Osteogenesis imperfecta (OI), ou "doença dos ossos frágeis", é uma doença genética rara do tecido conjuntivo caracterizada por uma fragilidade óssea grave. Embora a OI seja considerada uma única doença, inclui mais de 16 genótipos e fenótipos clínicos com diferentes graus de gravidade dos sintomas. Destes 16, os tipos I-IV são os mais comuns. Devido à raridade da OI, esta é considerada uma "doença órfã" nos Estados Unidos. O diagnóstico é feito clinicamente, através da história e do exame objetivo, e é confirmado com achados imagiológicos e análise do DNA DNA A deoxyribonucleotide polymer that is the primary genetic material of all cells. Eukaryotic and prokaryotic organisms normally contain DNA in a double-stranded state, yet several important biological processes transiently involve single-stranded regions. DNA, which consists of a polysugar-phosphate backbone possessing projections of purines (adenine and guanine) and pyrimidines (thymine and cytosine), forms a double helix that is held together by hydrogen bonds between these purines and pyrimidines (adenine to thymine and guanine to cytosine). DNA Types and Structure. Embora não haja uma cura definitiva, o tratamento é de suporte, geralmente envolvendo bisfosfonatos, e foca-se na redução da dor, redução da frequência de fraturas, redução da deformidade óssea e aumento da deambulação. O prognóstico é variável, dependendo do tipo de OI.
Last updated: Dec 15, 2025
Osteogenesis imperfecta Osteogenesis imperfecta Osteogenesis imperfecta (OI), or “brittle bone disease,” is a rare genetic connective tissue disorder characterized by severe bone fragility. Although OI is considered a single disease, OI includes over 16 genotypes and clinical phenotypes with differing symptom severity. Osteogenesis Imperfecta (OI) é uma doença hereditária do tecido conjuntivo caracterizada por défices na formação óssea e fragilidade óssea grave.
| Type I | Type II | Type III | Type IV | |
|---|---|---|---|---|
| Mutated gene Gene A category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms. Basic Terms of Genetics | COL1A1, COL1A2 ( collagen Collagen A polypeptide substance comprising about one third of the total protein in mammalian organisms. It is the main constituent of skin; connective tissue; and the organic substance of bones (bone and bones) and teeth (tooth). Connective Tissue: Histology type 1 Type 1 Spinal Muscular Atrophy alpha 1 and 2 chains) | COL1A1, COL1A2, and CRTAP ( cartilage-associated protein Cartilage-Associated Protein Osteogenesis Imperfecta) | COL1A1, COL1A2 | COL1A1, COL1A2 |
| Inheritance modality | Autosomal dominant Autosomal dominant Autosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance | Autosomal dominant Autosomal dominant Autosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance AND autosomal recessive Autosomal recessive Autosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal recessive diseases are only expressed when 2 copies of the recessive allele are inherited. Autosomal Recessive and Autosomal Dominant Inheritance | Autosomal dominant Autosomal dominant Autosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance | Autosomal dominant Autosomal dominant Autosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance |
| Defect | Frameshift mutations in collagen Collagen A polypeptide substance comprising about one third of the total protein in mammalian organisms. It is the main constituent of skin; connective tissue; and the organic substance of bones (bone and bones) and teeth (tooth). Connective Tissue: Histology type 1 Type 1 Spinal Muscular Atrophy alpha 1 and 2 chains leading to decreased amounts of normal collagen Collagen A polypeptide substance comprising about one third of the total protein in mammalian organisms. It is the main constituent of skin; connective tissue; and the organic substance of bones (bone and bones) and teeth (tooth). Connective Tissue: Histology | Disrupted formation of the collagen Collagen A polypeptide substance comprising about one third of the total protein in mammalian organisms. It is the main constituent of skin; connective tissue; and the organic substance of bones (bone and bones) and teeth (tooth). Connective Tissue: Histology triple helix structure, leading to little or no normal collagen Collagen A polypeptide substance comprising about one third of the total protein in mammalian organisms. It is the main constituent of skin; connective tissue; and the organic substance of bones (bone and bones) and teeth (tooth). Connective Tissue: Histology | Mutations causing structural protein defects leading to severe pathology | Mutations causing structural protein defects leading to minimal or mild pathology |
| Type I | Type II | Type III | Type IV | |
|---|---|---|---|---|
| Description | Non-deforming with blue sclerae Blue Sclerae Osteogenesis Imperfecta | Perinatally lethal | Progressively deforming | Variable Variable Variables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups. Types of Variables with normal sclerae |
| Severity | Mild | Perinatal lethal | Severe | Mild to moderate |
| Fractures | < 100 | > 100 | > 100 | > 100 |
| Bone Bone Bone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types deformity Deformity Examination of the Upper Limbs | Uncommon | Severe | Moderate to severe | Mild to moderate |
| Stature | Normal to mildly reduced | Severely reduced | Reduced | Variable Variable Variables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups. Types of Variables |
| Dentogenesis imperfecta | Variable Variable Variables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups. Types of Variables | Common | Common | Variable Variable Variables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups. Types of Variables |
| Color of sclerae | Blue | Dark blue | Blue | Normal to gray |
| Hearing loss Hearing loss Hearing loss, also known as hearing impairment, is any degree of impairment in the ability to apprehend sound as determined by audiometry to be below normal hearing thresholds. Clinical presentation may occur at birth or as a gradual loss of hearing with age, including a short-term or sudden loss at any point. Hearing Loss | Present in approximately 50% | — | Frequent | Variable Variable Variables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups. Types of Variables |

