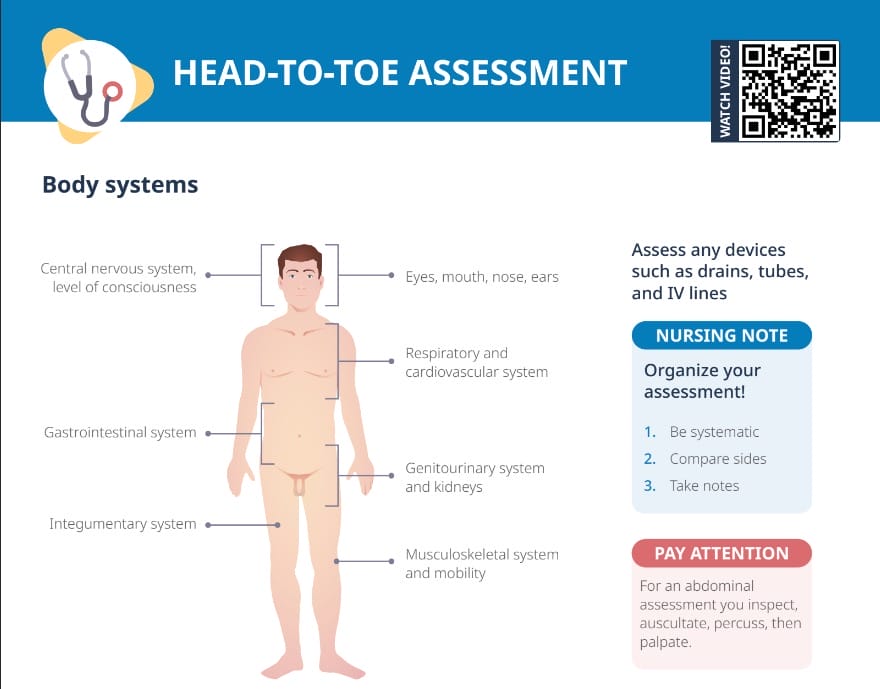
An abdominal assessment is a systematic examination of the client’s abdomen conducted to gather information about the health of the abdominal organs. It helps identify any abnormalities, pain, or changes in the digestive system.
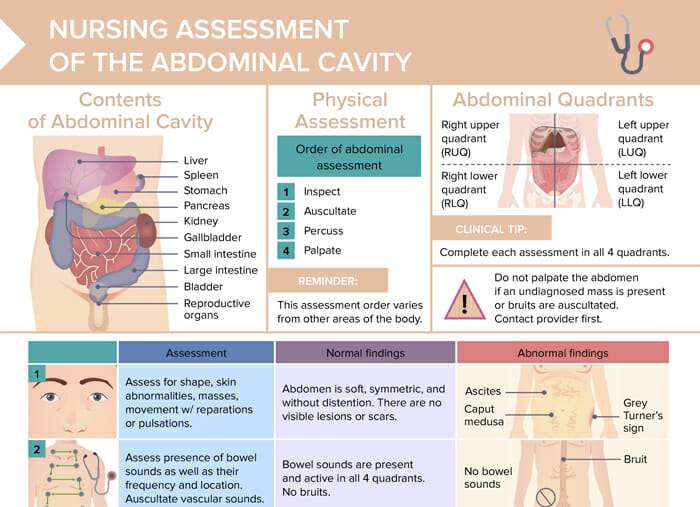
Note: The assessment order for abdominal assessments varies from other areas of the body.
The recommended order for assessing the abdomen is inspection, auscultation, percussion, and then palpation.
This order is different because auscultation of bowel sounds could be altered if palpation or percussion were performed first, potentially leading to inaccurate findings. Auscultating before touching ensures the hearing of the natural state of the abdomen.
Note: Do not palpate the abdomen if an undiagnosed mass is present or bruits are auscultated. Contact provider first.
Note: Complete each assessment in all 4 quadrants.
