The abdominal organs are derived primarily from endodermEndodermThe inner of the three germ layers of an embryo.Gastrulation and Neurulation, which forms the primitive gut tube. The gut tube is divided into 3 regions: foregut, midgut, and hindgut. The foregut gives rise to the lining of the GI tract from the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy to the upper duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy, as well as the liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy, gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy, and pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy. The midgut gives rise to the GI tract lining between the midduodenum and midtransverse colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy. The hindgut gives rise to the GI tract lining from the midtransverse colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy through the upper anal canal. The mesodermMesodermThe middle germ layer of an embryo derived from three paired mesenchymal aggregates along the neural tube.Gastrulation and Neurulation gives rise to the muscles of the GI tract wall, connective tissueConnective tissueConnective tissues originate from embryonic mesenchyme and are present throughout the body except inside the brain and spinal cord. The main function of connective tissues is to provide structural support to organs. Connective tissues consist of cells and an extracellular matrix.Connective Tissue: Histology (including the mesenteries and omenta), and the vasculature. The ectodermEctodermThe outer of the three germ layers of an embryo.Gastrulation and Neurulation gives rise to the nerve tissue and the lining of the lower anal canal.
BlastocystBlastocystA post-morula preimplantation mammalian embryo that develops from a 32-cell stage into a fluid-filled hollow ball of over a hundred cells. A blastocyst has two distinctive tissues. The outer layer of trophoblasts gives rise to extra-embryonic tissues. The inner cell mass gives rise to the embryonic disc and eventual embryo proper.Fertilization and First Week and bilaminar discBilaminar discEmbryoblast and Trophoblast Development
The morulaMorulaAn early embryo that is a compact mass of about 16 blastomeres. It resembles a cluster of mulberries with two types of cells, outer cells and inner cells. Morula is the stage before blastula in non-mammalian animals or a blastocyst in mammals.Fertilization and First Week (ball of cells) undergoes a process called blastulation, in which a cavity begins to form. The cells then begin differentiating into outer and inner cell masses.
Outer cell massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast → trophoblastTrophoblastCells lining the outside of the blastocyst. After binding to the endometrium, trophoblasts develop into two distinct layers, an inner layer of mononuclear cytotrophoblasts and an outer layer of continuous multinuclear cytoplasm, the syncytiotrophoblasts, which form the early fetal-maternal interface (placenta).Fertilization and First Week → placentaPlacentaA highly vascularized mammalian fetal-maternal organ and major site of transport of oxygen, nutrients, and fetal waste products. It includes a fetal portion (chorionic villi) derived from trophoblasts and a maternal portion (decidua) derived from the uterine endometrium. The placenta produces an array of steroid, protein and peptide hormones (placental hormones).Placenta, Umbilical Cord, and Amniotic Cavity and membranes
Amniotic sac: a cavity of fluid that develops “above” the epiblastEpiblastEmbryoblast and Trophoblast Development (between epiblastEpiblastEmbryoblast and Trophoblast Development and trophoblastTrophoblastCells lining the outside of the blastocyst. After binding to the endometrium, trophoblasts develop into two distinct layers, an inner layer of mononuclear cytotrophoblasts and an outer layer of continuous multinuclear cytoplasm, the syncytiotrophoblasts, which form the early fetal-maternal interface (placenta).Fertilization and First Week)
Primitive yolk sacYolk SacThe first of four extra-embryonic membranes to form during embryogenesis. In reptiles and birds, it arises from endoderm and mesoderm to incorporate the egg yolk into the digestive tract for nourishing the embryo. In placental mammals, its nutritional function is vestigial; however, it is the source of intestinal mucosa; blood cells; and germ cells. It is sometimes called the vitelline sac, which should not be confused with the vitelline membrane of the egg.Embryoblast and Trophoblast Development:
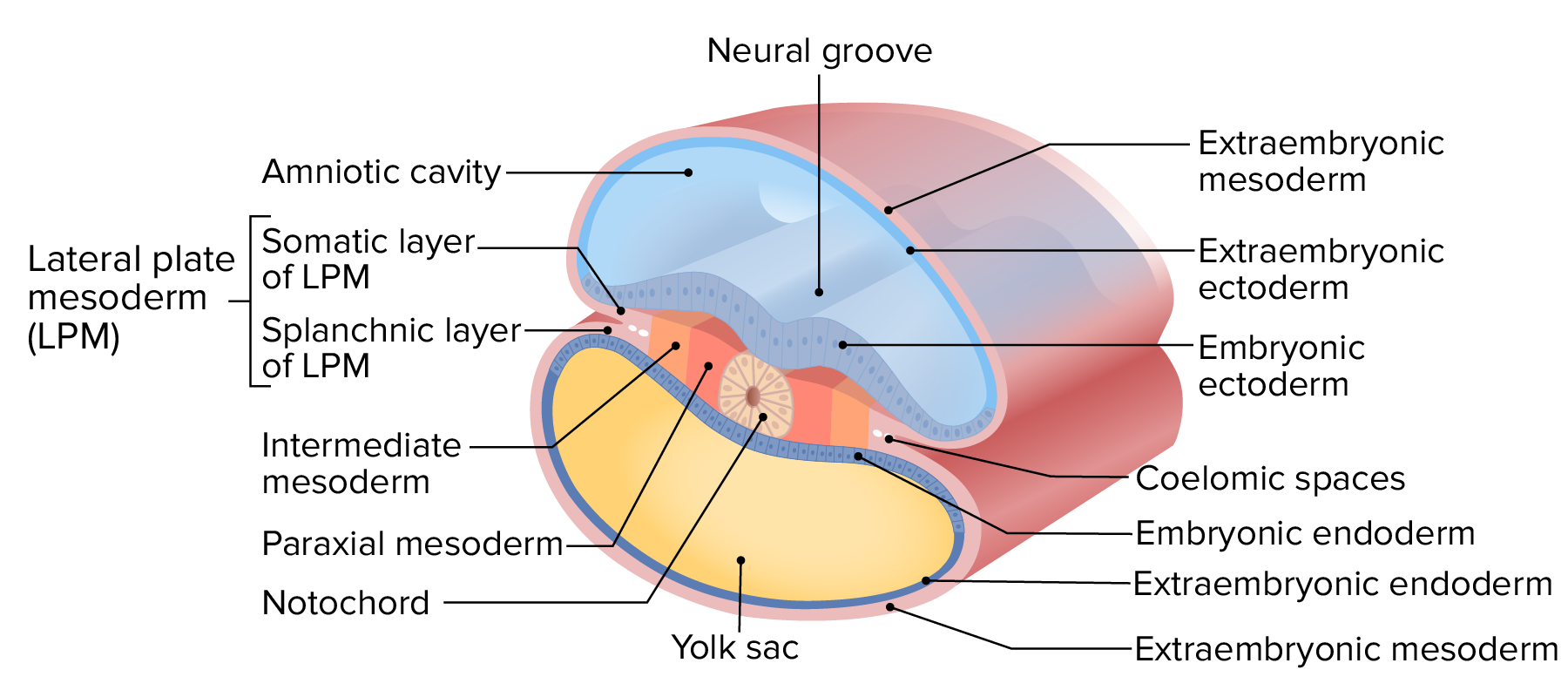
The bilaminar disk undergoes a process called gastrulationGastrulationBoth gastrulation and neurulation are critical events that occur during the 3rd week of embryonic development. Gastrulation is the process by which the bilaminar disc differentiates into a trilaminar disc, made up of the 3 primary germ layers: the ectoderm, mesoderm, and endoderm.Gastrulation and Neurulation to form the trilaminar discTrilaminar discGastrulation and Neurulation. There are 3 layers of the trilaminar discTrilaminar discGastrulation and Neurulation:
EctodermEctodermThe outer of the three germ layers of an embryo.Gastrulation and Neurulation (continuous with the amnionAmnionThe innermost membranous sac that surrounds and protects the developing embryo which is bathed in the amniotic fluid. Amnion cells are secretory epithelial cells and contribute to the amniotic fluid.Placenta, Umbilical Cord, and Amniotic Cavity)
MesodermMesodermThe middle germ layer of an embryo derived from three paired mesenchymal aggregates along the neural tube.Gastrulation and Neurulation:
Paraxial mesodermMesodermThe middle germ layer of an embryo derived from three paired mesenchymal aggregates along the neural tube.Gastrulation and Neurulation
Lateral plate mesodermMesodermThe middle germ layer of an embryo derived from three paired mesenchymal aggregates along the neural tube.Gastrulation and Neurulation (LPM):
Surrounds the yolk sacYolk SacThe first of four extra-embryonic membranes to form during embryogenesis. In reptiles and birds, it arises from endoderm and mesoderm to incorporate the egg yolk into the digestive tract for nourishing the embryo. In placental mammals, its nutritional function is vestigial; however, it is the source of intestinal mucosa; blood cells; and germ cells. It is sometimes called the vitelline sac, which should not be confused with the vitelline membrane of the egg.Embryoblast and Trophoblast Development → continuous with the splanchnic LPM
Extraembryonic endodermEndodermThe inner of the three germ layers of an embryo.Gastrulation and Neurulation → lines the yolk sacYolk SacThe first of four extra-embryonic membranes to form during embryogenesis. In reptiles and birds, it arises from endoderm and mesoderm to incorporate the egg yolk into the digestive tract for nourishing the embryo. In placental mammals, its nutritional function is vestigial; however, it is the source of intestinal mucosa; blood cells; and germ cells. It is sometimes called the vitelline sac, which should not be confused with the vitelline membrane of the egg.Embryoblast and Trophoblast Development
Secondary yolk sacYolk SacThe first of four extra-embryonic membranes to form during embryogenesis. In reptiles and birds, it arises from endoderm and mesoderm to incorporate the egg yolk into the digestive tract for nourishing the embryo. In placental mammals, its nutritional function is vestigial; however, it is the source of intestinal mucosa; blood cells; and germ cells. It is sometimes called the vitelline sac, which should not be confused with the vitelline membrane of the egg.Embryoblast and Trophoblast Development:the cavity between embryonic and extraembryonic endodermEndodermThe inner of the three germ layers of an embryo.Gastrulation and Neurulation
Folding of the trilaminar disk (folds in 2 directions):
Creates a cranial end and a caudal end (embryoEmbryoThe entity of a developing mammal, generally from the cleavage of a zygote to the end of embryonic differentiation of basic structures. For the human embryo, this represents the first two months of intrauterine development preceding the stages of the fetus.Fertilization and First Week becomes “bean-shaped”)
Forces the yolk sacYolk SacThe first of four extra-embryonic membranes to form during embryogenesis. In reptiles and birds, it arises from endoderm and mesoderm to incorporate the egg yolk into the digestive tract for nourishing the embryo. In placental mammals, its nutritional function is vestigial; however, it is the source of intestinal mucosa; blood cells; and germ cells. It is sometimes called the vitelline sac, which should not be confused with the vitelline membrane of the egg.Embryoblast and Trophoblast Development farther from the body.→ The elongating stalk connecting the yolk sacYolk SacThe first of four extra-embryonic membranes to form during embryogenesis. In reptiles and birds, it arises from endoderm and mesoderm to incorporate the egg yolk into the digestive tract for nourishing the embryo. In placental mammals, its nutritional function is vestigial; however, it is the source of intestinal mucosa; blood cells; and germ cells. It is sometimes called the vitelline sac, which should not be confused with the vitelline membrane of the egg.Embryoblast and Trophoblast Development to the gut tube is the vitelline ductVitelline ductThe narrow tube connecting the yolk sac with the midgut of the embryo; persistence of all or part of it in post-fetal life produces abnormalities, of which the commonest is meckel diverticulum.Meckel’s Diverticulum.
