Spinal cord injuries (SCIs) can have profound, life-changing implications for individuals and their families. Nurses play a critical role in the assessment and treatment of SCIs, as well as in providing education and support to clients and their loved ones. This guide provides an overview of the degree of injury, nursing care priorities, and assessment tools used in the care of clients with SCIs, and covers important topics such as complications, client education, and psychological adjustment.
Clients with a suspected SCI should be thoroughly examined using a validated assessment tool, such as the International Standards for Neurological Classification of Spinal Cord Injury from the American Spinal Injury Association (ASIA) examination.
Table: ASIA impairment scale
A
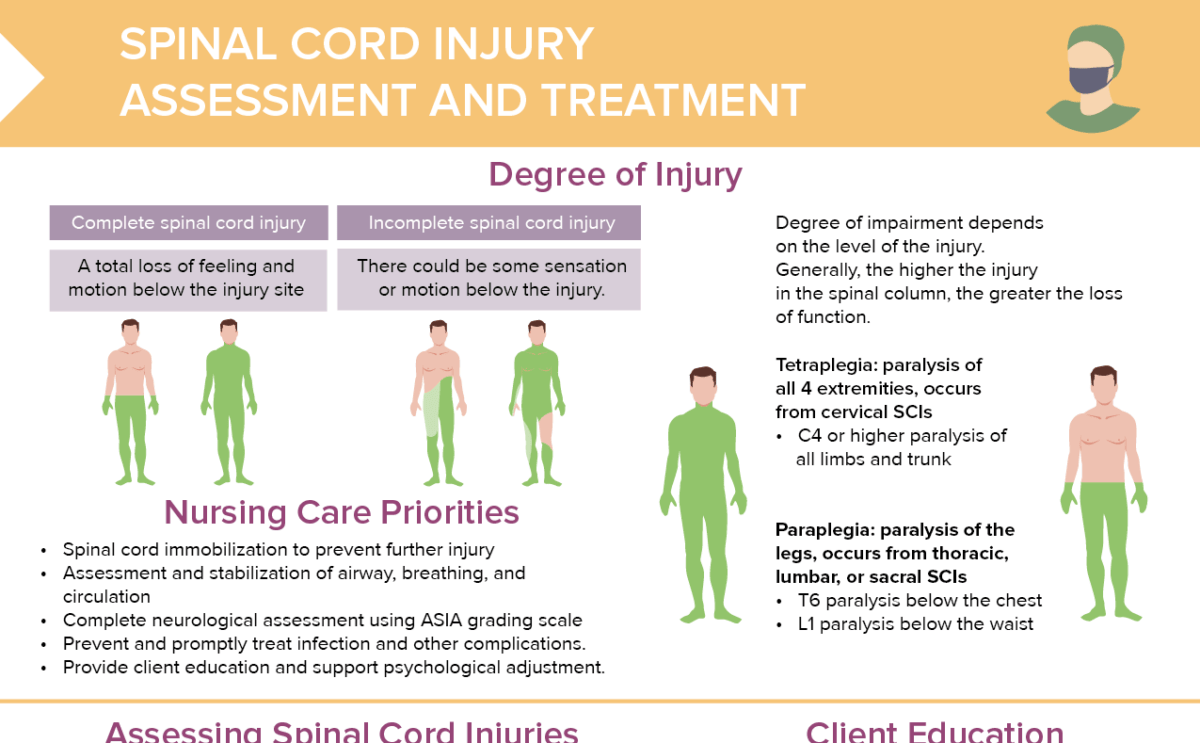
Complete
No sensory or motor function is preserved inthe sacral segments.
B
Incomplete
Sensory function, but not motor function, is preserved below neurological level and extends through sacral segments S4–S5.
C
Incomplete
Motor function is preserved below the neurologic level, and most key muscles below the neurologic level have a muscle grade of less than 3.
D
Incomplete
Motor function is preserved below the neurologic level, and most key muscles below the neurologic level have a muscle grade that is greater than or equal to 3.
E
Incomplete
Sensory and motor functions are normal.
