Knee ligament injuries are commonly seen in young athletes as well as in middle-aged adults. Although the clinical presentation varies for each injured ligament, all of these injuries present with joint instability, painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, and difficulty bearing weight. Diagnosis is based on clinical exam and confirmed with diagnostic imaging or direct visualization (arthroscopy). Management can be conservative or surgical, depending on the severity of the injury.
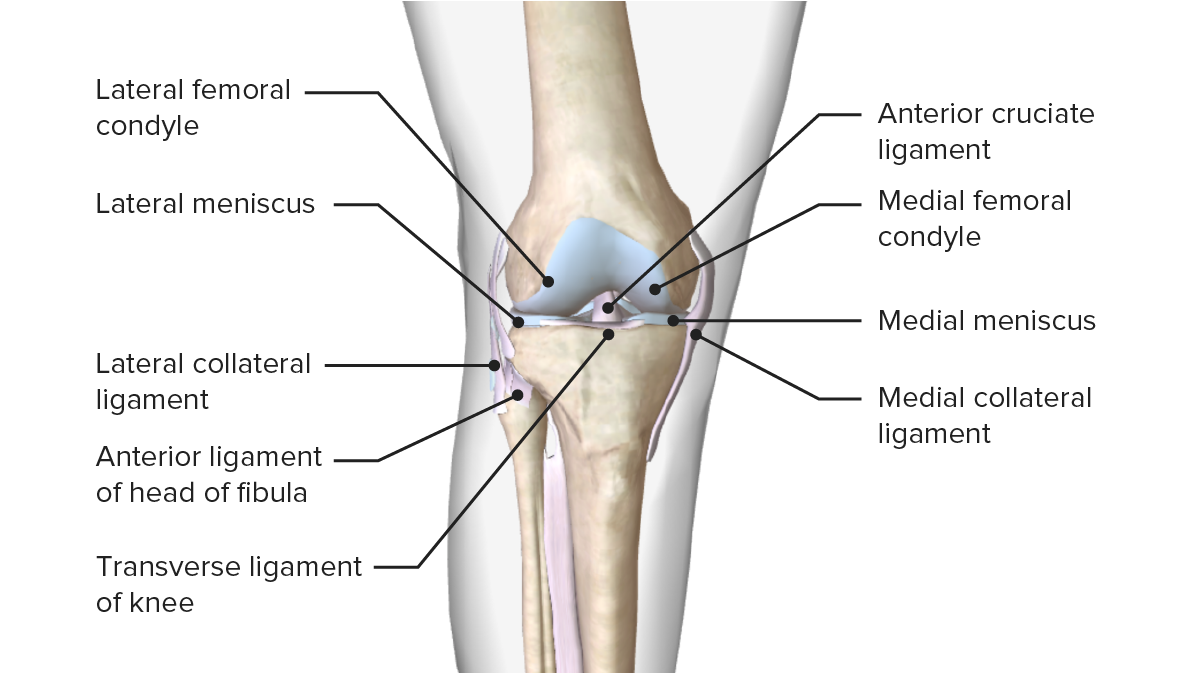
An anterior cruciate ligamentAnterior Cruciate LigamentA strong ligament of the knee that originates from the posteromedial portion of the lateral condyle of the femur, passes anteriorly and inferiorly between the condyles, and attaches to the depression in front of the intercondylar eminence of the tibia.Knee Joint: Anatomy (ACLACLA strong ligament of the knee that originates from the posteromedial portion of the lateral condyle of the femur, passes anteriorly and inferiorly between the condyles, and attaches to the depression in front of the intercondylar eminence of the tibia.Knee Joint: Anatomy) injury causes structural damage to the anterior cruciate ligamentAnterior Cruciate LigamentA strong ligament of the knee that originates from the posteromedial portion of the lateral condyle of the femur, passes anteriorly and inferiorly between the condyles, and attaches to the depression in front of the intercondylar eminence of the tibia.Knee Joint: Anatomy. The functions of the ligament are to:
Control anterior translationTranslationTranslation is the process of synthesizing a protein from a messenger RNA (mRNA) transcript. This process is divided into three primary stages: initiation, elongation, and termination. Translation is catalyzed by structures known as ribosomes, which are large complexes of proteins and ribosomal RNA (rRNA). Stages and Regulation of Translation of the tibiaTibiaThe second longest bone of the skeleton. It is located on the medial side of the lower leg, articulating with the fibula laterally, the talus distally, and the femur proximally.Knee Joint: Anatomy on the femur
Restrict varus/valgus deviation of the tibiaTibiaThe second longest bone of the skeleton. It is located on the medial side of the lower leg, articulating with the fibula laterally, the talus distally, and the femur proximally.Knee Joint: Anatomy on the femur
Anatomy
Originates at the posteromedial aspect of the lateral femoral condyle, posterior to the longitudinal axis of the femur
Runs inferiorly, medially, and anteriorly
Attaches to the anteromedial aspect of the tibiaTibiaThe second longest bone of the skeleton. It is located on the medial side of the lower leg, articulating with the fibula laterally, the talus distally, and the femur proximally.Knee Joint: Anatomy between the condyles
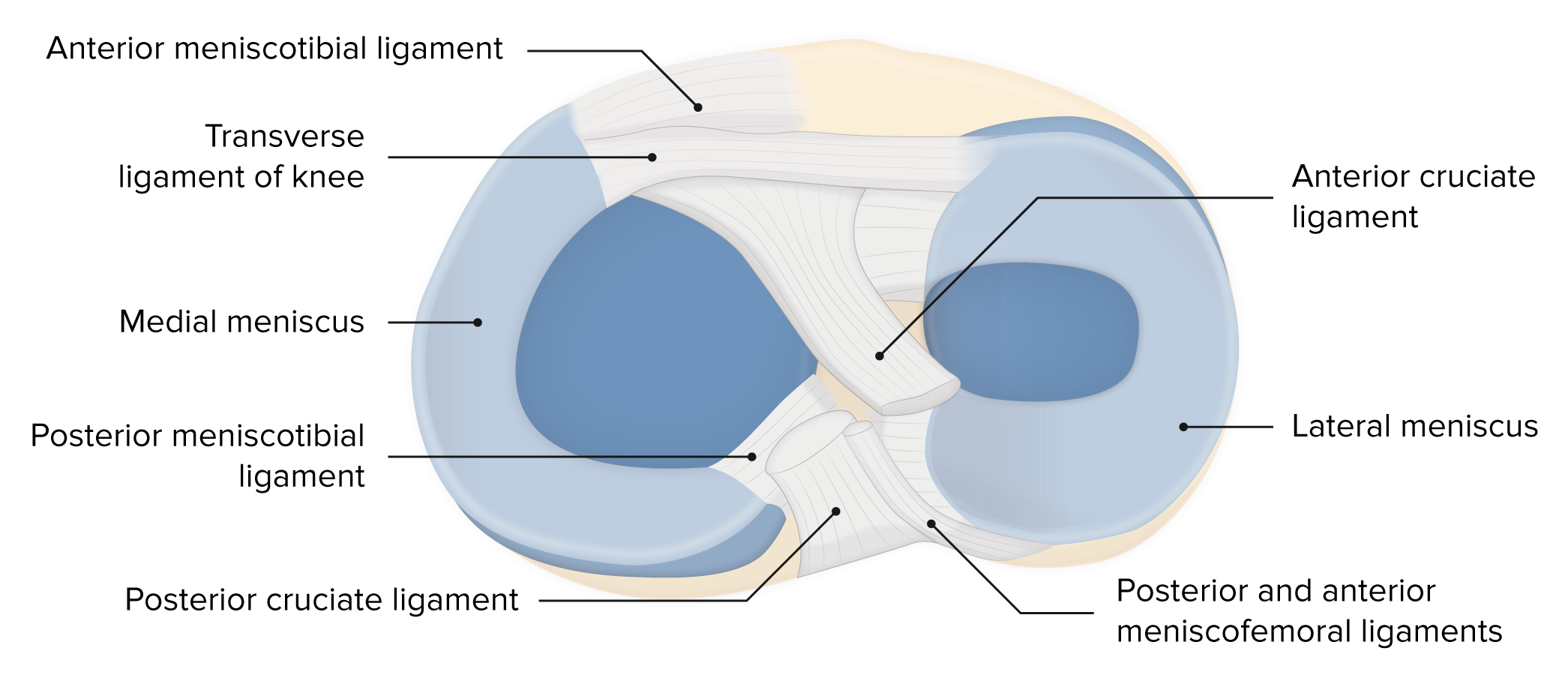
Image displaying the menisci and their relation with other articular surfaces that compose the knee joint
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency: 68.6 per 100,000/year in the United States
Peak incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency in men: between 19 and 25 years; related to sports
Peak incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency in women: 14–18 years
Most commonly injured ligament in the knee
Athletes and trauma patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship are the most commonly affected.