Layers of the trilaminar disc.
Image by Lecturio.
Cross-sectional view of the early embryo after it has undergone lateral folding
Image by Lecturio.
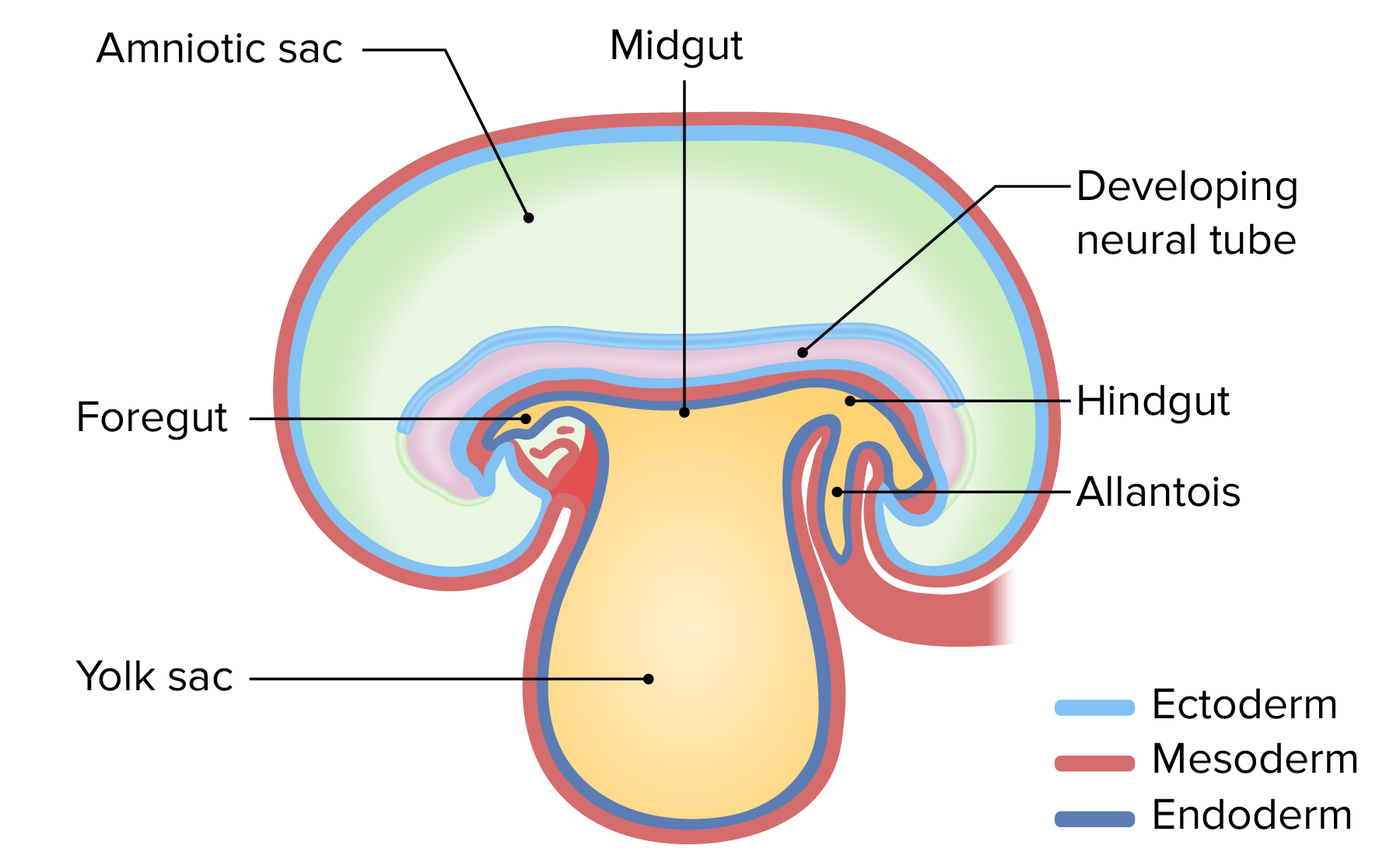
The early embryo with the amniotic sac above the embryo and the yolk sac below the embryo
Image by Lecturio.
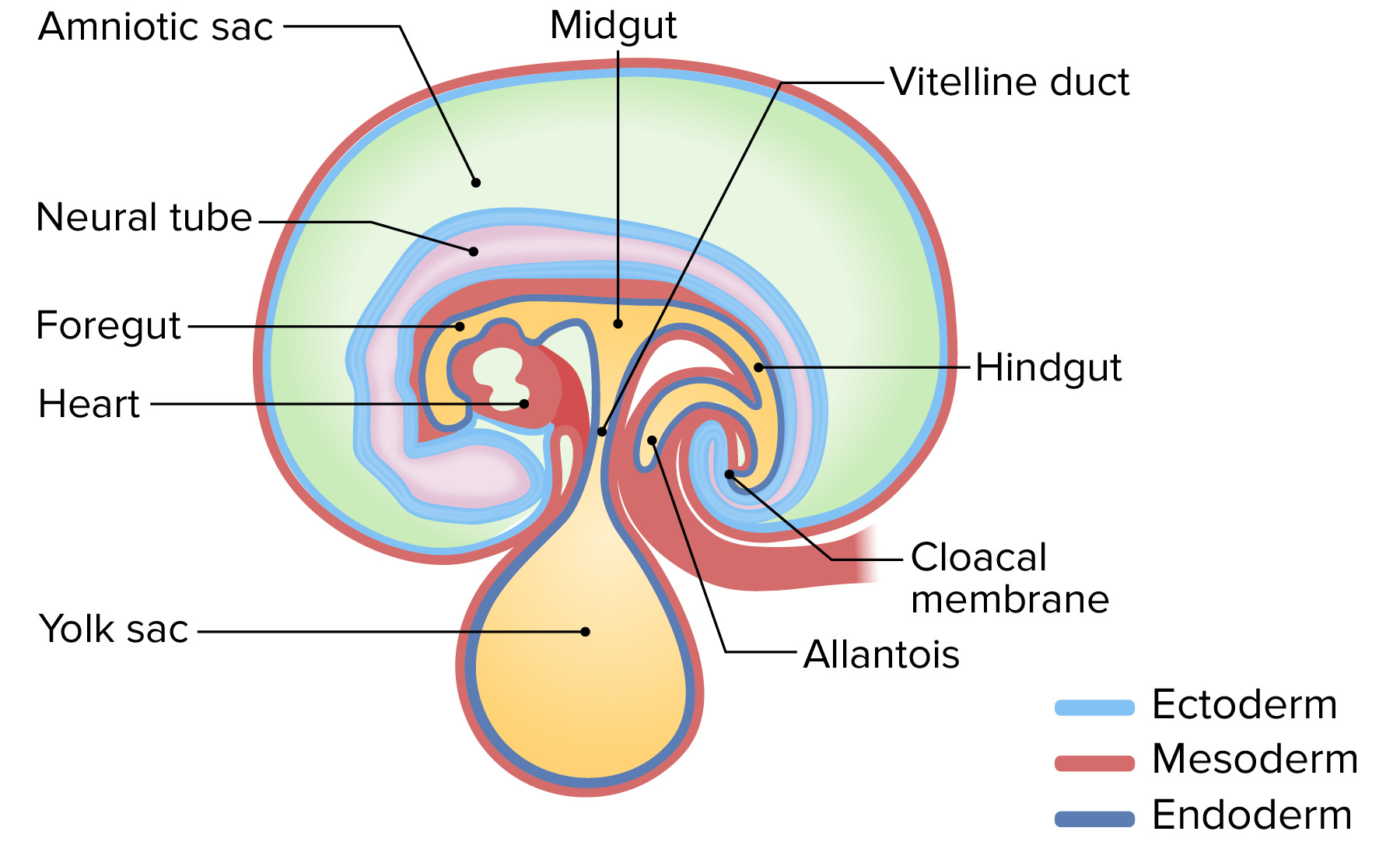
The early embryo with the amniotic sac above the embryo and the yolk sac below the embryo
Image by Lecturio.