Blue-colored sclera associated with OI
Image: “Blue sclera” by the Department of Medical Oncology, Ankara University School of Medicine, 06300 Ankara, Turkey. License: CC BY 3.0.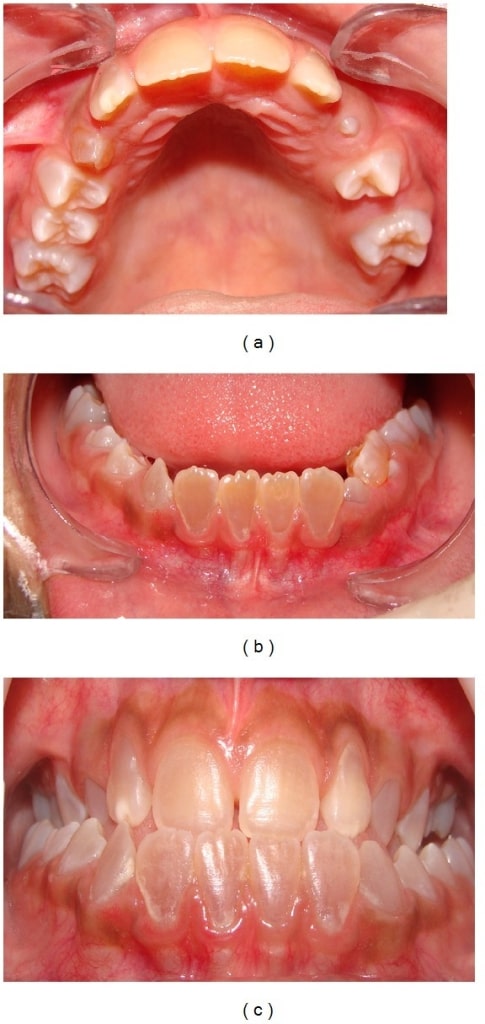
Dentinogenesis imperfecta:
Anterior teeth show a brownish discoloration (upper dental arch (a), lower arch (b), and dental occlusion(c)).

Intraoral photograph showing yellowish discoloration and chipping of the dentition: A 4-year-old male child with OI (type IV)
Image: “Chipping of the dentition” by the Department of Oral Medicine and Radiology, AB Shetty Memorial Institute of Dental Sciences, Nitte University, Mangalore 575018, India. License: CC BY 3.0.
Infant with OI: Notice the deformity of the limbs, an indication of possible fractures during inspection.
Image: “Congenita A type of osteogenesis imperfecta” by the Maria Sklodowska Curie Clinical Emergency Hospital for Children, Bucharest, Romania. License: CC BY 2.0.| Type I | Type II | Type III | Type IV | |
|---|---|---|---|---|
| Skull Skull The skull (cranium) is the skeletal structure of the head supporting the face and forming a protective cavity for the brain. The skull consists of 22 bones divided into the viscerocranium (facial skeleton) and the neurocranium. Skull: Anatomy radiographic findings | Intra-sutural bones | Undermineralization; calcified areas | Intra-sutural bones | Intra-sutural bones (sometimes) |
| Spine Spine The human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum. Vertebral Column: Anatomy radiographic findings | Biconcave vertebrae (adults) | Widened vertebral bodies (platyspondyly) | Biconcave vertebrae; kyphoscoliosis Kyphoscoliosis Osteomalacia and Rickets | Biconcave vertebrae |
| Extremity radiographic findings | Thin cortices | Severely deformed femurs | Flared metaphyses, bowing, thin cortices | Thin cortices |
| Other radiographic findings | Osteopenia Osteopenia Osteoporosis | Small, beaded ribs Ribs A set of twelve curved bones which connect to the vertebral column posteriorly, and terminate anteriorly as costal cartilage. Together, they form a protective cage around the internal thoracic organs. Chest Wall: Anatomy (pathognomonic) | Thin ribs Ribs A set of twelve curved bones which connect to the vertebral column posteriorly, and terminate anteriorly as costal cartilage. Together, they form a protective cage around the internal thoracic organs. Chest Wall: Anatomy, severe osteoporosis Osteoporosis Osteoporosis refers to a decrease in bone mass and density leading to an increased number of fractures. There are 2 forms of osteoporosis: primary, which is commonly postmenopausal or senile; and secondary, which is a manifestation of immobilization, underlying medical disorders, or long-term use of certain medications. Osteoporosis | Protrusio acetabuli Protrusio Acetabuli Marfan Syndrome in a subset |

