Nursing Knowledge
Research in pediatric populations is limited given the ethical considerations involved in conducting medical research on children.
The research we do have reveals wide variation in the pediatric response to medications compared to adults. Immature organ systems put pediatric clients at increased risk for adverse drug reactions. Response to drugs varies by age group and stage of development within the pediatric population, with the youngest clients being most sensitive to medications and most at risk of adverse effects.
The following medications should be avoided in children:
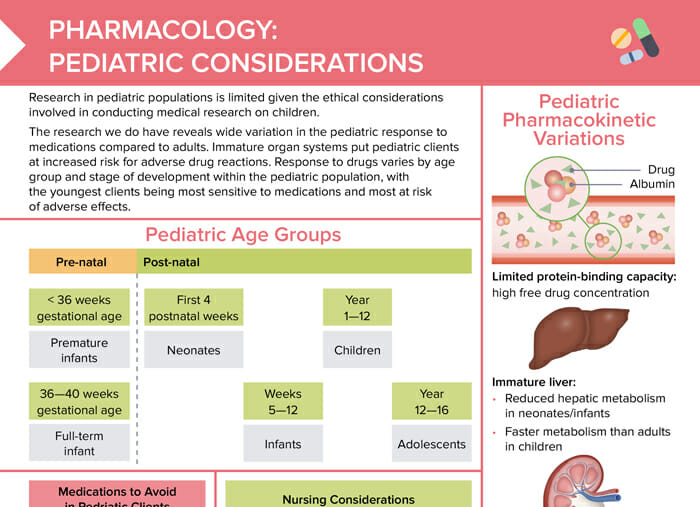
Children’s bodies’ limited protein-binding capacity leads to a high free drug concentration.
Neonates and infants have a reduced hepatic metabolism; while children have a faster metabolism compared to adults.
Renal excretion is reduced in immature kidneys.
Pediatric clients’ blood–brain barrier not being fully developed leads to increased sensitivity to CNS medications.
RELATED TOPIC:
Free Download
Master the topic with a unique study combination of a concise summary paired with video lectures.
Your free account gives you access to:
or