Obliteration of the vitelline ductVitelline ductThe narrow tube connecting the yolk sac with the midgut of the embryo; persistence of all or part of it in post-fetal life produces abnormalities, of which the commonest is meckel diverticulum.Meckel’s Diverticulum and yolk sacYolk SacThe first of four extra-embryonic membranes to form during embryogenesis. In reptiles and birds, it arises from endoderm and mesoderm to incorporate the egg yolk into the digestive tract for nourishing the embryo. In placental mammals, its nutritional function is vestigial; however, it is the source of intestinal mucosa; blood cells; and germ cells. It is sometimes called the vitelline sac, which should not be confused with the vitelline membrane of the egg.Embryoblast and Trophoblast Development
As the embryoEmbryoThe entity of a developing mammal, generally from the cleavage of a zygote to the end of embryonic differentiation of basic structures. For the human embryo, this represents the first two months of intrauterine development preceding the stages of the fetus.Fertilization and First Week folds, the yolk sacYolk SacThe first of four extra-embryonic membranes to form during embryogenesis. In reptiles and birds, it arises from endoderm and mesoderm to incorporate the egg yolk into the digestive tract for nourishing the embryo. In placental mammals, its nutritional function is vestigial; however, it is the source of intestinal mucosa; blood cells; and germ cells. It is sometimes called the vitelline sac, which should not be confused with the vitelline membrane of the egg.Embryoblast and Trophoblast Development is pushed farther and farther away from the body.
Vitelline ductVitelline ductThe narrow tube connecting the yolk sac with the midgut of the embryo; persistence of all or part of it in post-fetal life produces abnormalities, of which the commonest is meckel diverticulum.Meckel’s Diverticulum: elongating stalk that connects the midgut to the yolk sacYolk SacThe first of four extra-embryonic membranes to form during embryogenesis. In reptiles and birds, it arises from endoderm and mesoderm to incorporate the egg yolk into the digestive tract for nourishing the embryo. In placental mammals, its nutritional function is vestigial; however, it is the source of intestinal mucosa; blood cells; and germ cells. It is sometimes called the vitelline sac, which should not be confused with the vitelline membrane of the egg.Embryoblast and Trophoblast Development as it is pushed away
The amniotic cavityAmniotic cavityEmbryoblast and Trophoblast Development starts on the dorsal side of the embryoEmbryoThe entity of a developing mammal, generally from the cleavage of a zygote to the end of embryonic differentiation of basic structures. For the human embryo, this represents the first two months of intrauterine development preceding the stages of the fetus.Fertilization and First Week
Grows and extends around the cranial and caudal ends of the embryoEmbryoThe entity of a developing mammal, generally from the cleavage of a zygote to the end of embryonic differentiation of basic structures. For the human embryo, this represents the first two months of intrauterine development preceding the stages of the fetus.Fertilization and First Week
Edges of the growing cavity meet on the ventral side at the abdomen → pinch off the yolk sacYolk SacThe first of four extra-embryonic membranes to form during embryogenesis. In reptiles and birds, it arises from endoderm and mesoderm to incorporate the egg yolk into the digestive tract for nourishing the embryo. In placental mammals, its nutritional function is vestigial; however, it is the source of intestinal mucosa; blood cells; and germ cells. It is sometimes called the vitelline sac, which should not be confused with the vitelline membrane of the egg.Embryoblast and Trophoblast Development/obliterate the vitelline ductVitelline ductThe narrow tube connecting the yolk sac with the midgut of the embryo; persistence of all or part of it in post-fetal life produces abnormalities, of which the commonest is meckel diverticulum.Meckel’s Diverticulum
Clinical relevance: Failure of the vitelline ductVitelline ductThe narrow tube connecting the yolk sac with the midgut of the embryo; persistence of all or part of it in post-fetal life produces abnormalities, of which the commonest is meckel diverticulum.Meckel’s Diverticulum to obliterate results in Meckel diverticulumDiverticulumA pouch or sac opening from the colon.Diverticular Disease:
A true diverticulumDiverticulumA pouch or sac opening from the colon.Diverticular Disease (contains all layers of the bowel wall)
Arises from the antimesenteric surface of the middle-to-distal ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy, anchoring it to the anterior abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen.
May lead to fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula, volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus, small bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis, and/or necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage
Overview of Gut Tube Differentiation
Structures derived from the gut tube
The primitive gut tube is formed from endodermEndodermThe inner of the three germ layers of an embryo.Gastrulation and Neurulation at the completion of lateral folding. The gut tube can initially be divided into 3 areas: foregut, midgut, and hindgut.
Note: This animation does not have sound.