Etiology
Noncontact mechanism (rotational forces):
Skiers
Baseball players
Soccer players
Basketball players
Contact mechanism (direct blunt trauma to the knee): football players
Clinical presentation
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with an ACLACLA strong ligament of the knee that originates from the posteromedial portion of the lateral condyle of the femur, passes anteriorly and inferiorly between the condyles, and attaches to the depression in front of the intercondylar eminence of the tibia.Knee Joint: Anatomy injury present with painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and report recent high-energy blunt trauma to the knee.
History:
Patient reports hearing or feeling a “pop” and that the affected knee “gave out” at the time of injury.
Tenderness to palpationPalpationApplication of fingers with light pressure to the surface of the body to determine consistency of parts beneath in physical diagnosis; includes palpation for determining the outlines of organs.Dermatologic Examination along the joint line
EdemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema around the knee jointKnee jointThe knee joint is made up of the articulations between the femur, tibia, and patella bones, and is one of the largest and most complex joints of the human body. The knee is classified as a synovial hinge joint, which primarily allows for flexion and extension with a more limited degree of translation and rotation. Knee Joint: Anatomy
Decreased range of motionRange of motionThe distance and direction to which a bone joint can be extended. Range of motion is a function of the condition of the joints, muscles, and connective tissues involved. Joint flexibility can be improved through appropriate muscle strength exercises.Examination of the Upper Limbs
Knee instability tests:
Anterior drawer maneuver:
The patient lies supine with hips flexed to 45 degrees, knee at a 90-degree angle, and feet flat on the exam table.
The clinicianClinicianA physician, nurse practitioner, physician assistant, or another health professional who is directly involved in patient care and has a professional relationship with patients.Clinician–Patient Relationship stabilizes the legLegThe lower leg, or just “leg” in anatomical terms, is the part of the lower limb between the knee and the ankle joint. The bony structure is composed of the tibia and fibula bones, and the muscles of the leg are grouped into the anterior, lateral, and posterior compartments by extensions of fascia.Leg: Anatomy by sitting on the patient’s toes and holds the proximal tibiaTibiaThe second longest bone of the skeleton. It is located on the medial side of the lower leg, articulating with the fibula laterally, the talus distally, and the femur proximally.Knee Joint: Anatomy with both hands and pulls anteriorly.
Positive test: Proximal tibiaTibiaThe second longest bone of the skeleton. It is located on the medial side of the lower leg, articulating with the fibula laterally, the talus distally, and the femur proximally.Knee Joint: Anatomy will slide anteriorly, like a drawer being opened.
The patient lies supine with the knee fully extended.
The clinicianClinicianA physician, nurse practitioner, physician assistant, or another health professional who is directly involved in patient care and has a professional relationship with patients.Clinician–Patient Relationship places an internal rotationInternal RotationExamination of the Upper Limbs and valgus force on the proximal tibiaTibiaThe second longest bone of the skeleton. It is located on the medial side of the lower leg, articulating with the fibula laterally, the talus distally, and the femur proximally.Knee Joint: Anatomy while carrying the knee into passive flexionFlexionExamination of the Upper Limbs.
The test is positive if the knee becomes unstable and subluxated; even a “clunk” sound could be produced.
Lachman test:
The patient lies supine with the affected knee at a 30-degree angle.
The clinicianClinicianA physician, nurse practitioner, physician assistant, or another health professional who is directly involved in patient care and has a professional relationship with patients.Clinician–Patient Relationship stabilizes the distal femur with the left handHandThe hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. It consists of 5 metacarpal bones and 14 phalanges, as well as numerous muscles innervated by the median and ulnar nerves. Hand: Anatomy and pulls on the tibiaTibiaThe second longest bone of the skeleton. It is located on the medial side of the lower leg, articulating with the fibula laterally, the talus distally, and the femur proximally.Knee Joint: Anatomy toward themselves.
Positive test: anterior displacementDisplacementThe process by which an emotional or behavioral response that is appropriate for one situation appears in another situation for which it is inappropriate.Defense Mechanisms
Anterior drawer test
Image: “Anterior Drawer test” by Rossi R, Dettoni F, Bruzzone M, Cottino U, D’Elicio DG, Bonasia DE. License: CC BY 2.0
Pivot shift test
Image: “Pivot Shift (Jerk) Test” by Rossi R, Dettoni F, Bruzzone M, Cottino U, D’Elicio DG, Bonasia DE. License: CC BY 2.0
Lachman test
Image: “Lachman Test” by Rossi R, Dettoni F, Bruzzone M, Cottino U, D’Elicio DG, Bonasia DE. License: CC BY 2.0
Diagnosis
Diagnosis is made clinically and confirmed by imaging.
