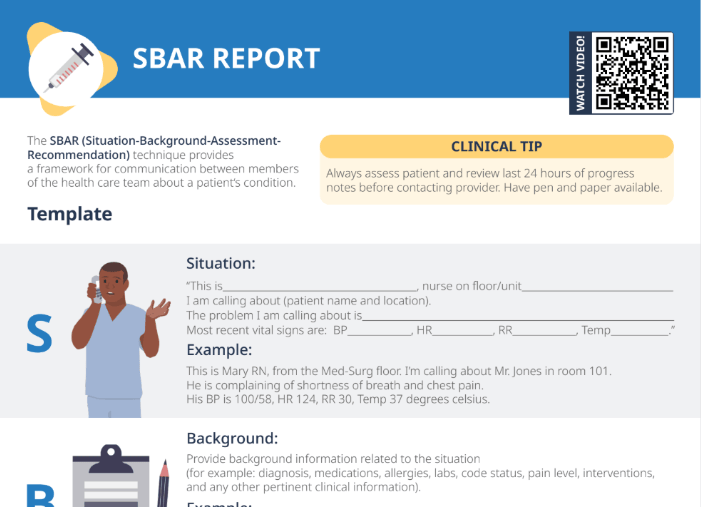
Effective communication is essential in healthcare, especially when it comes to client care. The SBAR (Situation-Background-Assessment-Recommendation) technique is a standardized way of communicating important information about a client’s condition between healthcare team members. This technique is particularly relevant to clinical practice for nurses, who are often responsible for communicating with other healthcare professionals about their clients.