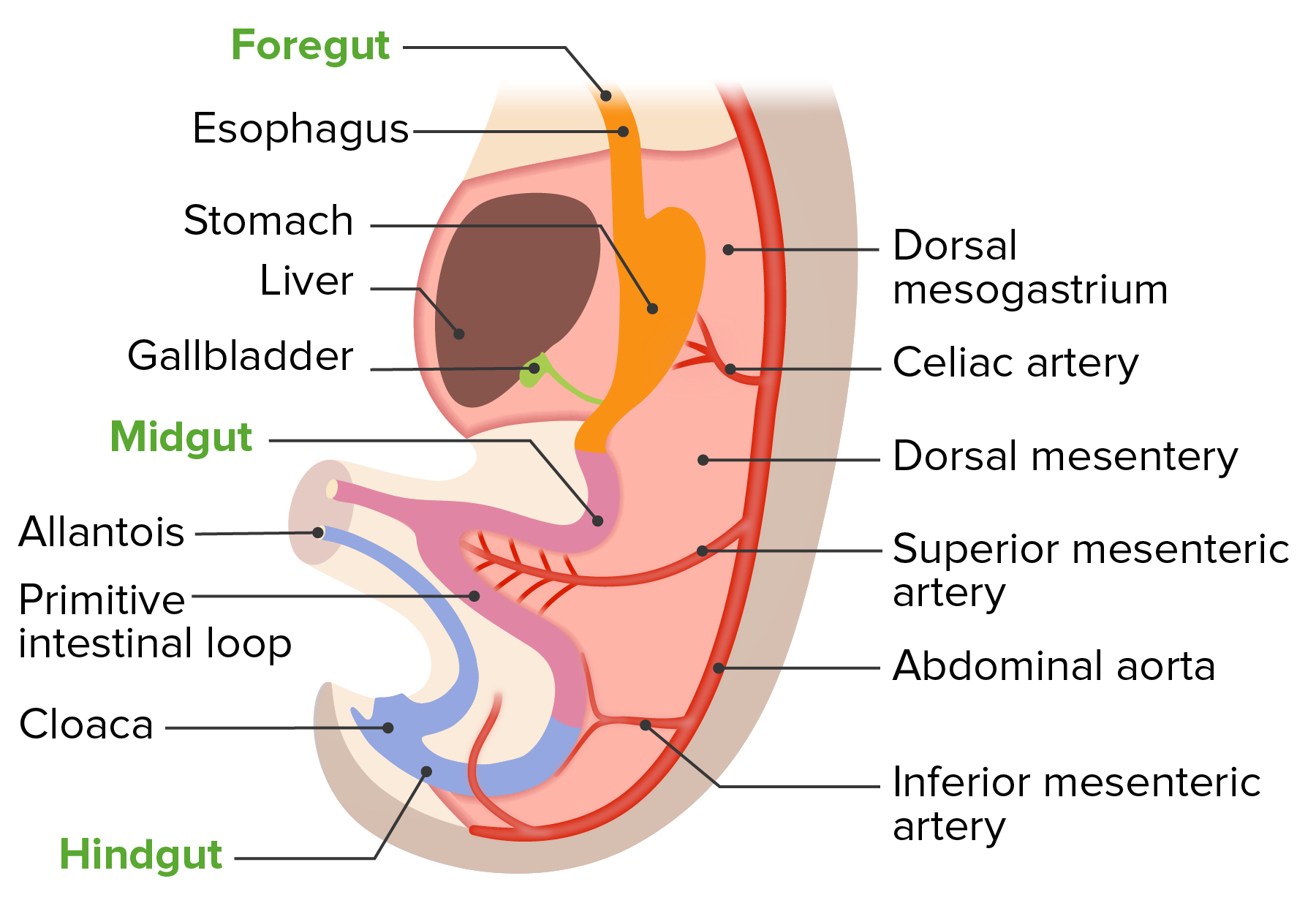
Foregut: abdominal derivatives supplied by celiac artery
EsophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy
StomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy
Proximal duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy (above the ampulla of Vater)
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy
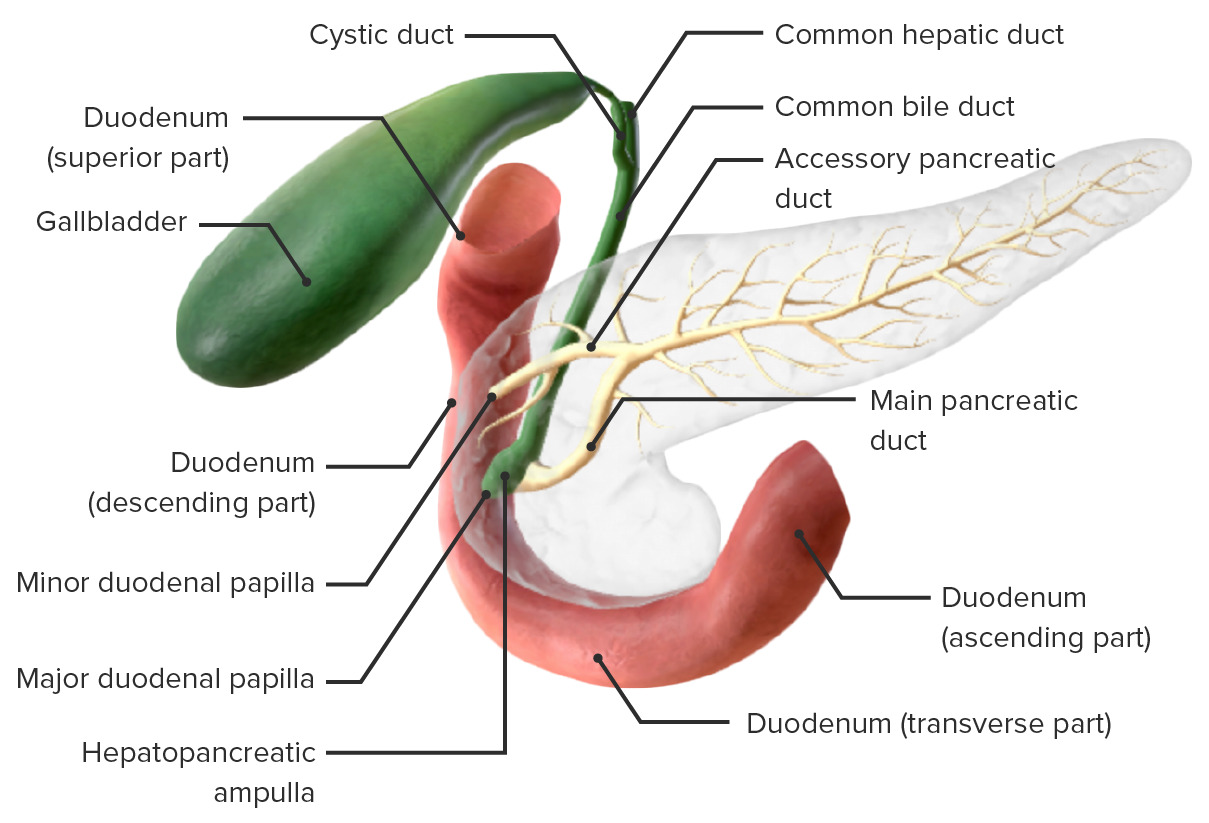
GallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy and bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy ducts
PancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy
Structures derived from the foregut above the abdomen:
Primordial pharynxPharynxThe pharynx is a component of the digestive system that lies posterior to the nasal cavity, oral cavity, and larynx. The pharynx can be divided into the oropharynx, nasopharynx, and laryngopharynx. Pharyngeal muscles play an integral role in vital processes such as breathing, swallowing, and speaking. Pharynx: Anatomy and its derivatives
Cervical and thoracic esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy
Respiratory tract
Midgut: derivatives supplied by the superior mesenteric arterySuperior mesenteric arteryA large vessel supplying the whole length of the small intestine except the superior part of the duodenum. It also supplies the cecum and the ascending part of the colon and about half the transverse part of the colon. It arises from the anterior surface of the aorta below the celiac artery at the level of the first lumbar vertebra.Small Intestine: Anatomy (SMA)
Distal duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy (below the ampulla of Vater)
JejunumJejunumThe middle portion of the small intestine, between duodenum and ileum. It represents about 2/5 of the remaining portion of the small intestine below duodenum.Small Intestine: Anatomy
IleumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy
CecumCecumThe blind sac or outpouching area of the large intestine that is below the entrance of the small intestine. It has a worm-like extension, the vermiform appendix.Colon, Cecum, and Appendix: Anatomy
Ascending colonAscending colonThe segment of large intestine between the cecum and the transverse colon. It passes cephalad from the cecum to the caudal surface of the right lobe of the liver where it bends sharply to the left, forming the right colic flexure.Colon, Cecum, and Appendix: Anatomy
Proximal ⅔ of the transverse colonTransverse colonThe segment of large intestine between ascending colon and descending colon. It passes from the right colic flexure across the abdomen, then turns sharply at the left colonic flexure into the descending colon.Colon, Cecum, and Appendix: Anatomy
Hindgut: derivatives supplied by the inferior mesenteric arteryInferior mesenteric arteryThe artery supplying nearly all the left half of the transverse colon, the whole of the descending colon, the sigmoid colon, and the greater part of the rectum. It is smaller than the superior mesenteric artery and arises from the aorta above its bifurcation into the common iliac arteries.Small Intestine: Anatomy (IMA)
Distal ⅓ of the transverse colonTransverse colonThe segment of large intestine between ascending colon and descending colon. It passes from the right colic flexure across the abdomen, then turns sharply at the left colonic flexure into the descending colon.Colon, Cecum, and Appendix: Anatomy
SigmoidSigmoidA segment of the colon between the rectum and the descending colon.VolvuluscolonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy
RectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy
Superior portion of the anal canal
Development of the dorsal mesentery with the primitive gut tube
Key structures derived from endodermEndodermThe inner of the three germ layers of an embryo.Gastrulation and Neurulation related to development of the abdominal organs:
Epithelial lining of the entire GI tract
Mucosal and submucosal glands
Structures derived from mesodermMesodermThe middle germ layer of an embryo derived from three paired mesenchymal aggregates along the neural tube.Gastrulation and Neurulation
Key structures derived from mesodermMesodermThe middle germ layer of an embryo derived from three paired mesenchymal aggregates along the neural tube.Gastrulation and Neurulation related to development of the abdominal organs:
Splanchnic layer of the LPM:
Alimentary canal wall (i.e., intestinal walls)
Muscular tissue (e.g., circular and longitudinal layers, sphincters)
Connective tissueConnective tissueConnective tissues originate from embryonic mesenchyme and are present throughout the body except inside the brain and spinal cord. The main function of connective tissues is to provide structural support to organs. Connective tissues consist of cells and an extracellular matrix.Connective Tissue: Histology
MesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomy of the small intestineSmall intestineThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum. Small Intestine: Anatomy
Transverse and sigmoidSigmoidA segment of the colon between the rectum and the descending colon.Volvulus mesocolon
Numerous named abdominal ligaments
Somatic layer of the LPM: parietalParietalOne of a pair of irregularly shaped quadrilateral bones situated between the frontal bone and occipital bone, which together form the sides of the cranium.Skull: AnatomyperitoneumPeritoneumThe peritoneum is a serous membrane lining the abdominopelvic cavity. This lining is formed by connective tissue and originates from the mesoderm. The membrane lines both the abdominal walls (as parietal peritoneum) and all of the visceral organs (as visceral peritoneum).Peritoneum: Anatomy