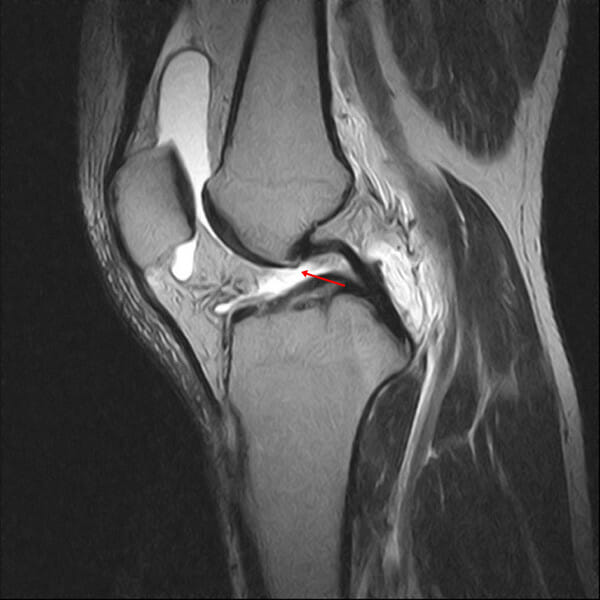
MRI is the preferred imaging method:
Primary signs:
Hyperintensity of the ACLACLA strong ligament of the knee that originates from the posteromedial portion of the lateral condyle of the femur, passes anteriorly and inferiorly between the condyles, and attaches to the depression in front of the intercondylar eminence of the tibia.Knee Joint: Anatomy (usually at the midportion)
Discontinuity of ligament fibers
Alteration of Blumensaat’s line
EdemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema
Secondary signs:
Bone marrowBone marrowThe soft tissue filling the cavities of bones. Bone marrow exists in two types, yellow and red. Yellow marrow is found in the large cavities of large bones and consists mostly of fat cells and a few primitive blood cells. Red marrow is a hematopoietic tissue and is the site of production of erythrocytes and granular leukocytes. Bone marrow is made up of a framework of connective tissue containing branching fibers with the frame being filled with marrow cells.Bone Marrow: Composition and HematopoiesisedemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema
Anterior tibial translationTranslationTranslation is the process of synthesizing a protein from a messenger RNA (mRNA) transcript. This process is divided into three primary stages: initiation, elongation, and termination. Translation is catalyzed by structures known as ribosomes, which are large complexes of proteins and ribosomal RNA (rRNA). Stages and Regulation of Translation > 7 mm
X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests is useful only to rule out fractures.
Arthroscopy: uses an instrument (arthroscope) inserted into the joint through a small incision
Gold standard for diagnosis
Minimally invasive surgical procedure used for diagnosis; may also be used for the treatment of meniscal tears
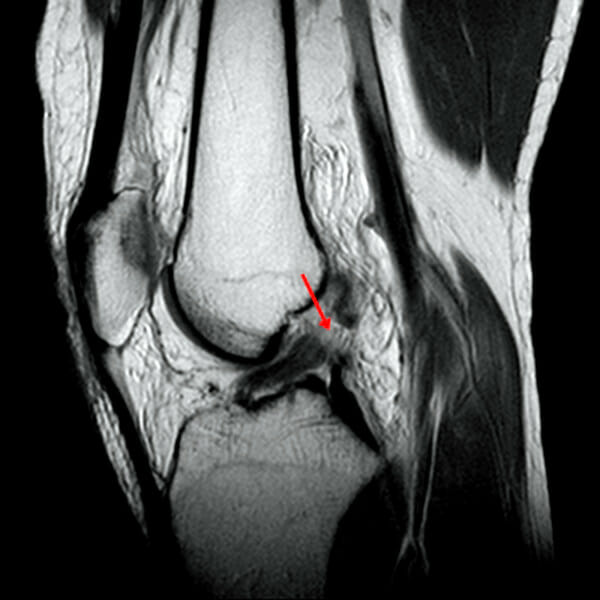
In the proton-density sagittal image, the anterior cruciate ligament (ACL) is not seen in the notch of the knee (arrow). Nonvisualization is defined as a failure to visualize the ACL on the image.
Image: “In this proton density sagittal image” by Chang et al. License: CC BY 2.0
T2-weighted, fat-suppressed sagittal image showing discontinuity of anterior cruciate ligament (ACL) fibers (arrow): Discontinuity is defined as a focal gap or interruption of ACL fibers.
Image: “In this T2-weighted fat-suppressed sagittal image” by Chang et al. License: CC BY 2.0
T2-weighted, fat-suppressed sagittal image showing abnormal signal intensity as increased signal intensity within the anterior cruciate ligament (arrow)
Image: “In this T2-weighted fat-suppressed sagittal image” by Chang et al. License: CC BY 2.0
T2-weighted, fat-suppressed sagittal image showing bone contusions in the lateral femoral condyle and posterolateral tibial plateau
Image: “Sagittal fat-suppressed T2-weighted image” by Chang et al. License: CC BY 2.0
Management
Conservative management: in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with low functional demand
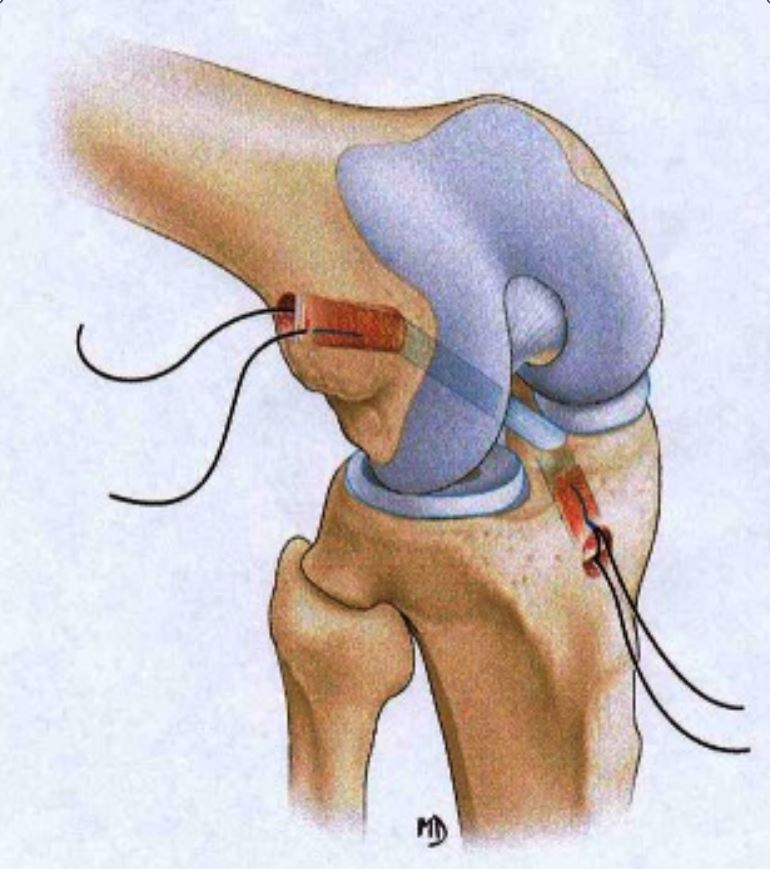
Orthopedic surgery consultation and surgical management for reconstruction using a tissue graftGraftA piece of living tissue that is surgically transplantedOrgan Transplantation is done in:
Athletes
Young, active patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas: 90% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship will return to normal functioning after repair.
Meniscal tear: injury to the meniscus caused by rotational or shearing forcesShearing forcesVascular Resistance, Flow, and Mean Arterial Pressure across the tibiofemoral jointTibiofemoral jointKnee Joint: Anatomy. Clinical presentation includes a history of a twisting or rotational injury followed by joint line painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways associated with a small effusion. Some patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may also present with mechanical symptoms, such as joint locking, clicking, or catching.
Posterior knee dislocationPosterior Knee DislocationKnee Dislocation: pathologic loss of articulation of the knee jointKnee jointThe knee joint is made up of the articulations between the femur, tibia, and patella bones, and is one of the largest and most complex joints of the human body. The knee is classified as a synovial hinge joint, which primarily allows for flexion and extension with a more limited degree of translation and rotation. Knee Joint: Anatomy due to high-energy trauma such as that due to motor-vehicle collisions or low-energy traumaLow-Energy TraumaToddler’s Fractures such as that seen in athletic training.
