Chronic obstructive pulmonary disease (COPD) is a common and serious lung disease that affects millions of people worldwide. It is a progressive disease that causes airflow obstruction, making it difficult to breathe. COPD is a significant cause of morbidity and mortality, and its prevalence is expected to increase in the coming years. Nurses will likely encounter many clients with this condition, regardless of their specific area of practice. Knowing how to provide effective care for clients with COPD, including how to manage symptoms, provide smoking cessation support, and education on using inhalers or supplemental oxygen, is an important skill for many nurses.
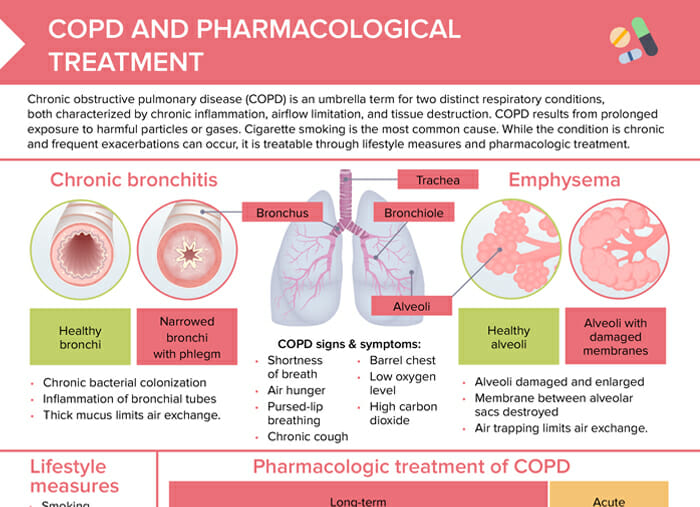
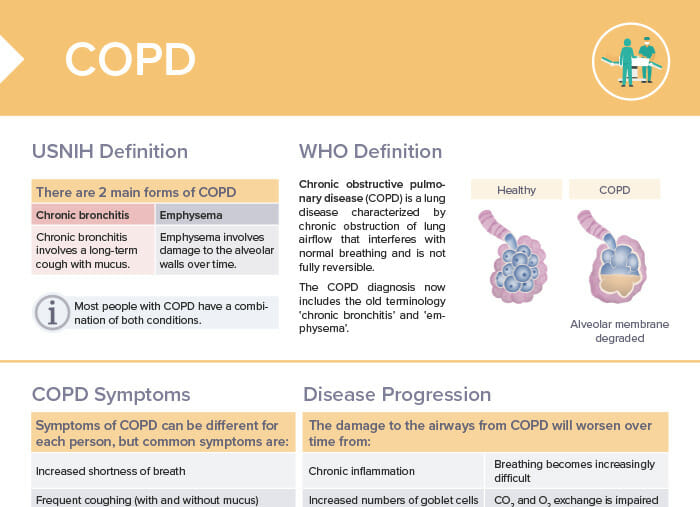
Chronic obstructive pulmonary disease (COPD) is a lung disease characterized by chronic obstruction of lung airflow that interferes with normal breathing and is not fully reversible. COPD is an umbrella term for two distinct respiratory conditions, emphysema and chronic bronchitis. They are both characterized by chronic inflammation, airflow limitation, and tissue destruction. While the condition is chronic and frequent exacerbations can occur, it is treatable through lifestyle measures and pharmacologic treatment.
The most common cause of COPD is long-term exposure to lung irritants (harmful particles or gases), the most common being cigarette smoke.
Other risk factors for the development of COPD include:
Exposure to air pollutants in environment or workplace (dust, chemical fumes)
Alpha-1 antitrypsin deficiency
History of respiratory diseases
Aging
Interference with lung development e.g. through secondhand smoking in childhood
As a nurse, part of your role will be educating clients and communities about these risk factors and promoting behaviors to reduce risk, such as smoking cessation and avoiding exposure to lung irritants.
The symptoms of COPD can vary from person to person. Common symptoms of COPD include:
Frequent coughing (with and without mucus)
Increased breathlessness
Wheezing
Tightness in the chest
Narrowing and reduction in the number of small airways
Air hunger
Pursed-lip breathing
Chronic cough
Barrel chest
Low oxygen level
High carbon dioxide
What are the 4 stages of COPD?
The GOLD staging system of COPD by the Global Initiative for Chronic Obstructive Lung Disease classifies the severity of COPD into 4 stages, primarily based on lung function:
Mild COPD:
Chronic cough possible
FEV1: >= 80%
Moderate COPD:
Symptoms more noticeable (breathlessness, cough, sputum production)
FEV1: 50–80%
Severe COPD:
More severe breathlessness
Possible fatigue, respiratory infections, exacerbations
FEV1: 30–50%
Very severe COPD (end-stage COPD):
Poor quality of life, dyspnea even at rest
FEV1: < 30% of expected value or < 50% with chronic respiratory failure
Note: While classifying COPD into these stages can be helpful, individual symptoms and impact of the disease can vary significantly.
Emphysema vs COPD: What is the difference?
Emphysema is a type of COPD. COPD is an umbrella term that includes both chronic bronchitis and emphysema.
