As a nurse, conducting a comprehensive assessment on clients is a crucial skill that forms the foundation of clinical practice. This process involves systematically examining each body system, from the central nervous system to the integumentary system, to gather valuable information about a client’s overall health.
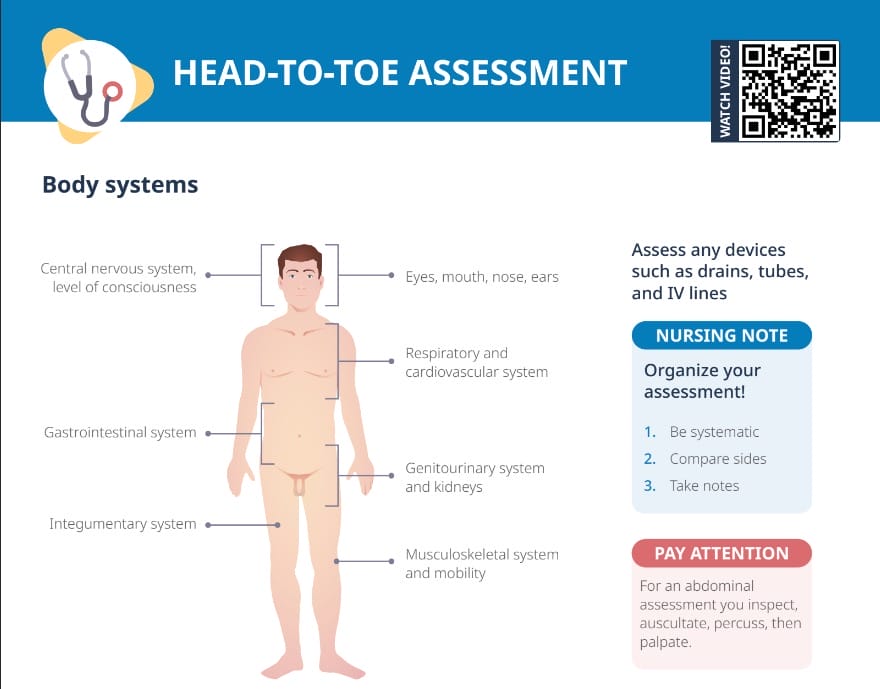
A head-to-toe assessment is a comprehensive method used by nurses and other healthcare providers to evaluate the overall health status of a client. This systematic and structured evaluation includes physical, mental, and physiological assessments, typically starting from the head and moving down the body to the toes.
How to do a head-to-toe assessment
Starting at the head, move down the client’s body, conducting evaluations of each body system:
General impression: level of consciousness, skin color, facial expression, personal hygiene; signs of distress?
Inspection: visual examination, looking for any visible abnormalities (e.g. color changes)
Palpation: manually feeling for abnormalities (e.g. lumps, masses, or areas of tenderness)
Percussion: tapping on the client’s body to produce sounds that can give clues about the underlying structures (e.g. hollow vs dull sounds over lungs)
Auscultation: listening to sounds produced by the body, usually with a stethoscope (heart sounds, breath sounds, bowel sounds)
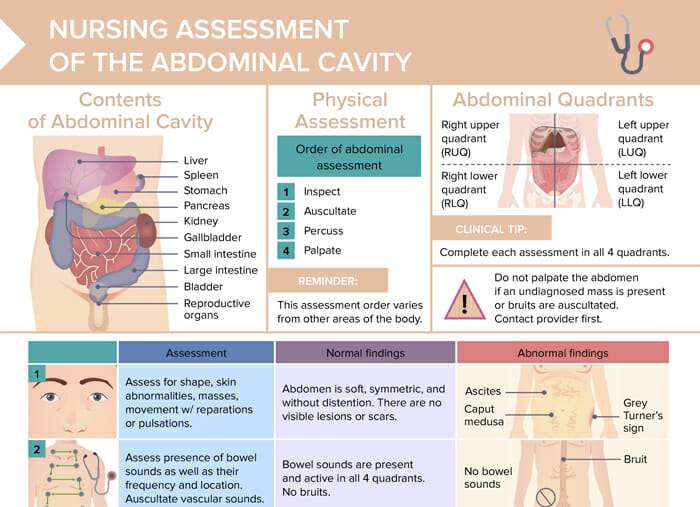
Note: For an abdominal examination, the usual order changes. To assess undisturbed bowel sounds, the order is to inspect, auscultate, percuss, then palpate.
Tips for doing head-to-toe assessments
Be systematic: It’s called head-to-toe for a reason–thoroughly move down the body, taking in the big picture as well as the details of each specific assessment.
Compare sides: Always check both sides and make sure you find asymmetries or issues that may only occur on one side.
Take notes: Note down your findings as you go, so that you don’t forget details when documenting the assessment.
When are head-to-toe assessments done?
Head-to-toe assessments are typically done whenever healthcare personnel need to take stock of a client’s overall health status. This could be when a client is first admitted to a hospital, at the beginning of a nursing shift, whenever there is a significant change in a patient’s condition, or following a regular schedule of assessments based on facility policy or monitoring guidelines.
What kinds of nursing assessments are there?
Different specific physical assessments that nurses do include:
Cardiovascular assessment: heart rate and rhythm, heart sounds, peripheral pulses, and signs of peripheral vascular disease
Respiratory assessment: rate and depth of respiration, ease or difficulty of breathing, lung sounds, and use of accessory muscles
Gastrointestinal assessment: inspection of the abdomen, auscultation of bowel sounds, percussion, palpation for tenderness or masses, and assessing the patient’s appetite, diet, and bowel habits
Neurological assessment: evaluation of level of consciousness, pupil size and reactivity, symmetry and strength of movement, reflexes, sensation, and orientation
Musculoskeletal assessment: assessment of range of motion, muscle strength, and gait, any deformities, pain, or weakness
Skin assessment: inspecting the skin for color, temperature, moisture, turgor, and integrity, any wounds, rashes, or pressure ulcers