FractureFractureA fracture is a disruption of the cortex of any bone and periosteum and is commonly due to mechanical stress after an injury or accident. Open fractures due to trauma can be a medical emergency. Fractures are frequently associated with automobile accidents, workplace injuries, and trauma.Overview of Bone Fractures of the tibial spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: Anatomy or femoral or tibial epiphysisTibial EpiphysisBlount’s Disease: diagnosed on X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests and managed by an orthopedic specialist.
Medial collateral knee ligament injury: structural damage to the medial collateral ligamentMedial collateral ligamentKnee Joint: Anatomy (function is to provide valgus stability to the knee)
Unhappy triad: simultaneous injury of the MCLMCLKnee Joint: Anatomy, ACLACLA strong ligament of the knee that originates from the posteromedial portion of the lateral condyle of the femur, passes anteriorly and inferiorly between the condyles, and attaches to the depression in front of the intercondylar eminence of the tibia.Knee Joint: Anatomy, and the medial meniscusMedial MeniscusMeniscus Tear
Anatomy
Originates from the medial epicondyleMedial epicondyleArm: Anatomy of the femur and runs to the medial condyle of the tibiaTibiaThe second longest bone of the skeleton. It is located on the medial side of the lower leg, articulating with the fibula laterally, the talus distally, and the femur proximally.Knee Joint: Anatomy
Attaches in 2 places on the tibiaTibiaThe second longest bone of the skeleton. It is located on the medial side of the lower leg, articulating with the fibula laterally, the talus distally, and the femur proximally.Knee Joint: Anatomy
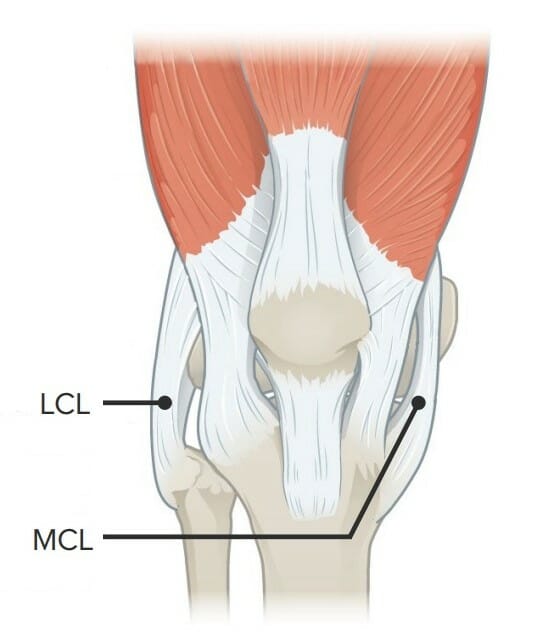
Image showcasing the lateral collateral ligament (LCL) and the medial collateral ligament (MCL)
Sudden, high-energy twisting or turning motions (rotational forces):
Skiers
Baseball players
Soccer players
Basketball players
Blunt trauma (direct blow to the lateral aspect of the knee)
Clinical presentation
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with MCLMCLKnee Joint: Anatomy injury present with painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and report recent trauma to the knee. The exam is ideally done in the 1st 20–30 minutes, before swellingSwellingInflammation interferes with the exam.
History:
Patient reports hearing or feeling a pop and that the affected knee feels unstable.
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways on palpationPalpationApplication of fingers with light pressure to the surface of the body to determine consistency of parts beneath in physical diagnosis; includes palpation for determining the outlines of organs.Dermatologic Examination along the course of the MCLMCLKnee Joint: Anatomy
EdemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema/ecchymosisEcchymosisExtravasation of blood into the skin, resulting in a nonelevated, rounded or irregular, blue or purplish patch, larger than a petechia.Orbital Fractures on the medial aspect of the knee
Decreased range of motionRange of motionThe distance and direction to which a bone joint can be extended. Range of motion is a function of the condition of the joints, muscles, and connective tissues involved. Joint flexibility can be improved through appropriate muscle strength exercises.Examination of the Upper Limbs
Knee instability test (valgus stress test):
The patient lies supine with the affected limb abducted off the examination table and the knee fully extended.
The clinicianClinicianA physician, nurse practitioner, physician assistant, or another health professional who is directly involved in patient care and has a professional relationship with patients.Clinician–Patient Relationship holds the ipsilateral ankle with 1 handHandThe hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. It consists of 5 metacarpal bones and 14 phalanges, as well as numerous muscles innervated by the median and ulnar nerves. Hand: Anatomy and applies valgus pressure on the knee.
The test is positive if joint opening and painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways are detected.
Grade I: painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways along the course of the MCLMCLKnee Joint: Anatomy with no joint opening
Grade II: partial opening of the joint
Grade III: significant joint opening
Valgus and varus stress tests
Image: “Valgus and varus stress tests” by Rossi R, Dettoni F, Bruzzone M, Cottino U, D’Elicio DG, Bonasia DE. License: CC BY 2.0
Diagnosis
Diagnosis is made clinically and later confirmed by imaging studies.
MRI is the preferred imaging method: allows for examination of neighboring structures
Ultrasonography may be a more accessible alternative to MRI.
X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests is useful only to rule out fractures.
Magnetic resonance imaging showing medial collateral ligament injury and displacement of the lateral meniscus
Image: “MRI showing medial collateral ligament injury and displacement of the lateral meniscus” by Matthijs R. Douma et al. License: CC BY 4.0
Management
Conservative management: in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with low functional demand
Return-to-play protocol: progressive increase in the difficulty of exercises
Program must be as comprehensive as possible to ensure maximal recovery of functionality.
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas: 98% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with grade I and II injuries will experience a full recovery with conservative management.
Grade I injuries: typically can return to athletic activity in 10–14 days
Grade II and III injuries: variableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables recovery times
Slipped capital femoral epiphysisEpiphysisThe head of a long bone that is separated from the shaft by the epiphyseal plate until bone growth stops. At that time, the plate disappears and the head and shaft are united.Bones: Structure and Types: orthopedic disorder of early adolescence characterized by the pathologic “slipping,” or displacementDisplacementThe process by which an emotional or behavioral response that is appropriate for one situation appears in another situation for which it is inappropriate.Defense Mechanisms, of the femoral head, or epiphysisEpiphysisThe head of a long bone that is separated from the shaft by the epiphyseal plate until bone growth stops. At that time, the plate disappears and the head and shaft are united.Bones: Structure and Types, on the femoral neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess. Slipped capital femoral epiphysisEpiphysisThe head of a long bone that is separated from the shaft by the epiphyseal plate until bone growth stops. At that time, the plate disappears and the head and shaft are united.Bones: Structure and Types is considered a type I Salter-Harris growth plate fractureGrowth Plate FractureSlipped Capital Femoral Epiphysis, and it affects boys twice as often as girls.