Key structures derived from ectodermEctodermThe outer of the three germ layers of an embryo.Gastrulation and Neurulation related to development of the abdominal organs:
At the cranial and caudal ends, the ectodermEctodermThe outer of the three germ layers of an embryo.Gastrulation and Neurulation and endodermEndodermThe inner of the three germ layers of an embryo.Gastrulation and Neurulation meet (with no mesodermMesodermThe middle germ layer of an embryo derived from three paired mesenchymal aggregates along the neural tube.Gastrulation and Neurulation between) forming membranes that will ultimately rupture, becoming the openings of the GI tract
Cranial end: oropharyngeal membrane → mouth
Caudal end: cloacal membrane → anus
EpitheliumEpitheliumThe epithelium is a complex of specialized cellular organizations arranged into sheets and lining cavities and covering the surfaces of the body. The cells exhibit polarity, having an apical and a basal pole. Structures important for the epithelial integrity and function involve the basement membrane, the semipermeable sheet on which the cells rest, and interdigitations, as well as cellular junctions. Surface Epithelium: Histology: lines the distal anal canal
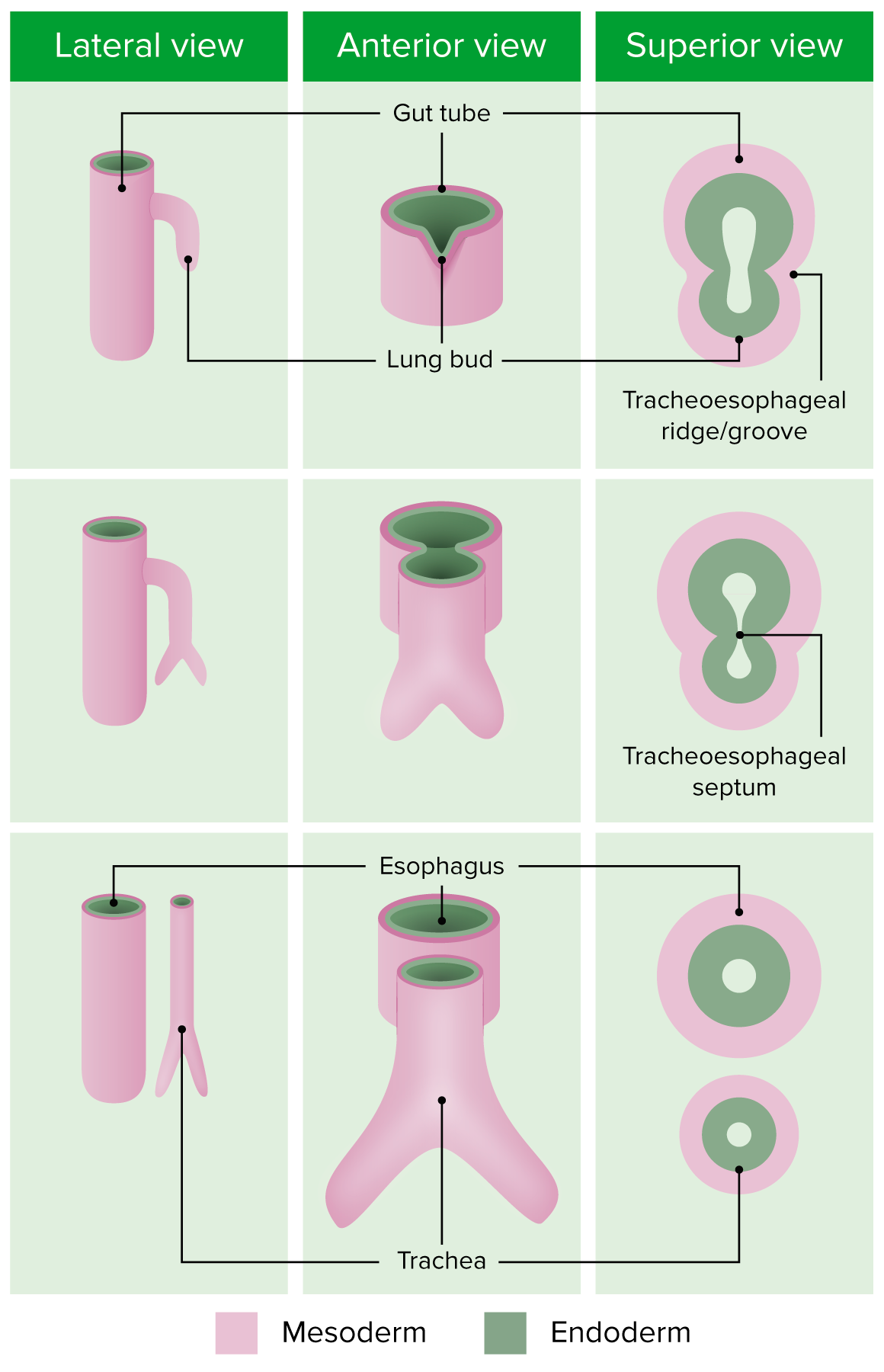
EsophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy
The tracheoesophageal septum creates 2 separate tubes:
EsophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy (posteriorly, from the original foregut)
TracheaTracheaThe trachea is a tubular structure that forms part of the lower respiratory tract. The trachea is continuous superiorly with the larynx and inferiorly becomes the bronchial tree within the lungs. The trachea consists of a support frame of semicircular, or C-shaped, rings made out of hyaline cartilage and reinforced by collagenous connective tissue. Trachea: Anatomy (anteriorly, from the lung budLung budDevelopment of the Respiratory System)
Clinical relevance:
Tracheoesophageal fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula (TEF): occurs when the tracheoesophageal grooves fail to fully close in the midline
Esophageal atresiaAtresiaHypoplastic Left Heart Syndrome (HLHS): portions of the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy fail to form; often coexists with TEF
Growth and descent:
EsophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy lengthens and descends together with the heart and lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy
StomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy
Development begins around the 4th week
Fusiform dilation of the foregut: site of primordial stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy
The lengthening esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy places the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy below the diaphragmDiaphragmThe diaphragm is a large, dome-shaped muscle that separates the thoracic cavity from the abdominal cavity. The diaphragm consists of muscle fibers and a large central tendon, which is divided into right and left parts. As the primary muscle of inspiration, the diaphragm contributes 75% of the total inspiratory muscle force.Diaphragm: Anatomy
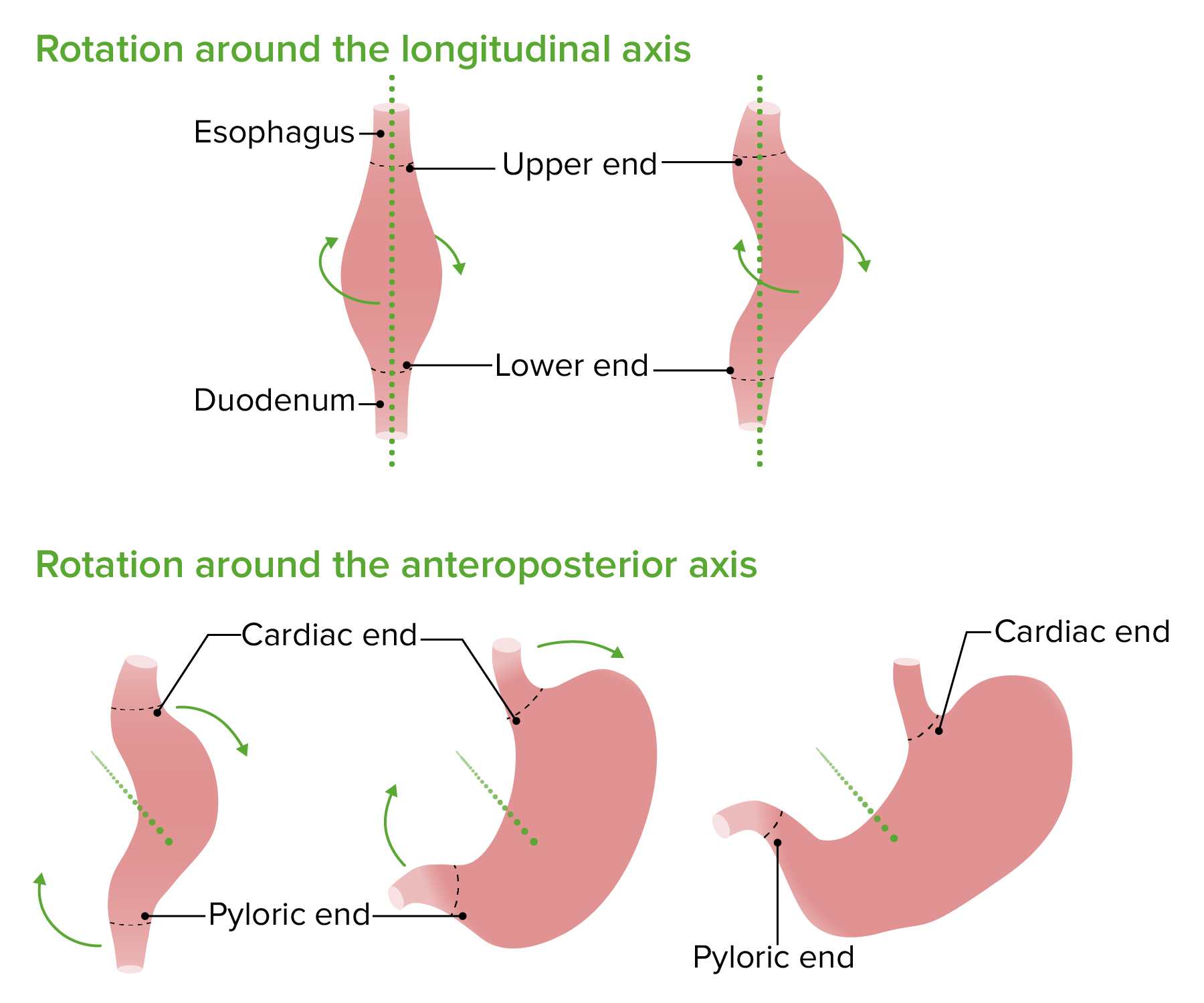
Posterior wall grows more quickly than anterior wall → develops a C shape
90-degree rotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays clockwise around longitudinal axis:
Left vagus nerveVagus nerveThe 10th cranial nerve. The vagus is a mixed nerve which contains somatic afferents (from skin in back of the ear and the external auditory meatus), visceral afferents (from the pharynx, larynx, thorax, and abdomen), parasympathetic efferents (to the thorax and abdomen), and efferents to striated muscle (of the larynx and pharynx).Pharynx: Anatomy innervates anterior wall
Right vagus nerveVagus nerveThe 10th cranial nerve. The vagus is a mixed nerve which contains somatic afferents (from skin in back of the ear and the external auditory meatus), visceral afferents (from the pharynx, larynx, thorax, and abdomen), parasympathetic efferents (to the thorax and abdomen), and efferents to striated muscle (of the larynx and pharynx).Pharynx: Anatomy innervates posterior wall
Smaller rotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays clockwise around the anteroposterior axis:
Cardiac portion of the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy moves down and to the left
Pyloric portion moves up and to the right
The stomach rotates clockwise 1st along its longitudinal axis and then along its anteroposterior axis:
The original dorsal side of the stomach grows faster than the original ventral side, creating the greater and lesser curvatures of the stomach.
Image by Lecturio.
A closer look at the rotation of the stomach clearly explains why the left vagus nerve contributes more heavily to the anterior vagal trunk and the right vagus nerve to the posterior vagal trunk.
Image by Lecturio.
Omenta
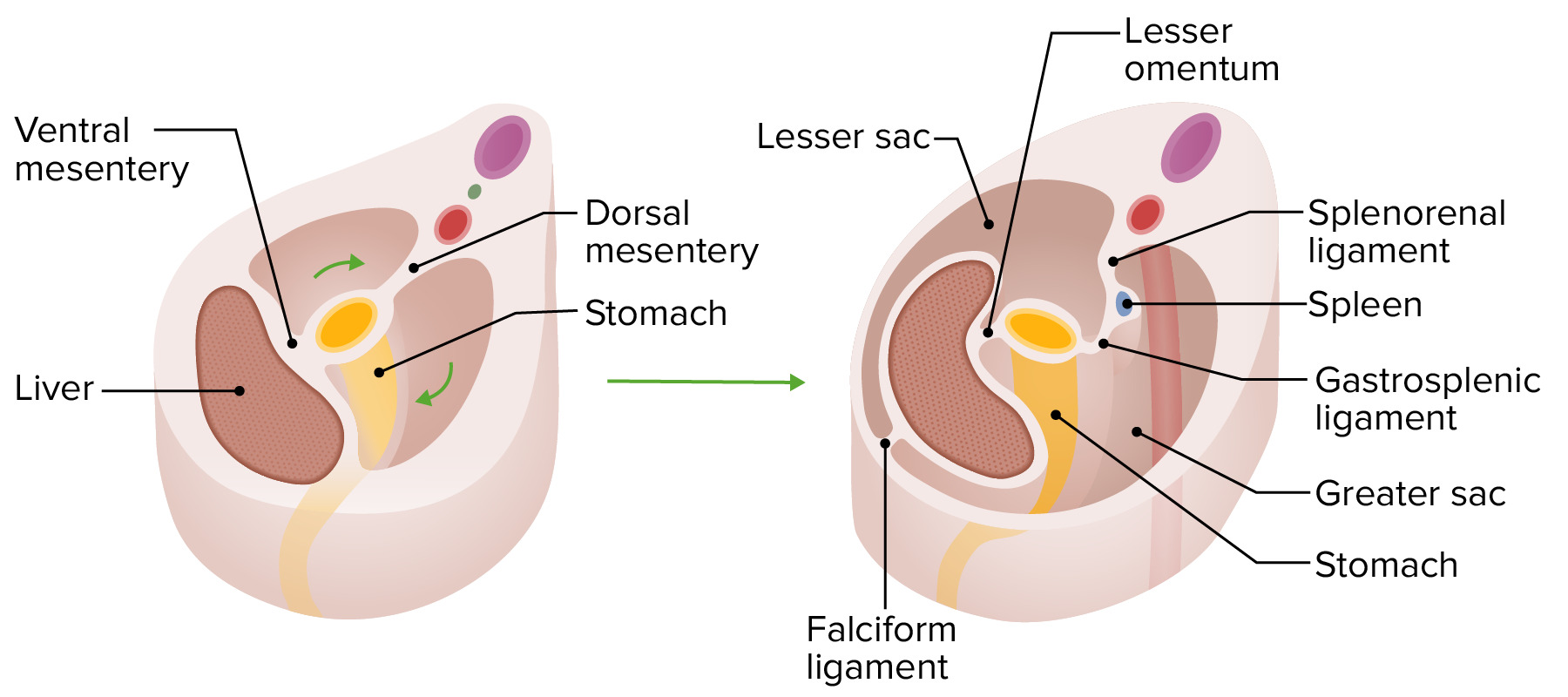
The greater and lesser omenta are formed from the dorsal and ventral mesogastrium (of mesodermal origin). As they rotate with the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy, they create the greater and lesser sacs.