Prenatal ultrasound diagnosing OI:
This prenatal ultrasound at 22 weeks’ gestation shows bowing of the femur (the crosshairs show the extremities of the femur).
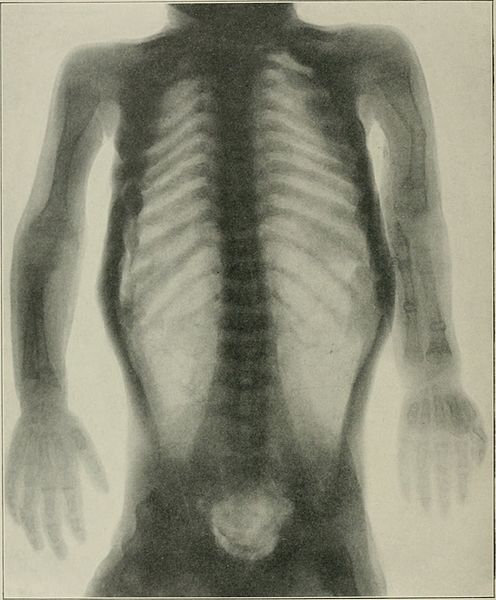
Radiograph showing OI:
periosteal dysplasia, almost complete absence of cortical bone, and numerous fractures

Chest radiograph showing long and narrow thorax (barrel-shaped chest) with anterior compression
Image: “Barrel-shaped chest” by the Department of Oral Medicine and Radiology, AB Shetty Memorial Institute of Dental Sciences, Nitte University, Mangalore 575018, India. License: CC BY 3.0.
Radiograph of the lower limbs showing bowing of the femur, with widening of the metaphases:
a 4-year-old boy with OI (type IV)

Radiograph showing a bowing tibia and fibula (saber shins):
a 4-year-old boy with OI (type IV)
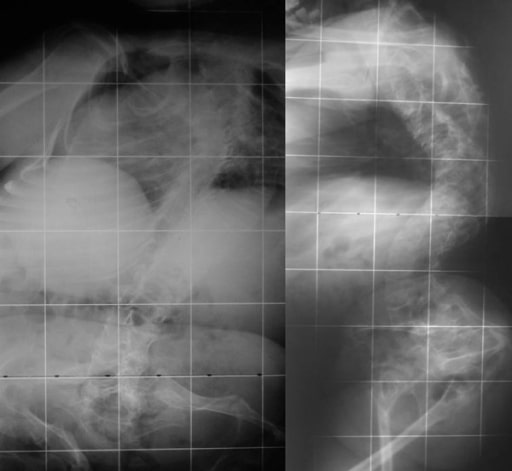
Biconcave deformities in the lower thoracic and lumbar vertebrae in a 15-year-old patient with OI (“codfish” vertebrae)
Image: “Osteogenesis imperfecta” by the 1st Department of Orthopaedic Surgery, School of Medicine, University of Athens, “Attikon” Hospital, Rimini 1 Haidari 12462, Athens, Greece. License: CC BY 2.0.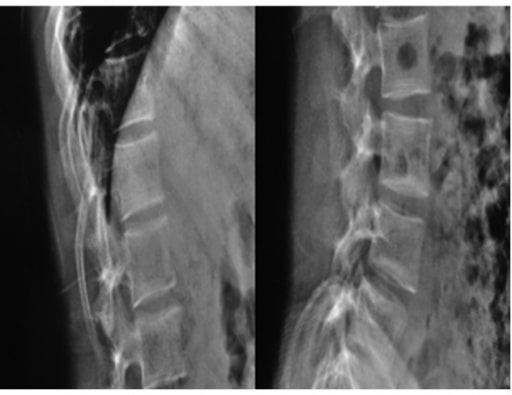
Radiographs of a 19-year-old woman with OI: Fragile bones, short trunk, severe kyphoscoliosis, and platyspondyly are noticed.
Image: “Biconcavity deformities” by the Department of Endocrine and Metabolic Diseases, Qilu Hospital, Shandong University, Jinan, Shandong 250012, P.R. China. License: CC BY 3.0.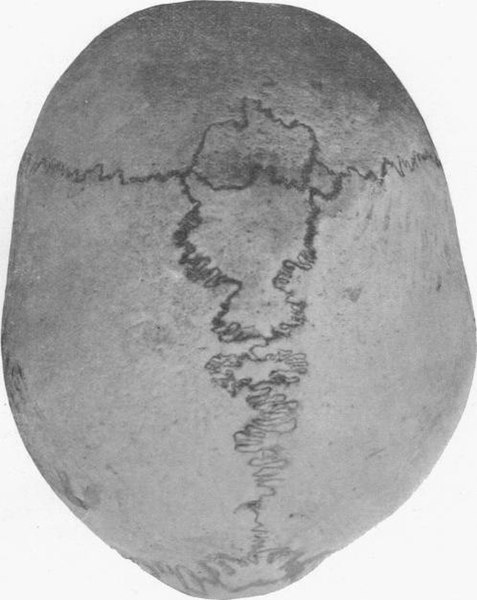
Human skull with wormian bones in a 21-year-old man
Image: “Wormian bones” by E. Barclay-Smith. License: Public domain.Não há cura definitiva para a OI.