OsteoarthritisOsteoarthritisOsteoarthritis (OA) is the most common form of arthritis, and is due to cartilage destruction and changes of the subchondral bone. The risk of developing this disorder increases with age, obesity, and repetitive joint use or trauma. Patients develop gradual joint pain, stiffness lasting < 30 minutes, and decreased range of motion. Osteoarthritis: most common form of arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis due to cartilageCartilageCartilage is a type of connective tissue derived from embryonic mesenchyme that is responsible for structural support, resilience, and the smoothness of physical actions. Perichondrium (connective tissue membrane surrounding cartilage) compensates for the absence of vasculature in cartilage by providing nutrition and support. Cartilage: Histology destruction and changes of the subchondral boneSubchondral BoneOsteochondritis Dissecans. The risk of developing osteoarthritisOsteoarthritisOsteoarthritis (OA) is the most common form of arthritis, and is due to cartilage destruction and changes of the subchondral bone. The risk of developing this disorder increases with age, obesity, and repetitive joint use or trauma. Patients develop gradual joint pain, stiffness lasting < 30 minutes, and decreased range of motion. Osteoarthritis increases with age, obesityObesityObesity is a condition associated with excess body weight, specifically with the deposition of excessive adipose tissue. Obesity is considered a global epidemic. Major influences come from the western diet and sedentary lifestyles, but the exact mechanisms likely include a mixture of genetic and environmental factors. Obesity, and repetitive joint use or trauma. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship develop gradual joint painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, stiffness lasting < 30 minutes, and decreased range of motionRange of motionThe distance and direction to which a bone joint can be extended. Range of motion is a function of the condition of the joints, muscles, and connective tissues involved. Joint flexibility can be improved through appropriate muscle strength exercises.Examination of the Upper Limbs.
Image displaying the menisci and their relation with other articular surfaces that compose the knee joint
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways on palpationPalpationApplication of fingers with light pressure to the surface of the body to determine consistency of parts beneath in physical diagnosis; includes palpation for determining the outlines of organs.Dermatologic Examination along the joint line
EdemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema around the knee jointKnee jointThe knee joint is made up of the articulations between the femur, tibia, and patella bones, and is one of the largest and most complex joints of the human body. The knee is classified as a synovial hinge joint, which primarily allows for flexion and extension with a more limited degree of translation and rotation. Knee Joint: Anatomy
Decreased range of motionRange of motionThe distance and direction to which a bone joint can be extended. Range of motion is a function of the condition of the joints, muscles, and connective tissues involved. Joint flexibility can be improved through appropriate muscle strength exercises.Examination of the Upper Limbs
Knee instability tests:
Varus stress test:
The patient lies supine with the affected knee at a 30-degree angle.
The clinicianClinicianA physician, nurse practitioner, physician assistant, or another health professional who is directly involved in patient care and has a professional relationship with patients.Clinician–Patient Relationship stabilizes the distal femur with 1 handHandThe hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. It consists of 5 metacarpal bones and 14 phalanges, as well as numerous muscles innervated by the median and ulnar nerves. Hand: Anatomy and applies varus pressure on the ankle.
The test is positive if there is lateral compartment gaping.
The patient lies supine with the affected knee extended.
The clinicianClinicianA physician, nurse practitioner, physician assistant, or another health professional who is directly involved in patient care and has a professional relationship with patients.Clinician–Patient Relationship stabilizes the distal femur with 1 handHandThe hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. It consists of 5 metacarpal bones and 14 phalanges, as well as numerous muscles innervated by the median and ulnar nerves. Hand: Anatomy and externally rotates the tibiaTibiaThe second longest bone of the skeleton. It is located on the medial side of the lower leg, articulating with the fibula laterally, the talus distally, and the femur proximally.Knee Joint: Anatomy.
Positive test: hyperextension of the knee
Grades of instability in LCL injuries:
Grade I:
Clinical signs of sprain (painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways)
No instability
Grade II:
More signs of sprain (painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema)
Ligament laxity is observed, but with an end point.
Grade III:
Severe clinical signs of sprain (painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema, ecchymosisEcchymosisExtravasation of blood into the skin, resulting in a nonelevated, rounded or irregular, blue or purplish patch, larger than a petechia.Orbital Fractures)
Noticeable knee instability
External rotation recurvatum test
Image: “External Rotation Recurvatum Test” by Rossi R, Dettoni F, Bruzzone M, Cottino U, D’Elicio DG, Bonasia DE. License: CC BY 2.0
Diagnosis
Diagnosis is made clinically and confirmed by imaging studies.
X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests is useful only to rule out fractures.
MRI indicated if:
History of significant trauma
Ultrasound findings suggest major injury to the LCL and other structures:
Cruciate ligament
Meniscal tear
Segond fracture in a 16-year-old (circled area):
The anterior cruciate ligament (ACL) and medial meniscus were torn during an athletic event.
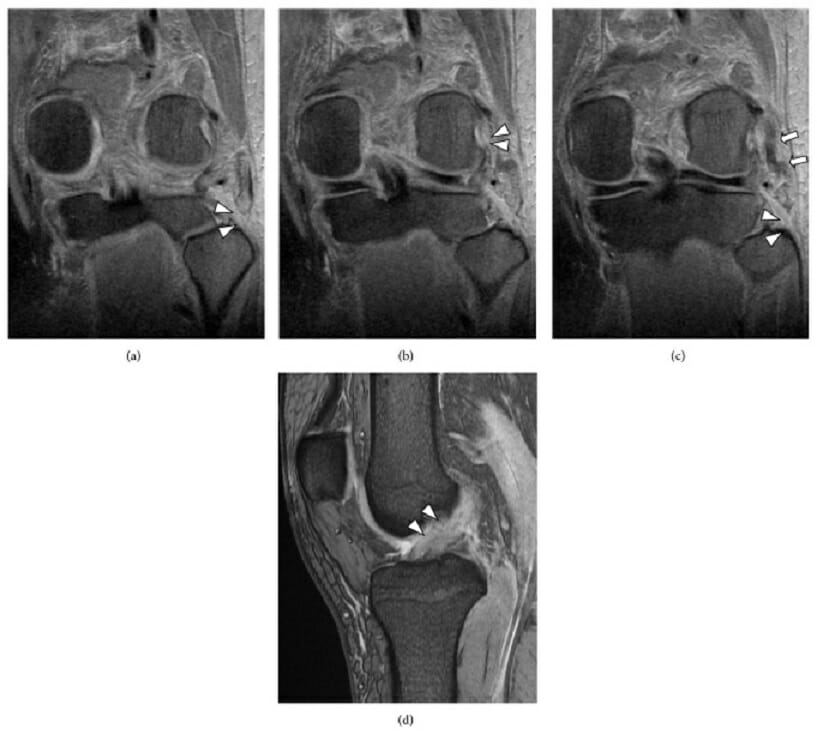
A multiple-ligament knee injury that includes posterolateral corner disruption: (a) A T2-weighted, coronal MRI shows absence of the biceps femoris tendon (arrowhead).
(b) A T2-weighted, coronal MRI shows popliteus muscle-tendon rupture at the femoral attachment (arrowhead).
(c) A T2-weighted, coronal MRI shows lateral collateral ligament (LCL) rupture at the fibula head (arrowhead) and substance of the LCL (arrow).
(d) A T2-weighted, sagittal MRI shows anterior cruciate ligament (ACL) rupture (arrowhead).
Image: “(a) Magnetic resonance imaging” by Takeshi Oshima et al. License: CC BY 3.0
Management
Conservative management for grade I and II injuries:
Orthopedic surgery consultation and surgical management:
Consultation in all cases to discuss treatment options
Surgery is indicated in grade III injuries.