Dorsal mesogastrium:
Suspends stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy from the dorsal wall
Originally located in the median plane
Moved to the left during 90-degree longitudinal rotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays
Creates a space posterior to the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy called the lesser sac (i.e., omental bursa)
Forms several important structures:
After rotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays of the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy, bulges down to form the greater omentumOmentumPeritoneum: Anatomy
Gastrosplenic ligamentGastrosplenic ligamentSpleen: Anatomy: connects the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy and spleenSpleenThe spleen is the largest lymphoid organ in the body, located in the LUQ of the abdomen, superior to the left kidney and posterior to the stomach at the level of the 9th-11th ribs just below the diaphragm. The spleen is highly vascular and acts as an important blood filter, cleansing the blood of pathogens and damaged erythrocytes. Spleen: Anatomy
Splenorenal ligamentSplenorenal ligamentSpleen: Anatomy: connects the spleenSpleenThe spleen is the largest lymphoid organ in the body, located in the LUQ of the abdomen, superior to the left kidney and posterior to the stomach at the level of the 9th-11th ribs just below the diaphragm. The spleen is highly vascular and acts as an important blood filter, cleansing the blood of pathogens and damaged erythrocytes. Spleen: Anatomy to the posterior abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen (near the kidney)
Structures developing within the dorsal mesogastrium:
SpleenSpleenThe spleen is the largest lymphoid organ in the body, located in the LUQ of the abdomen, superior to the left kidney and posterior to the stomach at the level of the 9th-11th ribs just below the diaphragm. The spleen is highly vascular and acts as an important blood filter, cleansing the blood of pathogens and damaged erythrocytes. Spleen: Anatomy
PancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy
Ventral mesogastrium:
Attached to the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy, duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy, liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy, and ventral abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen
Originally located in the median plane
Moved to the right during 90-degree longitudinal rotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays
Closes off the lesser sac between the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy and liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy
Forms 2 primary structures:
Lesser omentumOmentumPeritoneum: Anatomy: connects the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy and liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy
Falciform ligamentFalciform LigamentLiver: Anatomy: connects the liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy and the anterior abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen
Structures developing within the ventral mesogastrium:
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy
GallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy
BileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy ducts
Rotation of the stomach and gastric mesenteries
Image by Lecturio.
DuodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy
Development begins in the 4th week
Above the ampulla of Vater: derived from caudal part of theforegut → supplied by the celiac artery
Below the ampulla of Vater: derived from cranial part of the midgut → supplied by SMA
Elongates and forms C-shaped loop
Joins together with the developing pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy attached to the posterior body wall
Duodenal obliteration and recanalization:
Week 5: rapid cell proliferation in its walls leads to complete obstruction of the duodenal lumen
By the end of week 8:
Vacuoles form within the duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy
Vacuoles grow and merge → lumen recanalization
Clinical relevance: failure of the lumen to fully recanalize results in either:
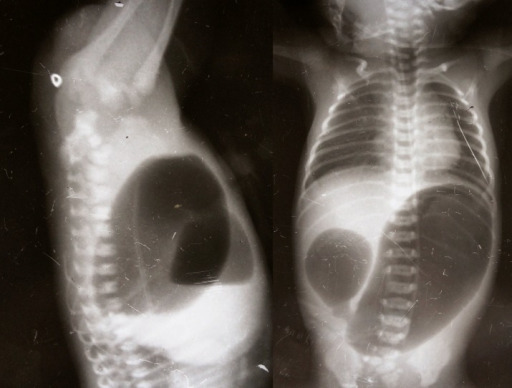
Double-bubble sign on radiography (invertography) indicating duodenal obstruction: The smaller bubble on the individual’s right is air in the duodenum, and the larger bubble on the left is air in the stomach.
Image: “Invertogram showing high ARM and AP view showing duodenal atresia” by Department of Pediatric Surgery, Gauhati Medical College, GUWAHATI, ASSAM, INDIA. License: CC BY 3.0
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy and biliary ducts
Development begins in the 3rd‒4th week
Appears from the caudal portion of the foregut as the hepatic diverticulumDiverticulumA pouch or sac opening from the colon.Diverticular Disease, which goes on to form the:
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy (endodermEndodermThe inner of the three germ layers of an embryo.Gastrulation and Neurulation differentiates into hepatocytesHepatocytesThe main structural component of the liver. They are specialized epithelial cells that are organized into interconnected plates called lobules.Liver: Anatomy)
Intrahepatic ducts
Extrahepatic portions of the hepatic ducts
As the hepatic diverticulumDiverticulumA pouch or sac opening from the colon.Diverticular Disease enlarges, the connection to the duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy narrows → common bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy duct
A smaller bud grows off the caudal side of the hepatic diverticulumDiverticulumA pouch or sac opening from the colon.Diverticular Disease:
Forms the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy
Connection between the caudal bud and the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy → cysticCysticFibrocystic Change duct
The hepatic diverticulumDiverticulumA pouch or sac opening from the colon.Diverticular Disease grows into the ventral mesogastrium.
Weeks 5–9:
Hematopoietic stem cellsHematopoietic stem cellsProgenitor cells from which all blood cells derived. They are found primarily in the bone marrow and also in small numbers in the peripheral blood.Bone Marrow: Composition and Hematopoiesis (mesodermal origin) migrate into the liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy:
HematopoiesisHematopoiesisThe development and formation of various types of blood cells. Hematopoiesis can take place in the bone marrow (medullary) or outside the bone marrow (extramedullary hematopoiesis).Bone Marrow: Composition and Hematopoiesis begins
LiverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy is the primary site of hematopoiesisHematopoiesisThe development and formation of various types of blood cells. Hematopoiesis can take place in the bone marrow (medullary) or outside the bone marrow (extramedullary hematopoiesis).Bone Marrow: Composition and Hematopoiesis up until about 28 weeks, when the primary job is taken over by the bone marrowBone marrowThe soft tissue filling the cavities of bones. Bone marrow exists in two types, yellow and red. Yellow marrow is found in the large cavities of large bones and consists mostly of fat cells and a few primitive blood cells. Red marrow is a hematopoietic tissue and is the site of production of erythrocytes and granular leukocytes. Bone marrow is made up of a framework of connective tissue containing branching fibers with the frame being filled with marrow cells.Bone Marrow: Composition and Hematopoiesis.
Week 12: beginning of bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: AnatomysecretionSecretionCoagulation Studies by hepatocytesHepatocytesThe main structural component of the liver. They are specialized epithelial cells that are organized into interconnected plates called lobules.Liver: Anatomy
PancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy
Development begins in the 4th week
Develops primarily from a dorsal pancreatic bud off the foregut:
Tail of the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy
A smaller ventral pancreatic bud contributes to the:
By week 13: alpha, beta, and delta cells present in islets
SpleenSpleenThe spleen is the largest lymphoid organ in the body, located in the LUQ of the abdomen, superior to the left kidney and posterior to the stomach at the level of the 9th-11th ribs just below the diaphragm. The spleen is highly vascular and acts as an important blood filter, cleansing the blood of pathogens and damaged erythrocytes. Spleen: Anatomy
Development begins in the 5th week
Derived from mesenchymal cells (i.e., from mesodermMesodermThe middle germ layer of an embryo derived from three paired mesenchymal aggregates along the neural tube.Gastrulation and Neurulation, not the endoderm-derived foregut)
Forms from mesenchymal buds off the dorsal mesogastrium
Buds fuse together, forming the spleenSpleenThe spleen is the largest lymphoid organ in the body, located in the LUQ of the abdomen, superior to the left kidney and posterior to the stomach at the level of the 9th-11th ribs just below the diaphragm. The spleen is highly vascular and acts as an important blood filter, cleansing the blood of pathogens and damaged erythrocytes. Spleen: Anatomy.
The midgut develops into the lining of the GI tract from the distal duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy (below the ampulla of Vater) to the midtransverse colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy. The hindgut develops into the GI tract from the distal ⅓ of the transverse colonTransverse colonThe segment of large intestine between ascending colon and descending colon. It passes from the right colic flexure across the abdomen, then turns sharply at the left colonic flexure into the descending colon.Colon, Cecum, and Appendix: Anatomy through the anus.