Percussion of all 4 quadrants
Image by Lecturio.Table: Abdominal assessment findings
| Normal findings | Abnormal findings | |
| Inspection | Abdomen soft, symmetric, without distention; no visible lesions or scars | Ascites, Grey–Turner’s sign, Caput medusa |
| Auscultation | Bowel sounds present and active in all 4 quadrants; no bruits | No bowel sounds; bruit |
| Percussion | General tympany with scattered dullness in all quadrants; dullness heard in upper right quadrant over the liver | Dullness in LLQ could indicate stool, mass, or fluid. |
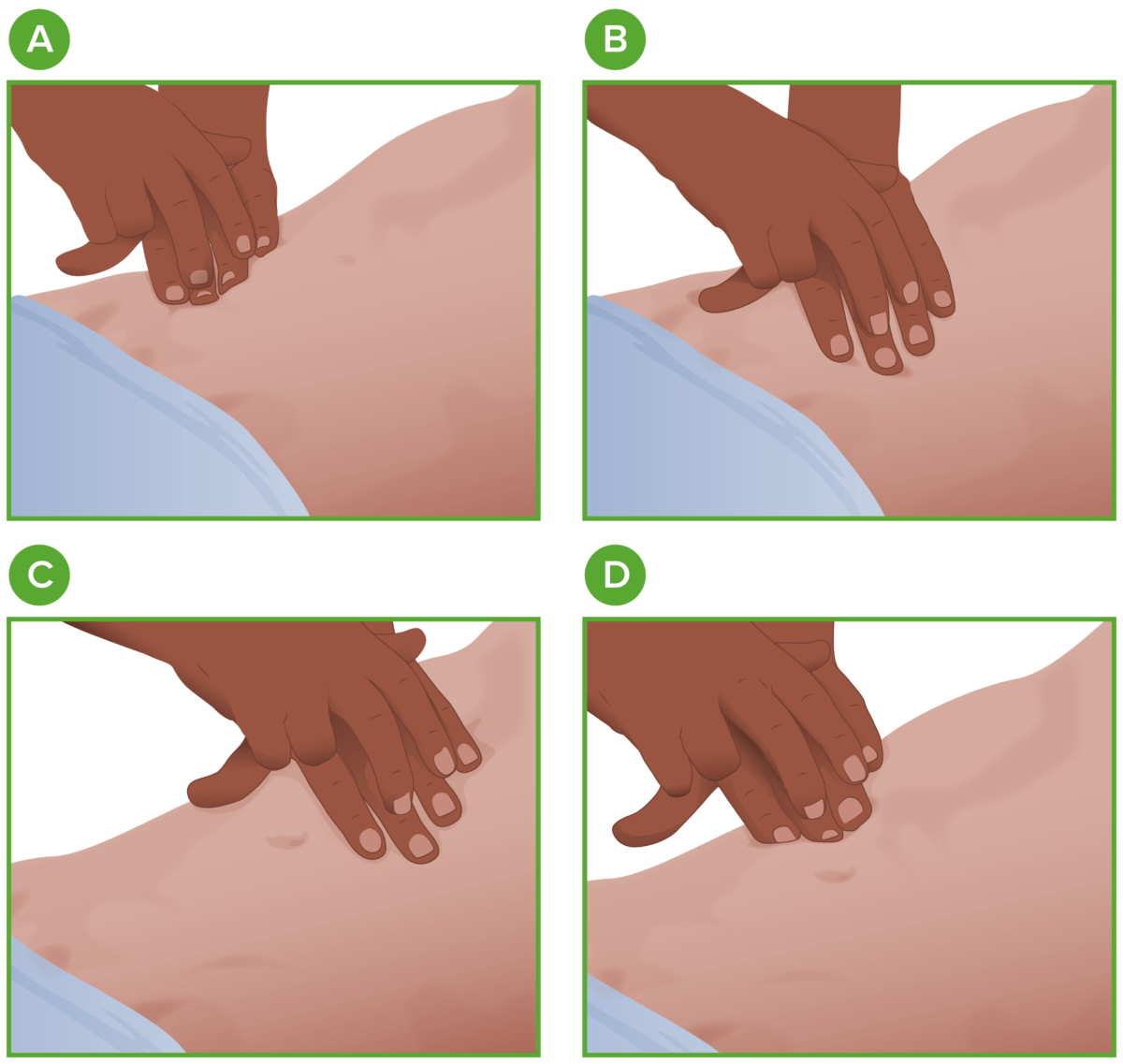
| Palpation | Abdomen soft with no masses, swelling, pain, or rigidity | Pain, mass |