Caution to avoid injury to the common peroneal nervePeroneal nerveThe lateral of the two terminal branches of the sciatic nerve. The peroneal (or fibular) nerve provides motor and sensory innervation to parts of the leg and foot.Popliteal Fossa: Anatomy and neurologic complications
Joint instability and painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways must be resolved and range of motionRange of motionThe distance and direction to which a bone joint can be extended. Range of motion is a function of the condition of the joints, muscles, and connective tissues involved. Joint flexibility can be improved through appropriate muscle strength exercises.Examination of the Upper Limbs restored.
Grade I: return to activity after 4 weeks
Grade II: return to activity after 10 weeks
Grade III injuries: immobilizationImmobilizationDelirium and non–weight-bearing for 6 weeks postoperatively
Rehabilitation starts 4 months after reconstruction.
Criteria for return to full activity:
Fully restored range of motionRange of motionThe distance and direction to which a bone joint can be extended. Range of motion is a function of the condition of the joints, muscles, and connective tissues involved. Joint flexibility can be improved through appropriate muscle strength exercises.Examination of the Upper Limbs
Recovered quadriceps and hamstring strength
Resolution of joint painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Resolution of joint laxity and instability
Able to complete normal physical activities without painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Complications:
Chronic knee painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas: The majority of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship return to normal functioning after treatment.
Differential diagnosis of LCL tear
Posterior knee dislocationPosterior Knee DislocationKnee Dislocation: pathologic loss of articulation of the knee jointKnee jointThe knee joint is made up of the articulations between the femur, tibia, and patella bones, and is one of the largest and most complex joints of the human body. The knee is classified as a synovial hinge joint, which primarily allows for flexion and extension with a more limited degree of translation and rotation. Knee Joint: Anatomy due to high-energy trauma such as that due to motor-vehicle collisions or low-energy traumaLow-Energy TraumaToddler’s Fractures such as that seen in athletic training.
Meniscal tear: injury to the meniscus caused by rotational or shearing forcesShearing forcesVascular Resistance, Flow, and Mean Arterial Pressure across the tibiofemoral jointTibiofemoral jointKnee Joint: Anatomy. Clinical presentation includes a history of a twisting or rotational injury followed by joint line painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways associated with a small effusion. Some patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may also present with mechanical symptoms, such as joint locking, clicking, or catching.
ACLACLA strong ligament of the knee that originates from the posteromedial portion of the lateral condyle of the femur, passes anteriorly and inferiorly between the condyles, and attaches to the depression in front of the intercondylar eminence of the tibia.Knee Joint: Anatomy injury: causes structural damage to the ligament whose functions are to control anterior translationTranslationTranslation is the process of synthesizing a protein from a messenger RNA (mRNA) transcript. This process is divided into three primary stages: initiation, elongation, and termination. Translation is catalyzed by structures known as ribosomes, which are large complexes of proteins and ribosomal RNA (rRNA). Stages and Regulation of Translation of the tibiaTibiaThe second longest bone of the skeleton. It is located on the medial side of the lower leg, articulating with the fibula laterally, the talus distally, and the femur proximally.Knee Joint: Anatomy and restrain tibial rotationRotationMotion of an object in which either one or more points on a line are fixed. It is also the motion of a particle about a fixed point.X-rays and varus/valgus stress.
Posterior Cruciate Ligament (PCL) Injury
Definition
The posterior cruciate ligamentPosterior Cruciate LigamentA strong ligament of the knee that originates from the anterolateral surface of the medial condyle of the femur, passes posteriorly and inferiorly between the condyles, and attaches to the posterior intercondylar area of the tibia.Knee Joint: Anatomy (PCLPCLA strong ligament of the knee that originates from the anterolateral surface of the medial condyle of the femur, passes posteriorly and inferiorly between the condyles, and attaches to the posterior intercondylar area of the tibia.Knee Joint: Anatomy) is the largest and strongest ligament in the knee. Injury to the PCLPCLA strong ligament of the knee that originates from the anterolateral surface of the medial condyle of the femur, passes posteriorly and inferiorly between the condyles, and attaches to the posterior intercondylar area of the tibia.Knee Joint: Anatomy causes structural damage resulting in loss of stabilization with resultant posterior translationTranslationTranslation is the process of synthesizing a protein from a messenger RNA (mRNA) transcript. This process is divided into three primary stages: initiation, elongation, and termination. Translation is catalyzed by structures known as ribosomes, which are large complexes of proteins and ribosomal RNA (rRNA). Stages and Regulation of Translation of the tibiaTibiaThe second longest bone of the skeleton. It is located on the medial side of the lower leg, articulating with the fibula laterally, the talus distally, and the femur proximally.Knee Joint: Anatomy.
