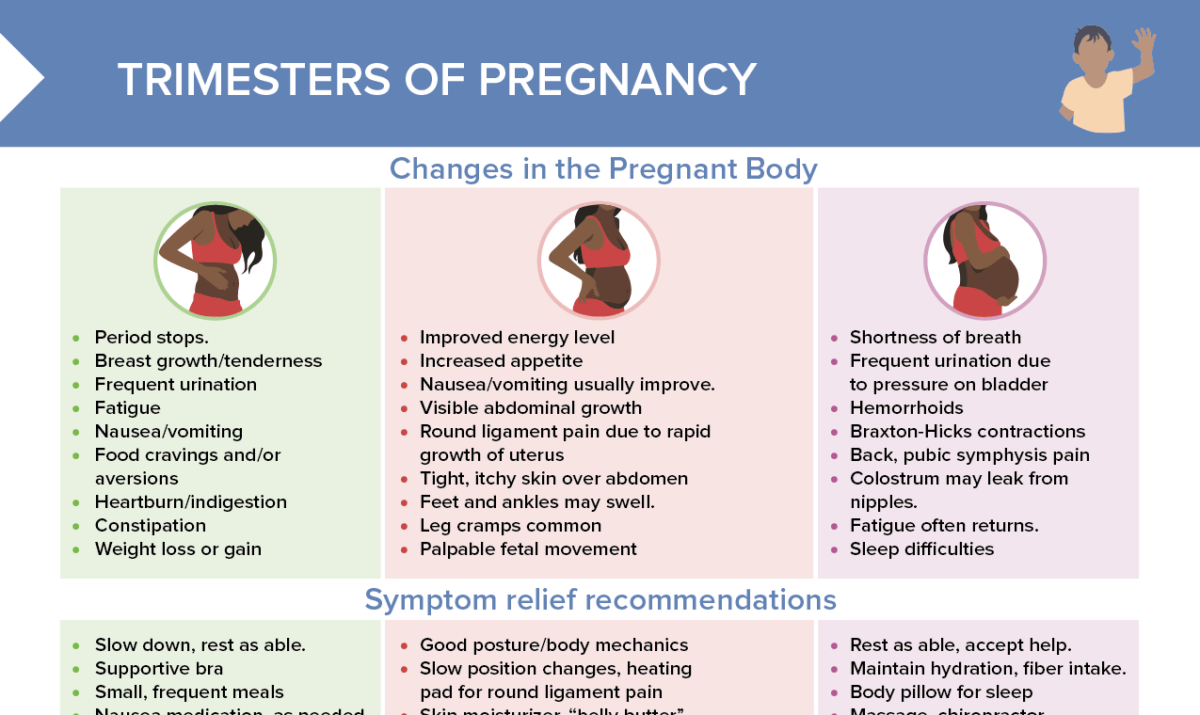
Pregnancy induces a cascade of remarkable physiological alterations in a woman’s body to support fetal development. In the clinical setting, understanding these changes is pivotal for nurses to distinguish between normal pregnancy-related changes and potential pathologies.
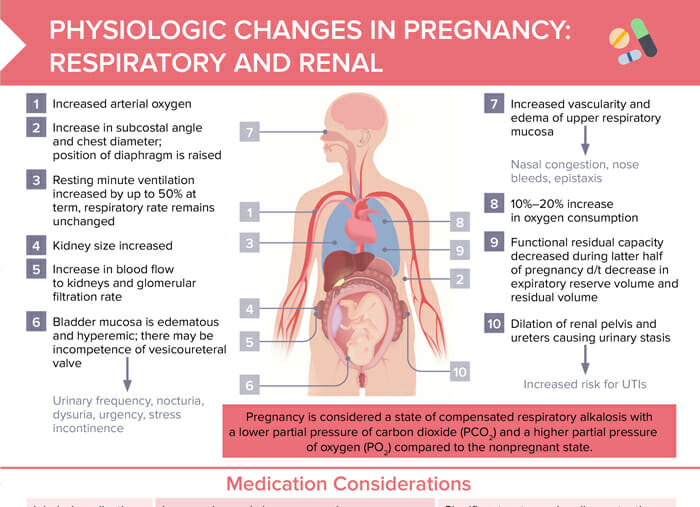
Increase in subcostal angle and chest diameter; position of diaphragm is raised
Increased kidney size
Resting minute ventilation increased by up to 50% at term (respiratory rate remains unchanged)
Increase in blood flow to kidneys and glomerular filtration rate
Bladder mucosa is edematous and hyperemic; there may be incompetence of vesicoureteral valve (→ urinary frequency, nocturia, dysuria, urgency, stress incontinence)
Increased vascularity and edema of upper respiratory mucosa (→ nasal congestion, nose bleeds, epistaxis)
10–20% increase in oxygen consumption
Functional residual capacity decreased during latter half of pregnancy d/t decrease in expiratory reserve volume and residual volume
Dilation of renal pelvis and ureters causing urinary stasis (-→increased risk for UTIs)
Tip: Pregnancy is considered a state of compensated respiratory alkalosis with a lower partial pressure of carbon dioxide (PCO2) and a higher partial pressure of oxygen (PO2) compared to the nonpregnant state.
During pregnancy, 30 minutes of moderate-intensity aerobic activity is recommended ≥ 5 days a week to support respiratory health.
Pregnant clients are at higher risk of severe illness from respiratory disease than non-pregnant clients. Recommend vaccines per guidelines.
Free download: Renal and respiratory changes in pregnancy
Overview of respiratory and renal changes during pregnancy, effect on medications, and client education
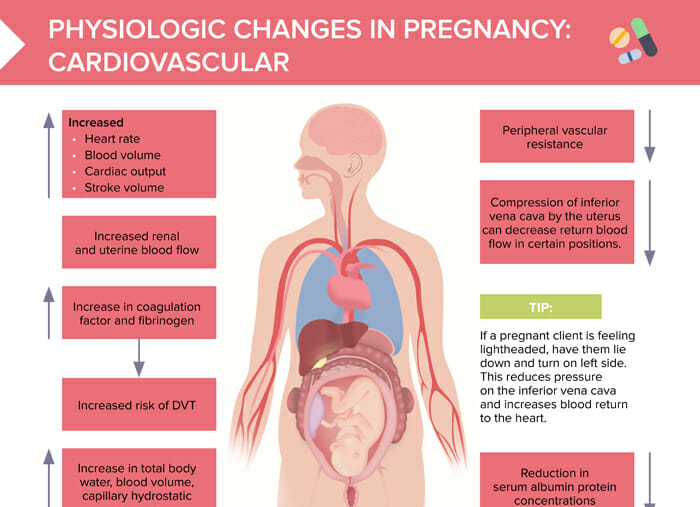
Tip: If a pregnant client is feeling lightheaded, instruct the client to lie down and turn onto the left side. This reduces pressure on the inferior vena cava and increases blood return to the heart.
Increase in:
Heart rate
Blood volume
Cardiac output
Stroke volume
Renal and uterine blood flow
Coagulation factor and fibrinogen (→ increased risk of DVT)
Total body water/blood volume/capillary hydrostatic pressure (→ forces fluid out of capillaries → swelling)
Decrease in:
Peripheral vascular resistance
Return blood flow in certain positions (due to compression of inferior vena cava by the uterus)
Serum albumin protein concentrations (→ less ability to hold fluid in capillaries → swelling)
Medication considerations during pregnancy
Special considerations related to respiratory and renal changes
Inhaled medications may be more readily absorbed.
Increase in renal clearance can increase elimination rates of renally cleared medications, leading to shorter half lives (e.g., lithium, ampicillin, cefuroxime, cephradine, cefazolin, piperacillin, atenolol, digoxin)
Significant water and sodium retention during pregnancy leads to hemodilution. This causes reduced peak serum concentrations of hydrophilic drugs.
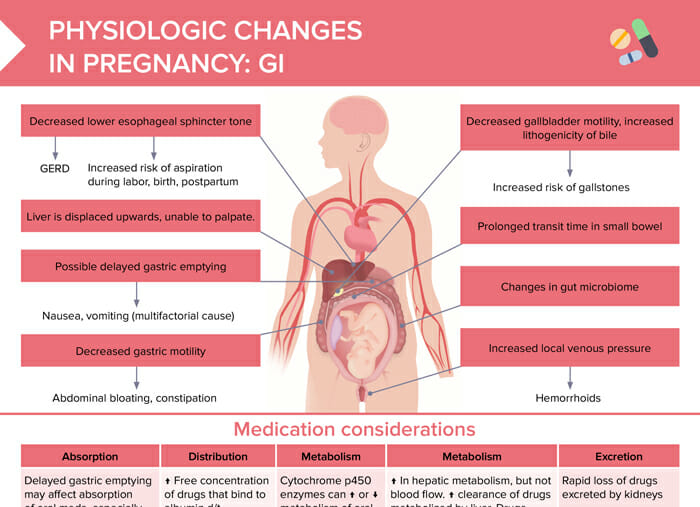
Special considerations related to GI changes
Absorption:
Delayed gastric emptying may affect absorption of oral meds, especially during labor.
IM meds are not affected.
Distribution: ↑ free concentration of drugs that bind to albumin d/t hemodilution
Metabolism:
Cytochrome p450 enzymes can ↑ or ↓ metabolism of oral drugs in the liver during pregnancy.
↑ In hepatic metabolism, but not blood flow
↑ Clearance of drugs metabolized by liver
Drugs that depend on delivery to the liver (blood flow) are unaltered.
Excretion: rapid loss of drugs excreted by kidneys
Special considerations related to cardiovascular changes
Due to increased total body water, hydrophilic drugs may require higher initial and maintenance doses.
There can be an increased amount of unbound (active) drugs in pregnant clients due to lower serum protein levels.
Permanent body changes after pregnancy
Most physiologic pregnancy changes are temporary. Pregnancy-induced physiologic changes to respiratory and renal systems should return to non-pregnant state by 4–6 weeks postpartum. GI changes often resolve after delivery (with some exceptions like hemorrhoids or GI muscle tone). Cardiovascular changes immediately begin to reverse with delivery and return to pre-pregnancy levels quickly, with the possible exception of cardiac remodeling that has happened during pregnancy which can take a few months to return to previous state.
Some changes that come with pregnancy can be long-lasting or permanent. Examples of more common permanent changes include:
Breast changes (different size and shape)
Foot size (may remain increased)
Stretch marks and varicose veins
Abdominal changes (e.g. diastasis recti, a persistent separation of the abdominal muscles)
Skin changes (e.g. melasma or linea nigra that may fade but not completely disappear)
Weight (may be difficult to return to previous body composition even with diet and exercise)