Emphysema specifically involves damage to the alveoli (air sacs) in the lungs, leading to shortness of breath. Chronic bronchitis involves inflamed airways and mucus production. Patients can have one or both conditions. Diagnosis and management require healthcare provider input.
Chronic bronchitis
Chronic bacterial colonization
Inflammation of bronchial tubes
Thick mucus limits air exchange.
Emphysema
Alveoli damaged and enlarged
Membrane between alveolar sacs destroyed
Air trapping limits air exchange.
Bonus download: pharmacological treatment of COPD
COPD Medications
Causes, symptoms, similarities and differences, diagnosis and treatment of Cushing Disease and Cushing Syndrome
The damage to the airways from COPD will worsen over time from:
Chronic inflammation: continuous exposure to irritants like cigarette smoke leads to chronic inflammation in the airways; causes the airway walls to thicken and become scarred
Increased mucus production: due to increased numbers of goblet cells and mucus gland hyperplasia; further obstructs airway
Loss of elasticity: alveolar walls in the lungs become damaged; leads to the loss of elasticity in the lung tissues, making it harder for the lungs to expand and contract during breathing
Air trapping in lungs: due to the collapse of small airways and destruction of alveolar walls; further impairs the exchange of oxygen and carbon dioxide
Pulmonary fibrosis: formation of scar tissue in the lungs; further restricts airflow
Signs of COPD getting worse
Increased shortness of breath
Frequent respiratory infections
Increased fatigue
Increased coughing
Changes in mucus
Decreased activity
Weight loss
Swelling in ankles, feet, or legs
If you notice these signs in your client, it’s important to report them to the healthcare provider as soon as possible for further assessment and treatment adjustments.
What is a COPD flare-up/exacerbation?
A COPD exacerbation is a period of time when COPD symptoms are significantly worse than usually. Exacerbations may be triggered by respiratory infections or exposure to environmental pollutants. COPD exacerbations can be serious and lead to other complications like respiratory failure, so it’s important to seek medical attention promptly. As a nurse, part of your role will be teaching clients to recognize the signs of a flare-up and understand when to seek help, as well as how to avoid known triggers.
Symptoms include:
Increased shortness of breath
Increased coughing
Changes in the color, thickness, or amount of mucus
Increased fatigue
Difficulty sleeping
Decreased appetite
Confusion or decreased alertness (in severe cases)
How is COPD treated?
Some specific aspects of COPD treatment from the perspective of nursing care include:
Medication management: educating clients on how to properly use prescribed medications/inhalers, such as bronchodilators, corticosteroids, or antibiotics
Patient education on medication adherence, how to recognize and manage exacerbations, and lifestyle modifications such as smoking cessation, exercise, and a healthy diet
Breathing techniques and exercise: teaching strategies to manage shortness of breath, encouraging physical activity
Managing oxygen therapy and teaching clients and families how to safely use and maintain oxygen equipment at home
Monitoring vital signs, lung function, and overall symptoms
Care coordination with respiratory therapists, physiotherapists, dietitians, and social workers
Emotional support for client and family
End-of-life care: discussions about advance directives, palliative care options, and hospice care in advanced cases
In general, the nursing care for a client with COPD should be individualized, client-centered, and focused on optimizing quality of life and reducing the risk of exacerbations.
Lifestyle measures
Smoking cessation, if applicable
Pulmonary rehabilitation
Pharmacological treatment of COPD
Long-term treatment:
Bronchodilators
Promote smooth muscle relaxation and prevent bronchoconstriction
LABAs, LAMAs, methylxanthines
Inhaled corticosteroids
Decrease inflammation
Combine with LABA or LAMA
Beclomethasone
Budesonide
Fluticasone
Methylxanthines
Phosphodiesterase-4 inhibitors
Used in severe cases
Reduce inflammation by preventing breakdown of intracellular cyclic AMP
Roflumilast
Acute treatment:
Short-acting bronchodilators (SABAs)
Oral corticosteroids
Antibiotics if concern for bacterial infection
Oxygen therapy, ranging from nasal cannula to mechanical ventilation based on severity
Emphysema vs COPD: What is the difference?
Emphysema is one of the 2 main forms of COPD: chronic bronchitis and emphysema.
Chronic bronchitis: involves a long-term cough with mucus
Emphysema: involves damage to the alveolar walls over time
Note: Most people with COPD have a combination of both conditions.
Asthma vs COPD: What is the difference?
The difference between asthma and COPD is based on the combination of conditions and symptoms present:
Asthma with reversible airflow obstruction → not COPD
Chronic bronchitis and/or emphysema but no airflow obstruction → not COPD
Chronic bronchitis and/or emphysema with non-reversible airflow obstruction → COPD
Asthma–COPD overlap syndrome is identified in clinical practice by the features that it shares with both asthma and COPD. (Global Initiative for Chronic Obstructive Lung Disease (GOLD) and GINA Science Committees)
Chronic obstructive pulmonary disease is one of the most common respiratory conditions. Never forget the signs and symptoms and how it differs from asthma with this cheat sheet!
Master the topic with a unique study combination of a concise summary paired with video lectures.