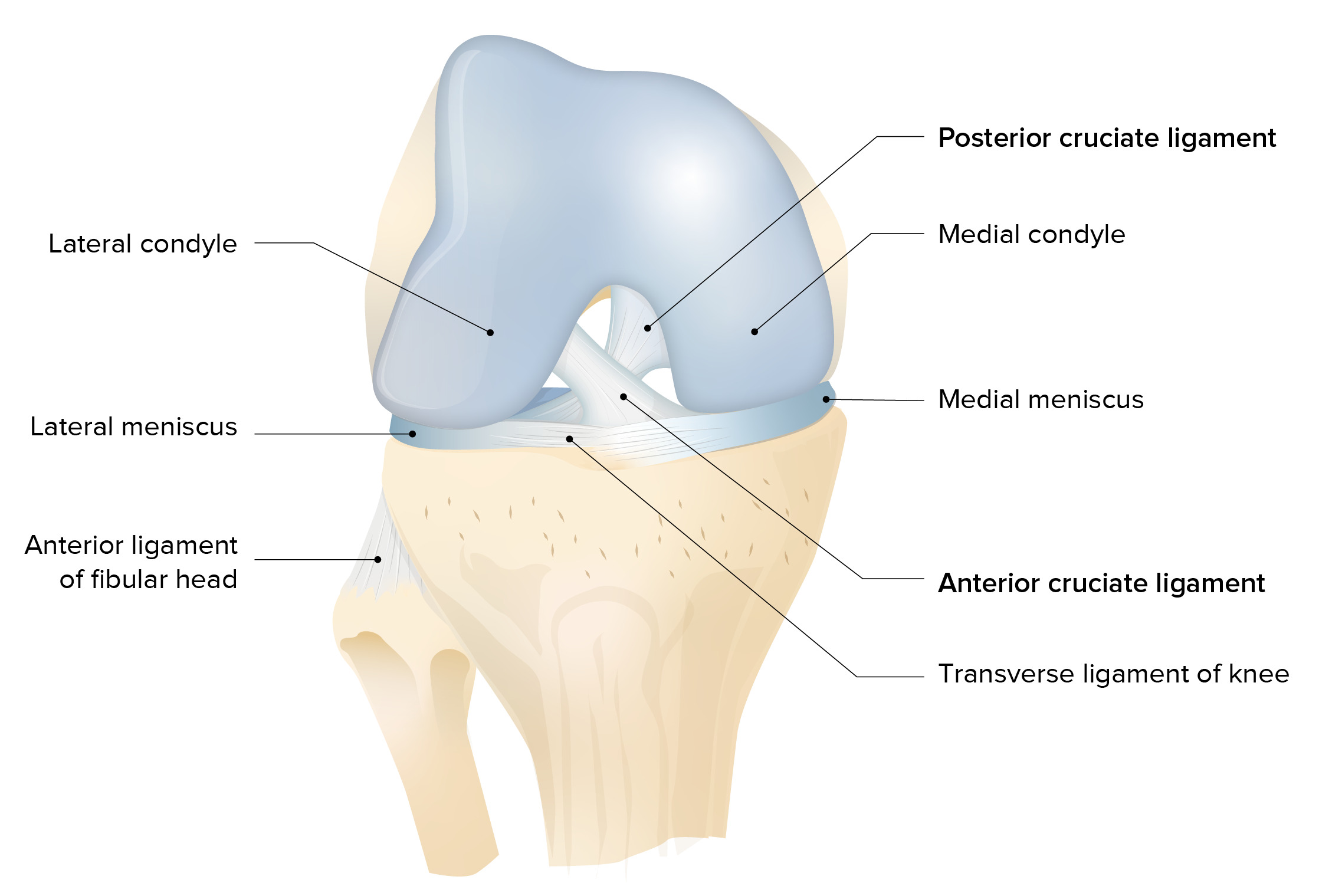
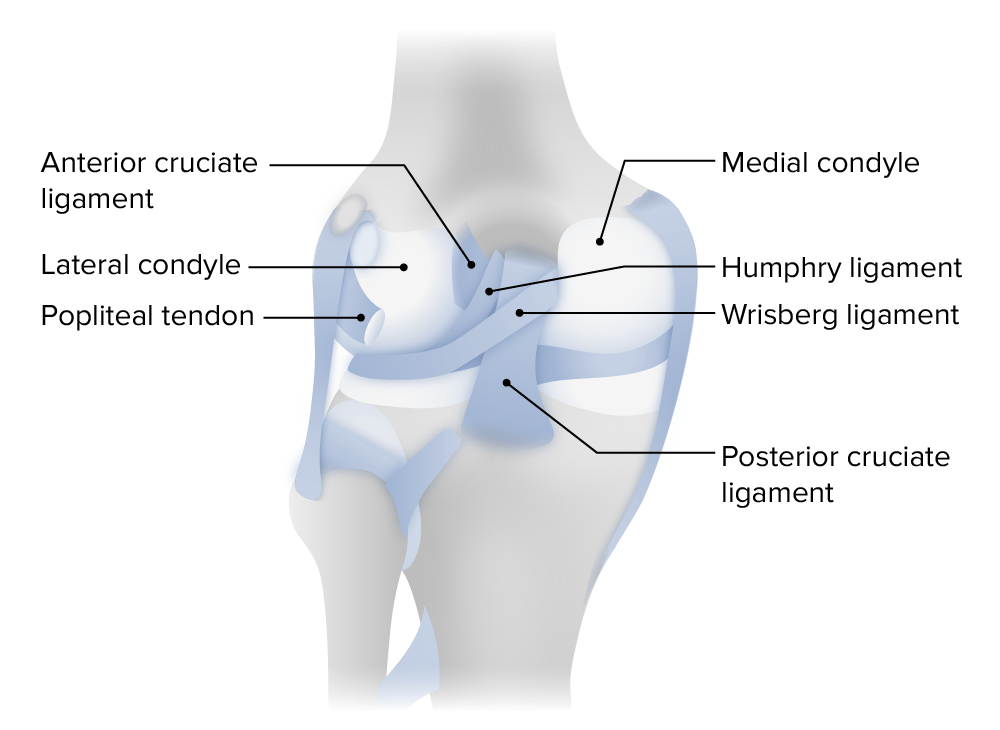
Posterior view of the left knee joint
Image by Lecturio.
Epidemiology
Seen in approximately 3% of knee injuries due to trauma
95% of PCLPCLA strong ligament of the knee that originates from the anterolateral surface of the medial condyle of the femur, passes posteriorly and inferiorly between the condyles, and attaches to the posterior intercondylar area of the tibia.Knee Joint: Anatomy tears occur in combination with other ligament tears; isolated PCLPCLA strong ligament of the knee that originates from the anterolateral surface of the medial condyle of the femur, passes posteriorly and inferiorly between the condyles, and attaches to the posterior intercondylar area of the tibia.Knee Joint: Anatomy injuries are uncommon.
Etiology
High-energy trauma such as motor-vehicle accidents, in association with damage to other knee structures
Sports injuries: 2nd most common cause of PCLPCLA strong ligament of the knee that originates from the anterolateral surface of the medial condyle of the femur, passes posteriorly and inferiorly between the condyles, and attaches to the posterior intercondylar area of the tibia.Knee Joint: Anatomy injury
Clinical presentation
Isolated PCLPCLA strong ligament of the knee that originates from the anterolateral surface of the medial condyle of the femur, passes posteriorly and inferiorly between the condyles, and attaches to the posterior intercondylar area of the tibia.Knee Joint: Anatomy injuries are relatively uncommon, and athletes with such injuries may continue to function at a high level.
History:
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways in the back of the knee (especially with squatting or kneeling)
Slight limp
Chronically injured PCL-deficient knee may present with generalized anterior knee painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways localized to the medial compartment or patellofemoral jointPatellofemoral JointThe articulation between the articular surface of the patella and the patellar surface of the femur.Knee Joint: Anatomy.
The patient lies supine with the affected knee at a 90-degree angle.
The clinicianClinicianA physician, nurse practitioner, physician assistant, or another health professional who is directly involved in patient care and has a professional relationship with patients.Clinician–Patient Relationship stabilizes the legLegThe lower leg, or just “leg” in anatomical terms, is the part of the lower limb between the knee and the ankle joint. The bony structure is composed of the tibia and fibula bones, and the muscles of the leg are grouped into the anterior, lateral, and posterior compartments by extensions of fascia.Leg: Anatomy by sitting on the patient’s toes and grasps the proximal lower legLegThe lower leg, or just “leg” in anatomical terms, is the part of the lower limb between the knee and the ankle joint. The bony structure is composed of the tibia and fibula bones, and the muscles of the leg are grouped into the anterior, lateral, and posterior compartments by extensions of fascia.Leg: Anatomy at the upper tibiaTibiaThe second longest bone of the skeleton. It is located on the medial side of the lower leg, articulating with the fibula laterally, the talus distally, and the femur proximally.Knee Joint: Anatomy and tries to displace the lower legLegThe lower leg, or just “leg” in anatomical terms, is the part of the lower limb between the knee and the ankle joint. The bony structure is composed of the tibia and fibula bones, and the muscles of the leg are grouped into the anterior, lateral, and posterior compartments by extensions of fascia.Leg: Anatomy posteriorly.
Positive test: excessive posterior translationTranslationTranslation is the process of synthesizing a protein from a messenger RNA (mRNA) transcript. This process is divided into three primary stages: initiation, elongation, and termination. Translation is catalyzed by structures known as ribosomes, which are large complexes of proteins and ribosomal RNA (rRNA). Stages and Regulation of Translation
Muller’s test, also called the quadriceps active test:
The patient lies supine as above and is asked to raise the footFootThe foot is the terminal portion of the lower limb, whose primary function is to bear weight and facilitate locomotion. The foot comprises 26 bones, including the tarsal bones, metatarsal bones, and phalanges. The bones of the foot form longitudinal and transverse arches and are supported by various muscles, ligaments, and tendons.Foot: Anatomy off the table.
