Peptic ulcer disease encompasses conditions characterized by the erosion of the stomach or duodenal lining, resulting in gastric or duodenal ulcers. These ulcers arise due to factors like Helicobacter pylori infection or prolonged NSAID use. For nurses, understanding PUD is vital because of its prevalence and potential complications like bleeding or perforation.
A stomach ulcer is an open sore (ulcer) that develops in the lining of the stomach.
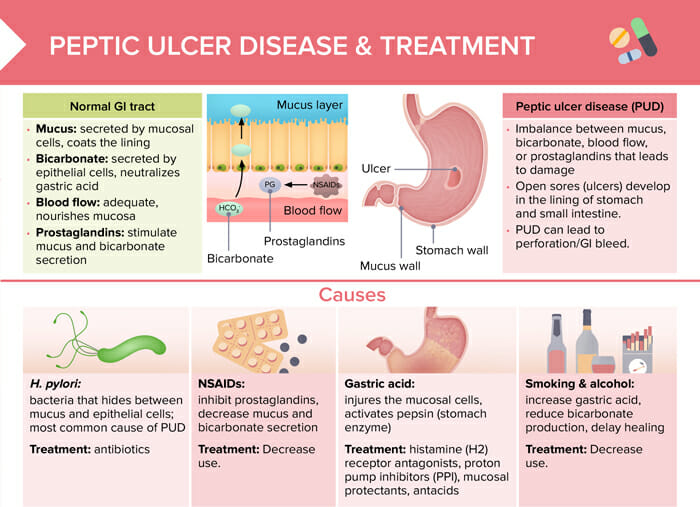
It is a manifestation of peptic ulcer disease – an imbalance between mucus, bicarbonate, blood flow, or prostaglandins that leads to damage and perforation/GI bleed, which develops into ulcers in the stomach and small intestine.
Background:
Mucus is the secretion of the mucosal cells that coats the lining of the GI tract. Bicarbonate is secreted by epithelial cells and neutralizes gastric acid. Adequate blood flow nourishes the mucosa. Prostaglandins stimulate mucus and bicarbonate secretion.
What causes stomach ulcers?
Common causes of PUD and stomach ulcers include:
Helicobacter pylori (H. pylori): bacteria that hides between mucus and epithelial cells (most common cause)
NSAIDs: inhibit prostaglandins, decrease mucus and bicarbonate secretion
Gastric acid: injures the mucosal cells, activates pepsin (stomach enzyme)
Diagnosing stomach ulcers (gastric ulcers) involves a combination of clinical evaluation and specific diagnostic tests. Here are the primary methods used to diagnose gastric ulcers:
Clinical history and physical examination:
Symptoms of burning stomach pain, bloating, heartburn, nausea, or vomiting
Review use of medications, (e.g., NSAIDs, aspirin)
Check for complications, like signs of bleeding (dark, tarry stools or vomiting blood)
Esophagogastroduodenoscopy: most direct way to visualize and diagnose a gastric ulcer
Barium swallow test
Tests for Helicobacter pylori (blood test for antibodies, urea breath test, stool antigen test, biopsy)
Tests for anemia (which might indicate bleeding from the ulcer) using a complete blood count (CBC)
The duration of a stomach (gastric) ulcer can vary based on its cause, severity, and the effectiveness of treatment. Generally:
With proper treatment, most uncomplicated gastric ulcers heal within 4–8 weeks with proper treatment.
Without treatment, ulcers might gradually heal on their own, but this can take much longer and may be accompanied by complications such as bleeding, perforation, or obstruction. Some ulcers may become chronic and persist for extended periods, especially if the underlying causative factors such as NSAID use or H. pylori infection are not addressed.
How to sleep with a stomach ulcer
Clients with stomach ulcers may have trouble sleeping due to pain or acid reflux. Here are some recommendations that can help alleviate these issues and help better sleep quality:
Elevate the head to prevent acid reflux
Eat the last meal about 3 hours before and limit liquids before bedtime
Sleep on the left side
Stop smoking, if applicable
Limit trigger foods like caffeine and spicy foods
Manage stress and create a calm sleep environment
Follow prescribed medication plan
Nursing diagnosis for peptic ulcer disease
For peptic ulcer disease (PUD), relevant nursing diagnoses can include:
Acute pain related to the inflammatory response and increased gastric acid secretion.
Imbalanced nutrition: less than body requirements related to anorexia, nausea, and vomiting
Disturbed sleep pattern related to nocturnal pain or discomfort
Activity intolerance related to generalized weakness or associated anemia
Risk for perforation related to the progressive erosion of the gastric or duodenal lining
Risk for bleeding related to erosion of the gastric or duodenal lining
Stomach ulcers treatments
It is important to address the underlying cause of the stomach ulcer: