Nursing Knowledge
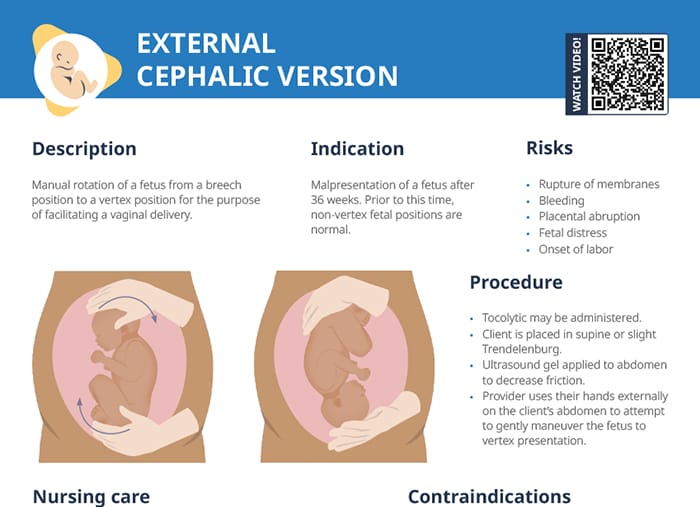
External cephalic version refers to a procedure to manually rotate a fetus from a breech position to a vertex position. Vertex position facilitates vaginal delivery.
External cephalic version is indicated if a fetus is malpresenting after 36 weeks. Prior to this time, non-vertex fetal positions are normal.
External cephalic version is successful approximately 50% of the time.
ECV should not be performed if any the following is present:
Manually rotating a fetus causes a risk of:
A tocolytic may be administered, and an ultrasound gel is applied to the abdomen to decrease friction. The client is placed in supine or slight Trendelenburg position.
The provider uses their hands externally on the client’s abdomen to attempt to gently maneuver the fetus into a vertex position.
After a successful procedure, labor may be induced to decrease the chance of the fetus changing position again.
Internal cephalic version is a more invasive way of repositioning the fetus, with the provider reaching a hand up through the cervix and manually turning the baby there. It is performed less commonly and reserved for specific circumstances.
Make sure to educate clients to notify a provider if:
Some clients experience mild discomfort during the procedure, while others do find it painful. Provide reassurance and check if pain relief options are warranted.
Since an external cephalic version is only successful in half the cases, make sure to manage client expectations before the procedure and explain why an attempt may be recommended anyway in the specific case.
RELATED TOPIC:
Free Download
Master the topic with a unique study combination of a concise summary paired with video lectures.
Your free account gives you access to:
or