Midgut milestones
Cranial portion: grows rapidly and forms small intestinal loop
Unequal growth of cecal walls → appendixAppendixA worm-like blind tube extension from the cecum.Colon, Cecum, and Appendix: Anatomy enters the cecumCecumThe blind sac or outpouching area of the large intestine that is below the entrance of the small intestine. It has a worm-like extension, the vermiform appendix.Colon, Cecum, and Appendix: Anatomy medially
Week 5: obliteration of the vitelline ductVitelline ductThe narrow tube connecting the yolk sac with the midgut of the embryo; persistence of all or part of it in post-fetal life produces abnormalities, of which the commonest is meckel diverticulum.Meckel’s Diverticulum (yolk sacYolk SacThe first of four extra-embryonic membranes to form during embryogenesis. In reptiles and birds, it arises from endoderm and mesoderm to incorporate the egg yolk into the digestive tract for nourishing the embryo. In placental mammals, its nutritional function is vestigial; however, it is the source of intestinal mucosa; blood cells; and germ cells. It is sometimes called the vitelline sac, which should not be confused with the vitelline membrane of the egg.Embryoblast and Trophoblast Development is pinched off from the midgut)
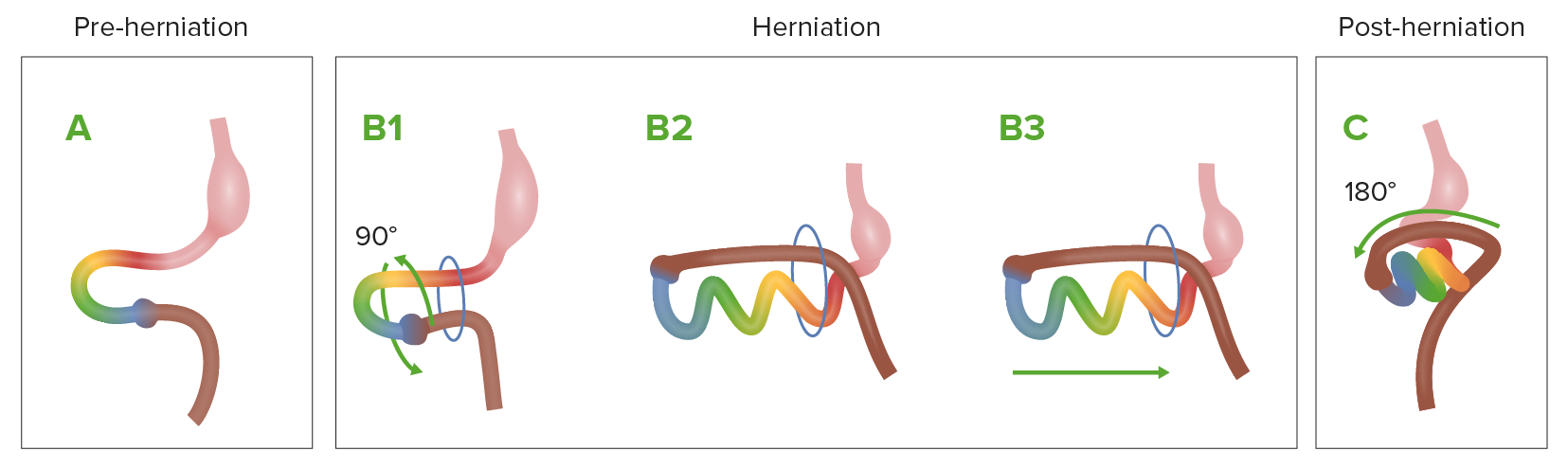
Week 6: physiologic herniationHerniationOmphalocele of the midgut through the umbilicus
The midgut naturally herniates through the umbilical ring.
Creates more space within the embryoEmbryoThe entity of a developing mammal, generally from the cleavage of a zygote to the end of embryonic differentiation of basic structures. For the human embryo, this represents the first two months of intrauterine development preceding the stages of the fetus.Fertilization and First Week for the the developing abdominal organs (especially the liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy)
Weeks 6–10:
Rapid growth of the midgut occurs outside the embryoEmbryoThe entity of a developing mammal, generally from the cleavage of a zygote to the end of embryonic differentiation of basic structures. For the human embryo, this represents the first two months of intrauterine development preceding the stages of the fetus.Fertilization and First Week
RotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays:
Midgut rotates 270 degrees counterclockwise around SMA.
Pulls the small intestineSmall intestineThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum. Small Intestine: Anatomy into mature anatomic position: jejunumJejunumThe middle portion of the small intestine, between duodenum and ileum. It represents about 2/5 of the remaining portion of the small intestine below duodenum.Small Intestine: Anatomy begins in the LUQ
Pulls the large intestineLarge intestineThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy into its mature anatomic position: upside-down U shape surrounding the small intestines
Week 10: midgut returns to the abdominal cavity
Growing abdominal cavity creates enough space for the developing midgut
Clinical relevance: Failure of the midgut to reenter the abdomen results in an omphaloceleOmphaloceleOmphalocele is a congenital anterior abdominal wall defect in which the intestines are covered by peritoneum and amniotic membranes. The condition results from the failure of the midgut to return to the abdominal cavity by 10 weeks’ gestation. Omphalocele (a congenital anterior abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen defect in which the intestines are covered by peritoneumPeritoneumThe peritoneum is a serous membrane lining the abdominopelvic cavity. This lining is formed by connective tissue and originates from the mesoderm. The membrane lines both the abdominal walls (as parietal peritoneum) and all of the visceral organs (as visceral peritoneum).Peritoneum: Anatomy and amniotic membranes).
Diagram showing the normal process of intestinal rotation and herniation during embryologic development A: The midgut (multicolored loop) before herniation. B1–B3: As it grows rapidly, the midgut herniates through the umbilical ring and starts rotation. C: The midgut returns to the abdominal cavity.
Image by Lecturio.
Hindgut milestones
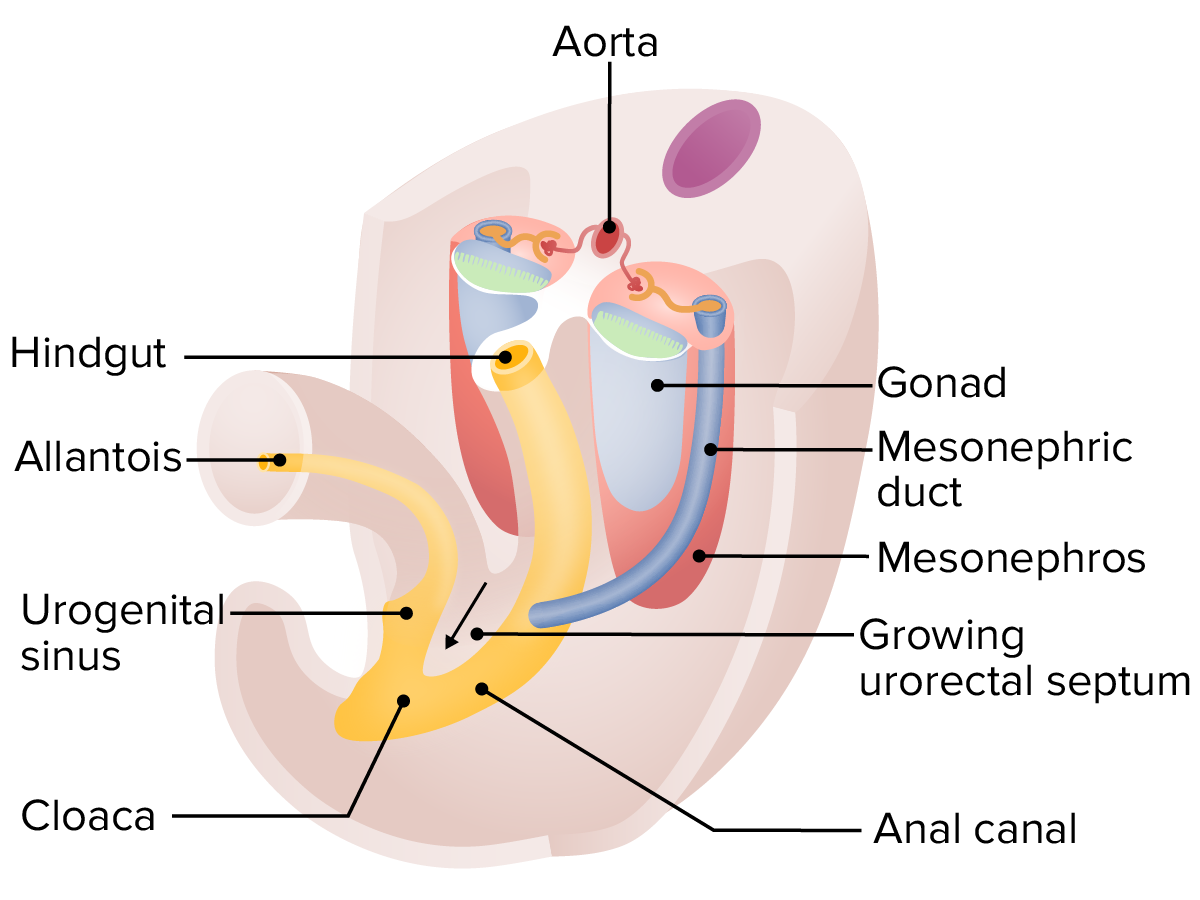
The hindgut develops simultaneously and in close association with the urogenital system.
Cloaca:
Distal portion of the hindgut
Adjacent to the “outside” of the developing embryoEmbryoThe entity of a developing mammal, generally from the cleavage of a zygote to the end of embryonic differentiation of basic structures. For the human embryo, this represents the first two months of intrauterine development preceding the stages of the fetus.Fertilization and First Week at the cloacal membrane, which:
Early in development, empties into a drainage tube called the allantois
Allantois:
Drains both gut tube and developing urinary system early
Travels through umbilical cordUmbilical cordThe flexible rope-like structure that connects a developing fetus to the placenta in mammals. The cord contains blood vessels which carry oxygen and nutrients from the mother to the fetus and waste products away from the fetus.Placenta, Umbilical Cord, and Amniotic Cavity
Called the urachus later in development
Ultimately obliterates, becoming the median umbilical ligament along the internal anterior abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen
Clinical relevance: incomplete obliteration can lead to a urachal fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula (infants may leak urine from the umbilicus at birth)
Weeks 4‒7: cloaca divided by a growing urorectal septum:
Starts at the superior/proximal portion of the cloaca → grows distally until it reaches the outside of the body, where it becomes the perineal body
Separates the cloaca into 2 structures:
Urogenital sinusUrogenital SinusCongenital Malformations of the Female Reproductive System (anterior/superior): connects to the uretersUretersOne of a pair of thick-walled tubes that transports urine from the kidney pelvis to the urinary bladder.Urinary Tract: Anatomy; develops into the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess, prostateProstateThe prostate is a gland in the male reproductive system. The gland surrounds the bladder neck and a portion of the urethra. The prostate is an exocrine gland that produces a weakly acidic secretion, which accounts for roughly 20% of the seminal fluid. (males), and urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy
Anal canal (posterior/inferior)
Clinical relevance: Failure of the anorectal septum to completely divide the cloaca can result in fistulas between the urogenital system and the anorectum.
