A reação de hipersensibilidade tipo III, também conhecida como hipersensibilidade mediada por complexos imunes, ocorre quando anticorpos e antigénios formam complexos imunes ( CI CI The percentage of the chest diameter occupied by the heart. Imaging of the Heart and Great Vessels) em circulação, que se depositam em tecidos suscetíveis. O sistema do complemento desencadeia a resposta imunológica, levando ao recrutamento de leucócitos e a lesões teciduais. Não há uma síndrome clínica única para esta hipersensibilidade. Os sintomas refletem o comprometimento de múltiplos sistemas de órgãos com base nos locais de deposição de CI CI The percentage of the chest diameter occupied by the heart. Imaging of the Heart and Great Vessels. A abordagem diagnóstica depende em grande parte da anamnese, incluindo testes Testes Gonadal Hormones laboratoriais, imagiologia e biópsia do órgão afetado. O tratamento consiste na remoção ou evicção de agentes agressores e, em condições graves, glucocorticoides ou terapêutica imunossupressora.
Last updated: Dec 15, 2025
Formação de complexos imunes: CI CI The percentage of the chest diameter occupied by the heart. Imaging of the Heart and Great Vessels é formado pela ligação entre Ag AG Metabolic Acidosis e Ab
Deposição do complexo imune
A deposição do complexo imune depende de:
Reação inflamatória do complexo imune
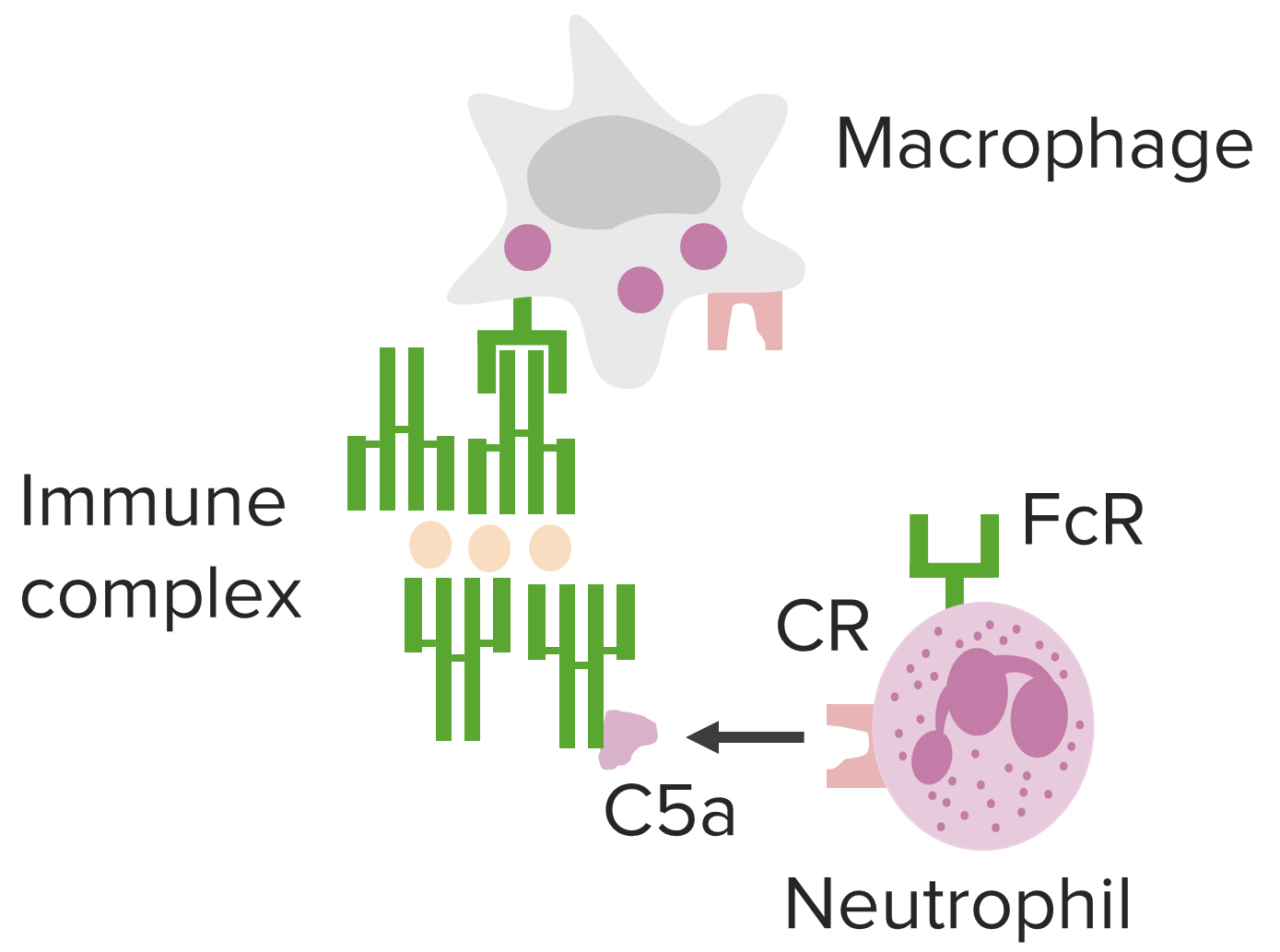
Vias mediadas por complexos imunes, subjacentes à hipersensibilidade tipo III.