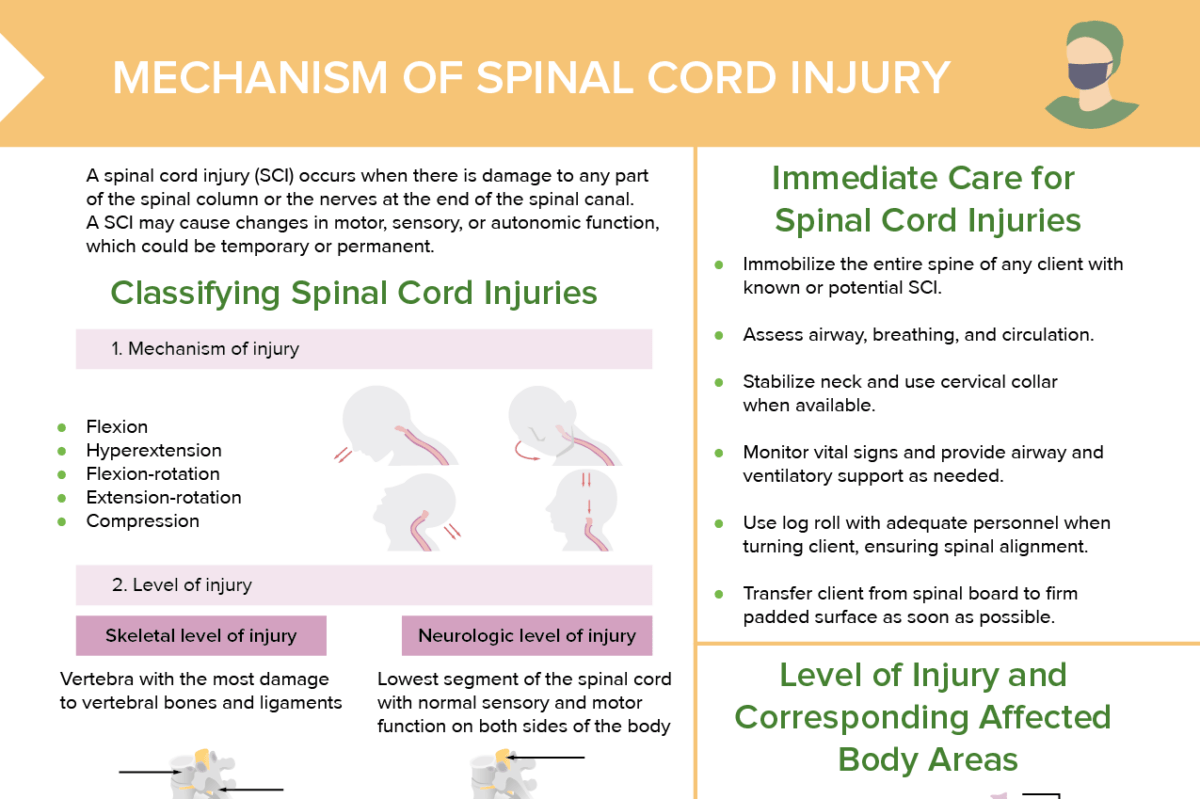
What finding raises suspicion of a complete spinal cord injury?
A complete spinal cord injury is suspected when there is loss of all sensory and motor function below the level of injury, characterized by:
Inability to feel anything in the lower body
Inability to move the lower body
Loss of bladder and bowel control
Findings should be confirmed by imaging studies.
MRI of spinal cord injury: Spinal cord transection at the T6 injury level (arrow) noted in a patient who had a fall from 300 feet.
Image: “Survival following a vertical free fall from 300 feet: the crucial role of body position to impact surface” by Weckbach S, Flierl MA, Blei M, Burlew CC, Moore EE, Stahel PF. License: CC BY 2.0, cropped by Lecturio.
How to educate clients with spinal cord injuries
Teach how to complete ADLs given new limitations.
Consider client’s psychosocial, emotional, and financial needs.
Team will include PT, OT, social work.
Client/family may need additional information on bowel and bladder functioning, sexual health, skin care, pain management, and risk for mental health concerns.
Connect client with home health care and rehabilitation services prior to discharge.
What is spinal shock?
Spinal shock is a temporary condition following a spinal cord injury, characterized by loss of reflexes, sensation, and motor activity below the level of the injury. It can resolve within hours to weeks.
What is neurogenic shock?
Neurogenic shock can be life-threatening. It is a type of distributive shock that can occur with a spinal cord injury above T6, and is characterized by bradycardia and hypotension due to disrupted autonomic pathways.
What is autonomic dysreflexia?
Autonomic dysreflexia is potentially life-threatening. It can occur in clients with SCIs above T6 and is characterized by severe hypertension, headache, and other symptoms, often triggered by a distended bladder or bowel.
How to manage bladder and bowel control in clients with SCIs