Imperforate anus: failure of the cloacal membrane to rupture
Anal atresiaAtresiaHypoplastic Left Heart Syndrome (HLHS): failure of the anal pit to form/meet rectumRectumThe rectum and anal canal are the most terminal parts of the lower GI tract/large intestine that form a functional unit and control defecation. Fecal continence is maintained by several important anatomic structures including rectal folds, anal valves, the sling-like puborectalis muscle, and internal and external anal sphincters. Rectum and Anal Canal: Anatomy; more complicated repair because there are no sphincter muscles
Hindgut/endoderm-derived: proximal ⅔ of the anal canal, lined by columnar epithelial cells
Ectoderm-derived: distal ⅓ of the anal canal, lined by stratified squamous epithelial cells
Hindgut is supplied by the IMA
Between weeks 4 and 7, the urorectal septum begins growing into the cloaca, starting at its proximal end and growing distally until it reaches the outside of the embryo, fully separating the cloaca into the urogenital sinus and the anal canal.
GastroschisisGastroschisisGastroschisis is a congenital abdominal wall defect characterized by the complete lack of closure of the abdominal musculature. A portion of intestine does not return to the abdominal cavity, thereby remaining in its early embryonic herniated state but with no coverings. Gastroschisis (see GastroschisisGastroschisisGastroschisis is a congenital abdominal wall defect characterized by the complete lack of closure of the abdominal musculature. A portion of intestine does not return to the abdominal cavity, thereby remaining in its early embryonic herniated state but with no coverings. Gastroschisis): defect caused by incomplete lateral folding of trilaminar embryoEmbryoThe entity of a developing mammal, generally from the cleavage of a zygote to the end of embryonic differentiation of basic structures. For the human embryo, this represents the first two months of intrauterine development preceding the stages of the fetus.Fertilization and First Week, resulting in an incomplete “tube.” This incomplete tube results in a defect in the abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen; the intestines will be free floating in the amniotic sac, not covered by peritoneumPeritoneumThe peritoneum is a serous membrane lining the abdominopelvic cavity. This lining is formed by connective tissue and originates from the mesoderm. The membrane lines both the abdominal walls (as parietal peritoneum) and all of the visceral organs (as visceral peritoneum).Peritoneum: Anatomy.
OmphaloceleOmphaloceleOmphalocele is a congenital anterior abdominal wall defect in which the intestines are covered by peritoneum and amniotic membranes. The condition results from the failure of the midgut to return to the abdominal cavity by 10 weeks’ gestation. Omphalocele: failure of midgut to reenter abdomen after physiologic herniationHerniationOmphalocele. This failure results in a congenital anterior abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen defect where the intestines are covered by peritoneumPeritoneumThe peritoneum is a serous membrane lining the abdominopelvic cavity. This lining is formed by connective tissue and originates from the mesoderm. The membrane lines both the abdominal walls (as parietal peritoneum) and all of the visceral organs (as visceral peritoneum).Peritoneum: Anatomy and amniotic membranes.
Esophageal atresiaAtresiaHypoplastic Left Heart Syndrome (HLHS): portions of the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy fail to fully form. Esophageal atresiaAtresiaHypoplastic Left Heart Syndrome (HLHS) often coexists with a tracheoesophageal fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula.
Tracheoesophageal fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula: connection between the tracheaTracheaThe trachea is a tubular structure that forms part of the lower respiratory tract. The trachea is continuous superiorly with the larynx and inferiorly becomes the bronchial tree within the lungs. The trachea consists of a support frame of semicircular, or C-shaped, rings made out of hyaline cartilage and reinforced by collagenous connective tissue. Trachea: Anatomy and esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy. This fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula occurs when the tracheoesophageal grooves fail to fully close in the midline (which should normally separate the tracheaTracheaThe trachea is a tubular structure that forms part of the lower respiratory tract. The trachea is continuous superiorly with the larynx and inferiorly becomes the bronchial tree within the lungs. The trachea consists of a support frame of semicircular, or C-shaped, rings made out of hyaline cartilage and reinforced by collagenous connective tissue. Trachea: Anatomy from the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy). Tracheoesophageal fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula is often associated with esophageal atresiaAtresiaHypoplastic Left Heart Syndrome (HLHS). Multiple different anatomic variations are possible.
Hypertrophic pyloric stenosisStenosisHypoplastic Left Heart Syndrome (HLHS): narrowing of the pylorusPylorusThe region between the sharp indentation at the lower third of the stomach (incisura angularis) and the junction of the pylorus with the duodenum. Pyloric antral glands contain mucus-secreting cells and gastrin-secreting endocrine cells (g cells).Stomach: Anatomy of the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy due to the thickening of its pyloric sphincter muscle. Hypertrophic pyloric stenosisStenosisHypoplastic Left Heart Syndrome (HLHS) presents clinically with nonbilious vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia and an olive-shaped massOlive-Shaped MassHypertrophic Pyloric Stenosis in the epigastric regionEpigastric regionAnterior Abdominal Wall: Anatomy.
Congenital defects of duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy: failure of the duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy to fully recanalize, leading to either stenosisStenosisHypoplastic Left Heart Syndrome (HLHS) (narrowing) or obstruction. Duodenal atresiaAtresiaHypoplastic Left Heart Syndrome (HLHS) presents with bilious vomitingBilious VomitingCongenital Duodenal Obstruction, and a double-bubble sign can be seen on x-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests; this defect is associated with Down syndromeDown syndromeDown syndrome, or trisomy 21, is the most common chromosomal aberration and the most frequent genetic cause of developmental delay. Both boys and girls are affected and have characteristic craniofacial and musculoskeletal features, as well as multiple medical anomalies involving the cardiac, gastrointestinal, ocular, and auditory systems.Down syndrome (Trisomy 21).
AnnularAnnularDermatologic ExaminationpancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy(see PancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy): results from the growth of the pancreatic bud around the duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy, which forms a pancreatic ring. May cause duodenal obstruction. Women are affected more frequently than men.
PancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy divisum (see PancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy): occurs when the ventral and dorsal ducts of the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy fail to fuse together to form the main pancreatic ductMain pancreatic ductPancreas: Anatomy during the 8th week. May predispose individual to chronic pancreatic painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways.
Accessory spleens (see SpleenSpleenThe spleen is the largest lymphoid organ in the body, located in the LUQ of the abdomen, superior to the left kidney and posterior to the stomach at the level of the 9th-11th ribs just below the diaphragm. The spleen is highly vascular and acts as an important blood filter, cleansing the blood of pathogens and damaged erythrocytes. Spleen: Anatomy): numerous splenic masses with functioning splenic tissue, which can occur when splenic buds fail to fully fuse. An accessory spleenAccessory SpleenImaging of the Spleen usually exists near the hilumHilumLungs: Anatomy of the spleenSpleenThe spleen is the largest lymphoid organ in the body, located in the LUQ of the abdomen, superior to the left kidney and posterior to the stomach at the level of the 9th-11th ribs just below the diaphragm. The spleen is highly vascular and acts as an important blood filter, cleansing the blood of pathogens and damaged erythrocytes. Spleen: Anatomy or the tail of the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy.
Intestinal malrotationMalrotationPediatric Gastrointestinal Abnormalities: failure of the GI tract to undergo normal rotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays around the mesenteric vessels during embryologic development. Intestinal malrotationMalrotationPediatric Gastrointestinal Abnormalities can result in a number of anatomic patterns characterized by abnormal location and attachments of the intestines within the abdominal cavity. These anomalies can be clinically silent or present with a number of complications, the most catastrophic of which is midgut volvulusMidgut VolvulusIntestinal Malrotation.
VolvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus: twisting or axialAxialComputed Tomography (CT)rotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays of a portion of bowel around its mesenteryMesenteryA layer of the peritoneum which attaches the abdominal viscera to the abdominal wall and conveys their blood vessels and nerves.Peritoneum: Anatomy. The most common site of volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus encountered in adults is the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy. Presentation is typically with symptoms of bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis, such as abdominal painAbdominal PainAcute Abdomen, distention, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia and constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation/obstipationObstipationLarge Bowel Obstruction.
Meckel diverticulumDiverticulumA pouch or sac opening from the colon.Diverticular Disease: failure of the vitelline ductVitelline ductThe narrow tube connecting the yolk sac with the midgut of the embryo; persistence of all or part of it in post-fetal life produces abnormalities, of which the commonest is meckel diverticulum.Meckel’s Diverticulum to obliterate, resulting in a “true” diverticulumDiverticulumA pouch or sac opening from the colon.Diverticular Disease, meaning that the outpouching from the ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy contains all layers of the bowel wall. (In a “false” diverticulumDiverticulumA pouch or sac opening from the colon.Diverticular Disease, only the mucosa and submucosa protrude.) These diverticula arise from the antimesenteric surface of the middle-to-distal ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy, anchoring it to the anterior abdominal wallAbdominal wallThe outer margins of the abdomen, extending from the osteocartilaginous thoracic cage to the pelvis. Though its major part is muscular, the abdominal wall consists of at least seven layers: the skin, subcutaneous fat, deep fascia; abdominal muscles, transversalis fascia, extraperitoneal fat, and the parietal peritoneum.Surgical Anatomy of the Abdomen, and may lead to a fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula, volvulusVolvulusA volvulus is the twisting or axial rotation of a portion of the bowel around its mesentery. The most common site of volvulus in adults is the colon; most frequently the sigmoid volvulus. Patients typically present with symptoms of bowel obstruction such as abdominal pain, distension, vomiting, and constipation/obstipation. Volvulus, small bowel obstructionBowel obstructionAny impairment, arrest, or reversal of the normal flow of intestinal contents toward the anal canal.Ascaris/Ascariasis, and/or necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage.