratory failure and/or in preparation for surgery. The IMV technique involves positive pressure ventilation delivered to the lungs through an endotracheal tube via a ventilator.Invasive Mechanical Ventilation:
Receives drainage from:
Left ½ of the large intestines
Via the superior rectal, sigmoidSigmoidA segment of the colon between the rectum and the descending colon.Volvulus, and left colic veinsVeinsVeins are tubular collections of cells, which transport deoxygenated blood and waste from the capillary beds back to the heart. Veins are classified into 3 types: small veins/venules, medium veins, and large veins. Each type contains 3 primary layers: tunica intima, tunica media, and tunica adventitia. Veins: Histology
Right, middle, and left colic lymph nodesLymph NodesThey are oval or bean shaped bodies (1 – 30 mm in diameter) located along the lymphatic system.Lymphatic Drainage System: Anatomy
Innervation
The colon is innervated by the ANSANSThe ans is a component of the peripheral nervous system that uses both afferent (sensory) and efferent (effector) neurons, which control the functioning of the internal organs and involuntary processes via connections with the CNS. The ans consists of the sympathetic and parasympathetic nervous systems.Autonomic Nervous System: Anatomy, which has parasympathetic and sympathetic divisions.
Parasympathetic innervation:
Stimulatory
Via branches of the:
Vagus nerveVagus nerveThe 10th cranial nerve. The vagus is a mixed nerve which contains somatic afferents (from skin in back of the ear and the external auditory meatus), visceral afferents (from the pharynx, larynx, thorax, and abdomen), parasympathetic efferents (to the thorax and abdomen), and efferents to striated muscle (of the larynx and pharynx).Pharynx: Anatomy
Water absorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption
Vitamin production by bacterial flora (and absorptionAbsorptionAbsorption involves the uptake of nutrient molecules and their transfer from the lumen of the GI tract across the enterocytes and into the interstitial space, where they can be taken up in the venous or lymphatic circulation.Digestion and Absorption):
Vitamin KVitamin KA lipid cofactor that is required for normal blood clotting. Several forms of vitamin K have been identified: vitamin K 1 (phytomenadione) derived from plants, vitamin K 2 (menaquinone) from bacteria, and synthetic naphthoquinone provitamins, vitamin K 3 (menadione). Vitamin k 3 provitamins, after being alkylated in vivo, exhibit the antifibrinolytic activity of vitamin k. Green leafy vegetables, liver, cheese, butter, and egg yolk are good sources of vitamin k.Fat-soluble Vitamins and their Deficiencies
Several B vitamins
Compaction of feces
Storage of feces
Moving waste materials toward the rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy for expulsion
Clinical Relevance
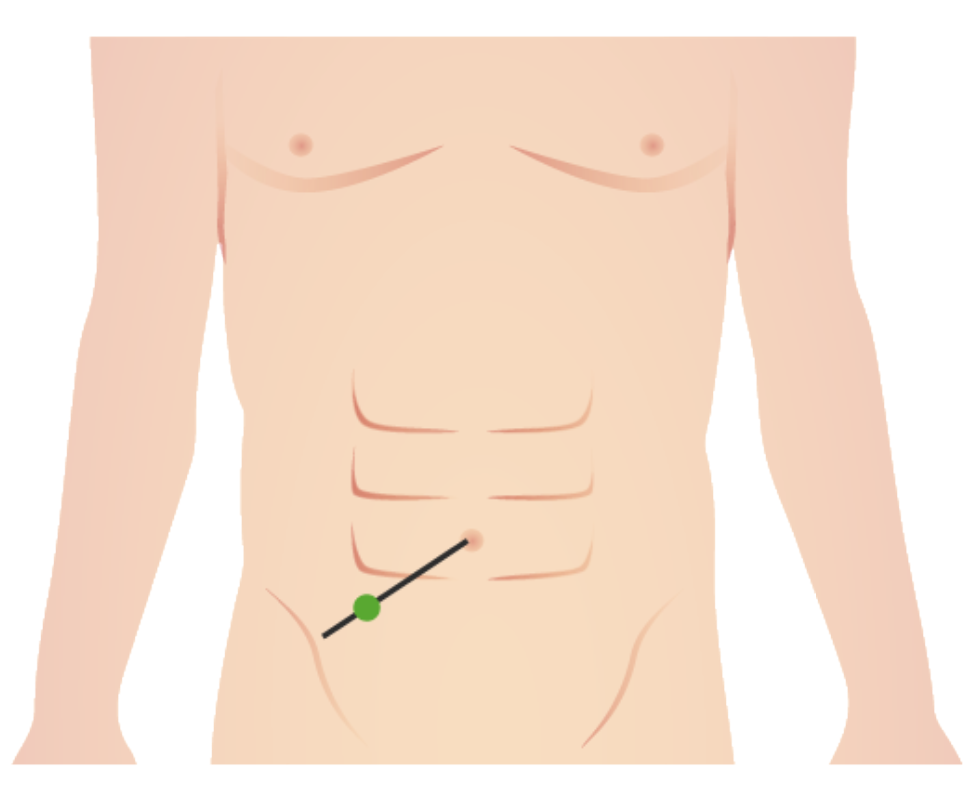
AppendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis: acute inflammationAcute InflammationInflammation of the appendix caused by obstruction of the lumen, typically due to calcified feces, tumors, or foreign bodies. AppendicitisAppendicitisAppendicitis is the acute inflammation of the vermiform appendix and the most common abdominal surgical emergency globally. The condition has a lifetime risk of 8%. Characteristic features include periumbilical abdominal pain that migrates to the right lower quadrant, fever, anorexia, nausea, and vomiting.Appendicitis is the most common abdominal surgical emergencySurgical EmergencyAcute Abdomen worldwide; it classically presents with periumbilical abdominal painAbdominal PainAcute Abdomen that migrates to the RLQ, feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, anorexiaAnorexiaThe lack or loss of appetite accompanied by an aversion to food and the inability to eat. It is the defining characteristic of the disorder anorexia nervosa.Anorexia Nervosa, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia. Management is usually surgical.
DiverticulosisDiverticulosisA pathological condition characterized by the presence of a number of colonic diverticula in the colon. Its pathogenesis is multifactorial, including colon aging, motor dysfunction, increases in intraluminal pressure, and lack of dietary fibers.Diverticular Disease: An intestinal diverticulumDiverticulumA pouch or sac opening from the colon.Diverticular Disease is a sac-like bulge of the intestinal wall protruding outward. Diverticula arise because of the increased intestinal pressures associated with a low-fiber diet and when the transport of intestinal content is slower. The condition is typically asymptomatic.
DiverticulitisDiverticulitisInflammation of a diverticulum or diverticula.Diverticular Disease: inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of diverticula that occurs when the diverticula become occluded. DiverticulitisDiverticulitisInflammation of a diverticulum or diverticula.Diverticular Disease often presents with lower abdominal painAbdominal PainAcute Abdomen and changes in bowel habits and may become complicated by abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease, perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis, fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula, and bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis.
Ischemic colitisIschemic colitisInflammation of the colon due to colonic ischemia resulting from alterations in systemic circulation or local vasculature.Large Bowel Obstruction: ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage of the colon due to hypoperfusion that may result from vessel occlusion (e.g., arterial thromboembolic events), hypovolemic shockHypovolemic ShockTypes of Shock, sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock, or traumatic vessel lacerationLacerationTorn, ragged, mangled wounds.Blunt Chest Trauma. The SMA is most commonly affected. Classically, presentation is with sudden onset of painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways that is out of proportion to physical findings. The primary goal of management is to restore blood flowBlood flowBlood flow refers to the movement of a certain volume of blood through the vasculature over a given unit of time (e.g., mL per minute).Vascular Resistance, Flow, and Mean Arterial Pressure.
Colon polypsColon polypsColon polyps are growths of mucosal tissue in the colon, the most common site of polyps in the GI tract. Polyps can be classified as neoplastic or nonneoplastic and may be associated with genetic syndromes. Hyperplastic polyps are nonneoplastic and are the most common type overall, whereas adenomas are the most common type of neoplastic polyp and have the potential to progress to cancer. Colon Polyps: A polyp is an overgrowth of mucosal tissue in the large intestine. A polyp may be sessile (wide and flat), branched, or pedunculated. Polyps are usually < 1 cm and do not cause any symptoms, though they may cause constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation, diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea, or blood in the stool. Polyps can be classified as neoplastic or nonneoplastic. HyperplasticHyperplasticColon Polyps polyps are nonneoplastic, while adenomas are the most common type of neoplastic polyp and have the potential to progress to cancer. Polyps may be associated with genetic syndromes.
Colorectal cancerColorectal cancerColorectal cancer (CRC) is the 2nd leading cause of cancer-related deaths in the United States. Colorectal cancer is a heterogeneous disease that arises from genetic and epigenetic abnormalities, with influence from environmental factors. Colorectal Cancer (CRC): malignant tumorTumorInflammation of the colon and/or rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy. Almost all cases of CRC are adenocarcinoma, and the majority of lesions come from the malignant transformationTransformationChange brought about to an organism’s genetic composition by unidirectional transfer (transfection; transduction, genetic; conjugation, genetic, etc.) and incorporation of foreign DNA into prokaryotic or eukaryotic cells by recombination of part or all of that DNA into the cell’s genome.Bacteriology of an adenomatous polypAdenomatous polypBenign neoplasms derived from glandular epithelium.Colon Polyps. Colorectal cancerColorectal cancerColorectal cancer (CRC) is the 2nd leading cause of cancer-related deaths in the United States. Colorectal cancer is a heterogeneous disease that arises from genetic and epigenetic abnormalities, with influence from environmental factors. Colorectal Cancer is usually asymptomatic, with symptoms such as occult bleeding typically developing late. The prognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas depends on the stage of cancer at discovery.
MalrotationMalrotationPediatric Gastrointestinal Abnormalities of the gut: congenital anomaly resulting from abnormal rotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays of the primitive gut tube during development. There are a number of variants of this condition, but typically the entire large intestine is located in the left ½ of the abdomen and the small intestines are located in the right ½. MalrotationMalrotationPediatric Gastrointestinal Abnormalities of the gut may be asymptomatic, or it may result in significant complications, such as midgutMidgutDevelopment of the Abdominal OrgansvolvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus.
Large bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis: interruption in the normal flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure of intestinal contents through the colon and rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy. This obstruction may be mechanical (due to actual physical occlusion of the lumen) or functional (due to a loss of normal peristalsisPeristalsisA movement, caused by sequential muscle contraction, that pushes the contents of the intestines or other tubular organs in one direction.Gastrointestinal Motility, also known as pseudo-obstruction). MalignancyMalignancyHemothorax and volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus are the most common causes of mechanical large bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis. The typical symptoms include intermittent lower abdominal painAbdominal PainAcute Abdomen, abdominal distentionAbdominal distentionMegacolon, and obstipationObstipationLarge Bowel Obstruction.
Irritable bowel syndromeIrritable bowel syndromeIrritable bowel syndrome (IBS) is a functional bowel disease characterized by chronic abdominal pain and altered bowel habits without an identifiable organic cause. The etiology and pathophysiology of this disease are not well understood, and there are many factors that may contribute. Irritable Bowel Syndrome (IBSIBSIrritable bowel syndrome (IBS) is a functional bowel disease characterized by chronic abdominal pain and altered bowel habits without an identifiable organic cause. The etiology and pathophysiology of this disease are not well understood, and there are many factors that may contribute. Irritable Bowel Syndrome): functional bowel disease characterized by chronic abdominal painAbdominal PainAcute Abdomen and altered bowel habits without an identifiable organic cause. Symptoms of IBSIBSIrritable bowel syndrome (IBS) is a functional bowel disease characterized by chronic abdominal pain and altered bowel habits without an identifiable organic cause. The etiology and pathophysiology of this disease are not well understood, and there are many factors that may contribute. Irritable Bowel Syndrome may include digestive problems along with abdominal painAbdominal PainAcute Abdomen, diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea, or constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation. This syndrome is associated with glutenGlutenProlamins in the endosperm of seeds from the triticeae tribe which includes species of wheat; barley; and rye.Celiac Disease sensitivity and psychological factors and is a diagnosis of exclusion.