Nursing Knowledge
RELATED STUDY SHEET
Nursing notes are written records detailing the care provided to a client, including observations, treatment plans, and interventions. They are essential for continuity of care and are a legal document.
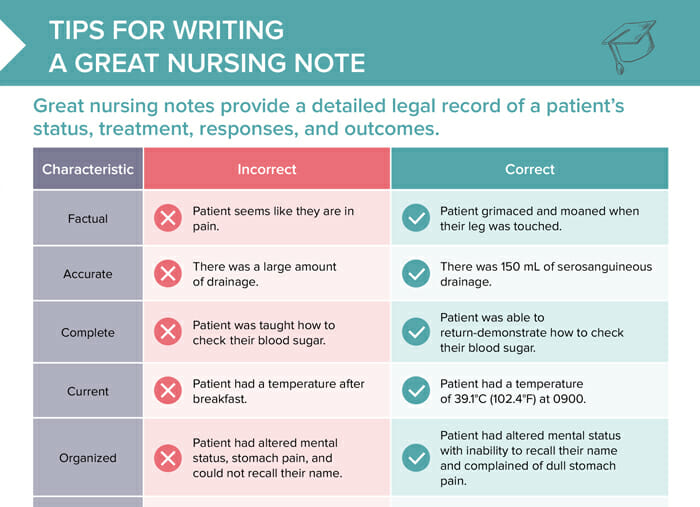
Good nursing notes provide a detailed legal record of a client’s status, treatment, responses, and outcomes.
All nursing notes must be:
Tips for writing nursing notes:
Writing nursing notes in a narrative format means telling the client’s story chronologically. The note will provide the information in free, written-out sentences.
An advantage is that notes in this format provide context and a fuller picture of the client’s situation, but they can be time-consuming to read and write.
“SOAP” is short for “Subjective, Objective, Assessment, and Plan”.
Giving nursing notes this structure creates easier reading to scan quickly and reduces the possibility of errors and oversights by providing a standardized, focused documentation.
The SOAP-format is often expanded to “SOAPIE”: Subjective, Objective, Assessment, Plan, Intervention and Evaluation.
An example for this format would be:
Following are examples of nursing note excerpts that show the dos and don’ts of how to follow the requirements of a good nursing note:
Don’t: Client seems like they are in pain.
Do: Client grimaced and moaned when their right leg was touched.
Interpretations and assumptions are not facts.
Don’t: There was a large amount of drainage.
Do: 0910-Serosanguineous drainage of 150 mL.
“Large amount” as a quantifier leaves the information open to the reader’s interpretation. Stick to the facts and give them in the most detailed way possible.
Don’t: Client was taught how to check their blood sugar.
Do: Client correctly demonstrates how to check their blood glucose.
Include how the teaching was done and the proof that it was successful.
Don’t: Client had an elevated temperature after breakfast.
Do: 0900-client’s temperature is 39.1°C (102.4°F)
This example shows again that it is important to be specific, precise, and to give all the available information.
Don’t: Client had altered mental status, stomach pain, and could not recall their name.
Do: Client disoriented to time; points to dull stomach pain around umbilicus at 5/10 pain level.
Group related information together.
Don’t: Client uncooperative and would not take meds.
Do: Client refused 0900 meds.
It is inappropriate to label clients as difficult, uncooperative, or use a negative description – simply state the actions, what happened, quotes stated and everything that may have kept you from taking measures you were supposed to. Leave out any personal perspectives, reactions, or feelings.
Free Download
Master the topic with a unique study combination of a concise summary paired with video lectures.
Your free account gives you access to:
or