Imagem de Lecturio.As manifestações clínicas dependem da porta de entrada, do(s) local(is) de deposição dos CIs CIS Multiple Sclerosis e da persistência do(s) antigénio(s).

Lesão tecidual da parede dos vasos sanguíneos mediada por CI na reação de hipersensibilidade tipo III, vasculite, com associação a várias patologias.
Imagem de Lecturio.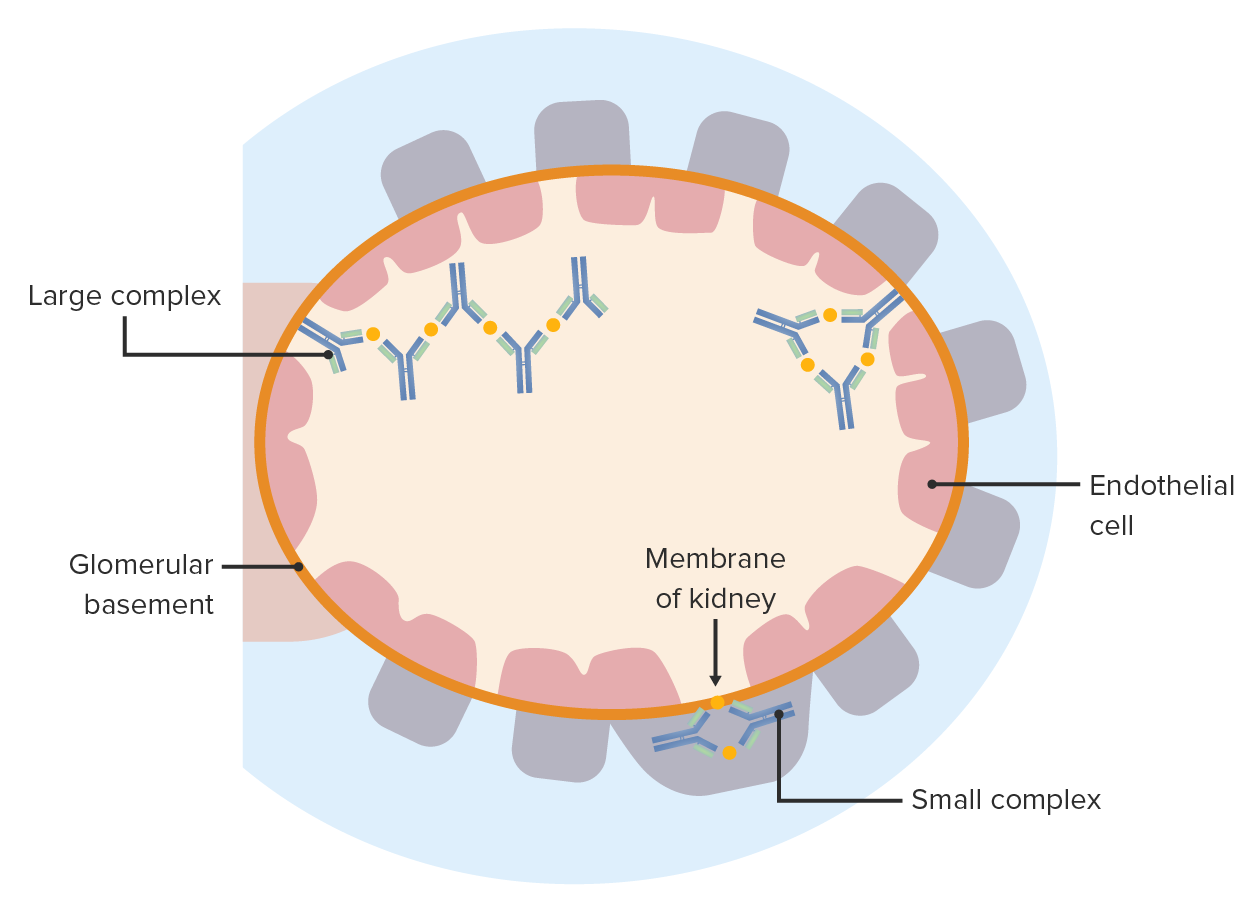
Doença por complexos imunes: os complexos antigénio-anticorpo depositam-se em qualquer lado da membrana basal glomerular. Estes provocam uma reação inflamatória e causam uma lesão glomerular.
Imagem de Lecturio.
Uma paciente do sexo feminino com 27 anos com antecedentes de exposição ao bolor. A tomografia computorizada de alta resolução do tórax (janela pulmonar) ao nível dos lobos inferiores mostra opacidades extensas em vidro despolido (asteriscos), com focos sobrepostos de retenção de ar lobular (setas).
Imagem: “Hypersensitivity Pneumonitis” de Torres PP, Moreira MA, Silva DG, da Gama RR, Sugita DM, Moreira MA. Licença: CC BY 4.0