Positive test: anterior translationTranslationTranslation is the process of synthesizing a protein from a messenger RNA (mRNA) transcript. This process is divided into three primary stages: initiation, elongation, and termination. Translation is catalyzed by structures known as ribosomes, which are large complexes of proteins and ribosomal RNA (rRNA). Stages and Regulation of Translation of the proximal tibiaTibiaThe second longest bone of the skeleton. It is located on the medial side of the lower leg, articulating with the fibula laterally, the talus distally, and the femur proximally.Knee Joint: Anatomy prior to the footFootThe foot is the terminal portion of the lower limb, whose primary function is to bear weight and facilitate locomotion. The foot comprises 26 bones, including the tarsal bones, metatarsal bones, and phalanges. The bones of the foot form longitudinal and transverse arches and are supported by various muscles, ligaments, and tendons.Foot: Anatomy leaving the table while attempting to elevate the footFootThe foot is the terminal portion of the lower limb, whose primary function is to bear weight and facilitate locomotion. The foot comprises 26 bones, including the tarsal bones, metatarsal bones, and phalanges. The bones of the foot form longitudinal and transverse arches and are supported by various muscles, ligaments, and tendons.Foot: Anatomy
Muller’s test, also called the quadriceps active test
Image: “Quadriceps Active Test” by Rossi R, Dettoni F, Bruzzone M, Cottino U, D’Elicio DG, Bonasia DE. License: CC BY 2.0
Diagnosis
X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests to rule out fractures
MRI for suspected PCLPCLA strong ligament of the knee that originates from the anterolateral surface of the medial condyle of the femur, passes posteriorly and inferiorly between the condyles, and attaches to the posterior intercondylar area of the tibia.Knee Joint: Anatomy injury
Management
Referral to orthopedic surgeon is needed.
Grade III PCLPCLA strong ligament of the knee that originates from the anterolateral surface of the medial condyle of the femur, passes posteriorly and inferiorly between the condyles, and attaches to the posterior intercondylar area of the tibia.Knee Joint: Anatomy injuries: demonstrated by the anterior border of the medial tibial plateauPlateauCardiac Physiology being displaced posteriorly > 10 mm
PCLPCLA strong ligament of the knee that originates from the anterolateral surface of the medial condyle of the femur, passes posteriorly and inferiorly between the condyles, and attaches to the posterior intercondylar area of the tibia.Knee Joint: Anatomy disruption involving avulsion fractureAvulsion fractureTearing away of the cortical bone fragment at the location of a strong ligament or tendon attachment. The bone fragment detachment site often occurs near a soft site (e.g., growth plate) at the base where ligaments; tendons; or joint capsules attach.Overview of Bone Fractures at the ligamentous insertion at the tibiaTibiaThe second longest bone of the skeleton. It is located on the medial side of the lower leg, articulating with the fibula laterally, the talus distally, and the femur proximally.Knee Joint: Anatomy
Isolated PCLPCLA strong ligament of the knee that originates from the anterolateral surface of the medial condyle of the femur, passes posteriorly and inferiorly between the condyles, and attaches to the posterior intercondylar area of the tibia.Knee Joint: Anatomy injuries, as multiligament trauma typically requires surgical intervention.
Posterior collateral ligament injury: Other injuries are often sustained in combination with PCLPCLA strong ligament of the knee that originates from the anterolateral surface of the medial condyle of the femur, passes posteriorly and inferiorly between the condyles, and attaches to the posterior intercondylar area of the tibia.Knee Joint: Anatomy injury.
Proximal tibial fractureFractureA fracture is a disruption of the cortex of any bone and periosteum and is commonly due to mechanical stress after an injury or accident. Open fractures due to trauma can be a medical emergency. Fractures are frequently associated with automobile accidents, workplace injuries, and trauma.Overview of Bone Fractures: may result from similar injuries causing a PCL tearPCL tearKnee Pain. A tibial fractureFractureA fracture is a disruption of the cortex of any bone and periosteum and is commonly due to mechanical stress after an injury or accident. Open fractures due to trauma can be a medical emergency. Fractures are frequently associated with automobile accidents, workplace injuries, and trauma.Overview of Bone Fractures typically presents clinically with a hemarthrosisHemarthrosisBleeding into the joints. It may arise from trauma or spontaneously in patients with hemophilia.Hemophilia, larger than the effusion seen with a PCLPCLA strong ligament of the knee that originates from the anterolateral surface of the medial condyle of the femur, passes posteriorly and inferiorly between the condyles, and attaches to the posterior intercondylar area of the tibia.Knee Joint: Anatomy injury. There is associated painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and guarding that limitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation clinical examination. Diagnosis is made with X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests, and management is by an orthopedic specialist.
Tibiofemoral dislocation: may occur following significant trauma and is a potentially limb-threatening injury if there is circulatory compromise. Tibiofemoral dislocation requires emergency evaluation. Clinical presentation is with severe painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and swellingSwellingInflammation and gross instability of the knee. There may be obvious deformityDeformityExamination of the Upper Limbs, and management is an urgent reduction if the dislocation does not reduce spontaneously.
BoneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types contusion: may occur at the same time as PCLPCLA strong ligament of the knee that originates from the anterolateral surface of the medial condyle of the femur, passes posteriorly and inferiorly between the condyles, and attaches to the posterior intercondylar area of the tibia.Knee Joint: Anatomy injury; however, posterior drawer test would be negative in a patient with an isolated boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types contusion.
Quadriceps tendonQuadriceps tendonKnee Joint: Anatomy and patellar tendon tears: also may occur due to an injury involving falling with the knee flexed. With tendon tears, patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship often report feeling a popping sensation in the knee and are immediately unable to bear weight, whereas patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with a PCLPCLA strong ligament of the knee that originates from the anterolateral surface of the medial condyle of the femur, passes posteriorly and inferiorly between the condyles, and attaches to the posterior intercondylar area of the tibia.Knee Joint: Anatomy injury usually can bear weight. On X-rayX-rayPenetrating electromagnetic radiation emitted when the inner orbital electrons of an atom are excited and release radiant energy. X-ray wavelengths range from 1 pm to 10 nm. Hard x-rays are the higher energy, shorter wavelength x-rays. Soft x-rays or grenz rays are less energetic and longer in wavelength. The short wavelength end of the x-ray spectrum overlaps the gamma rays wavelength range. The distinction between gamma rays and x-rays is based on their radiation source.Pulmonary Function Tests, patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with tendon tears may have altered height of the patellaPatellaThe flat, triangular bone situated at the anterior part of the knee.Knee Joint: Anatomy or signs of a patellar avulsion injury.
References
Jagodzinski, M., Weber-Spickschen, T. S., & Guenther, D. (2020). Dislocations and Soft Tissue Injuries of the Knee. In Browner, B., Jupiter, J., Krettek, C., Anderson, P. (Eds.), Skeletal Trauma: Basic Science, Management, and Reconstruction. pp. 2146–2180. Philadelphia: Elsevier.
Yaras, R. J., O’Neill, N., Yaish, A. M. (2024). Lateral collateral ligament knee injuries. StatPearls. Retrieved on August 6, 2025, from http://www.ncbi.nlm.nih.gov/books/NBK560847/