Playlist
Show Playlist
Hide Playlist
Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)


-
Slides RegulationADHandSIADH RenalPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
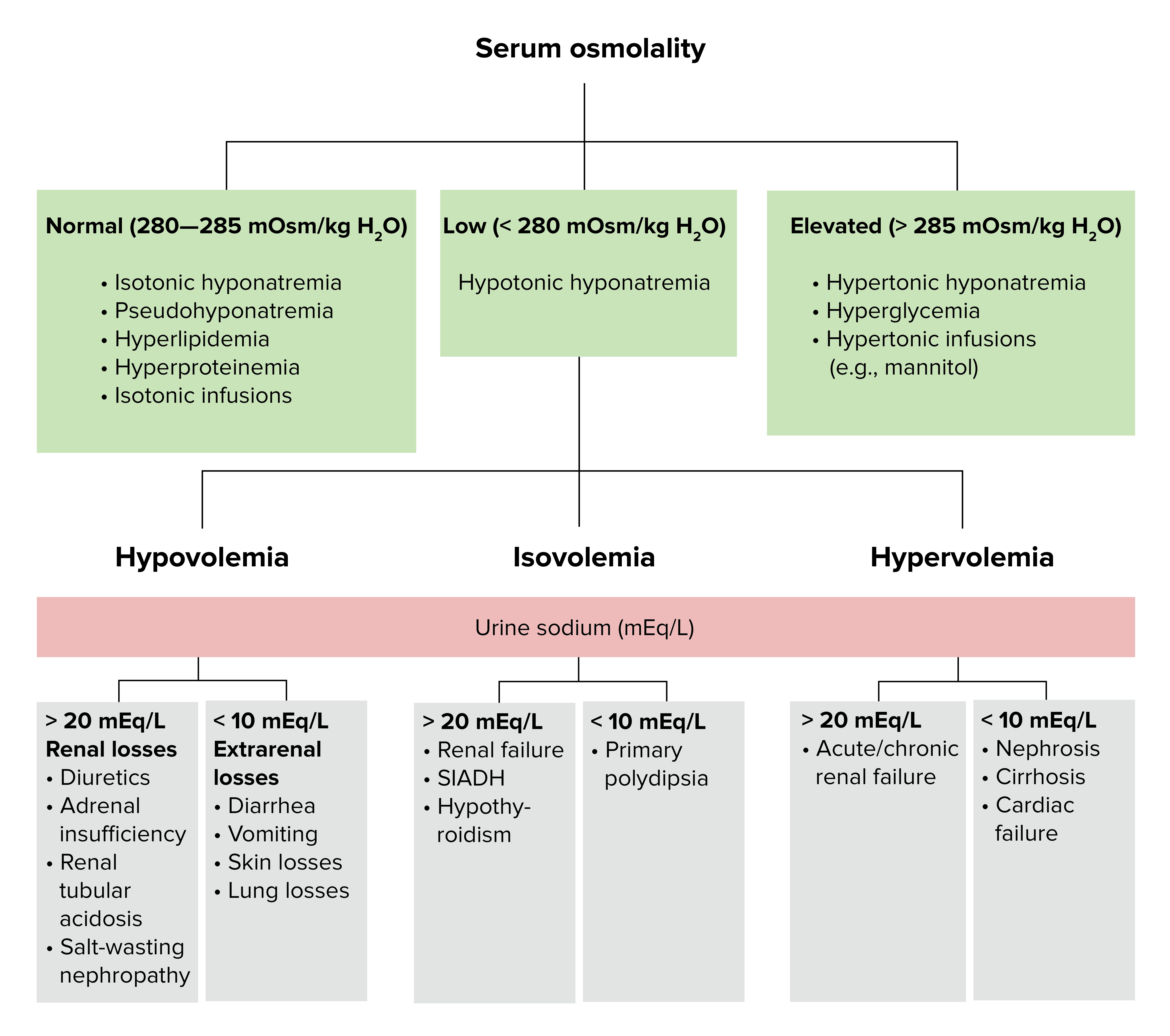
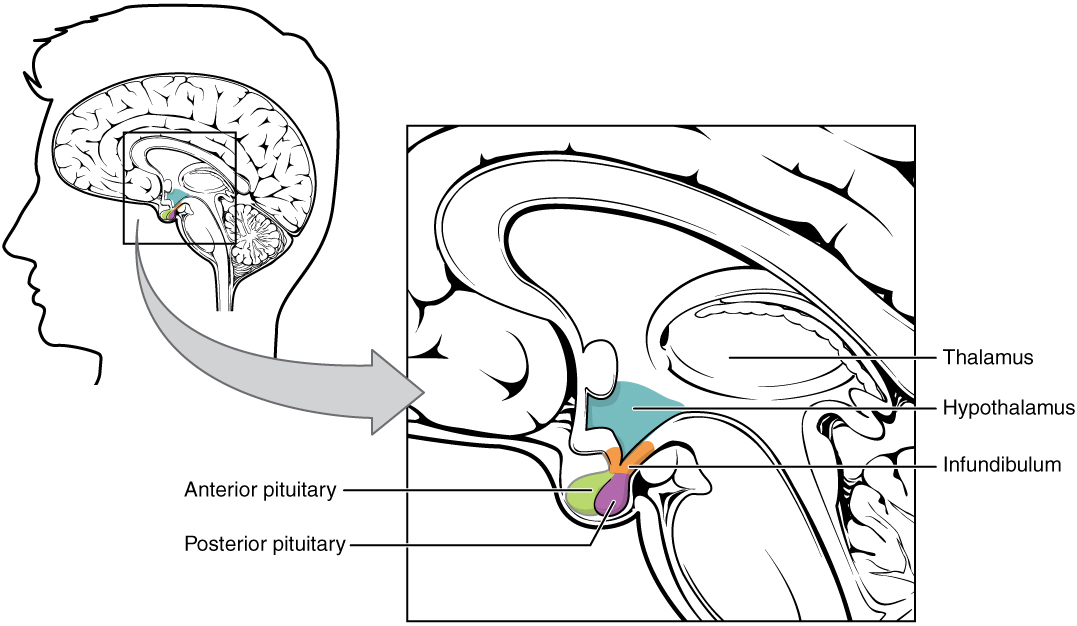
00:01 Let's going to SIADH. 00:03 SIADH, well, think about what is occurring here. 00:07 ADH once down to the collecting duct in excess and you are going to remove more, more, more free water. 00:14 As more free water is being produced or should I say free water is being reabsorbed, your plasma osmolarity will decrease at crazy. 00:22 What is the state of my urine? Look at the statement here. 00:25 What is this state of my urine? Hyperosmotic urine. 00:30 Urine remember I told you whenever you deal with osmolarity, always pay attention to the adjective. 00:36 Is it my urine compartment or is it my plasma compartment? From here too much ADH. 00:42 Circulating levels of ADH abnormally high. 00:48 How may this occur? Pay attention here now. 00:51 Head injury. From henceforth, head injury, do not think that you have destroyed the posterior pituitary resulting in lack of ADH. 01:03 Many students do that and they get everything wrong either in clinics and make a fool of themselves or in the boards and get the questions wrong. 01:12 So from henceforth, when you have a head injury, it can be rather unpredictable. 01:17 So what do you do? You base your question on the labs that are given. 01:22 What does that mean? If there is head injury and you find your plasma osmolarity. 01:27 Listen. If you had head injury and you find your plasma osmolarity really low and you find your urine osmolarity really high. 01:37 What is your patient suffering from? Release of too much ADH from the posterior pituitary. 01:44 What if we do the opposite? Now, I'm gonna thrown in the mix here, what if you find on a lab that your urine osmolarity is really low and your plasma osmolarity is really high? What is your diagnosis there? Central diabetes insipidus. Are you seeing this now? So be careful with head injury. 02:02 Do not always think that you exhaust all of your ADH, in fact you might release too much. 02:07 Where else could ADH come from? Lung tumor. 02:10 Which one? Small cell or squamous cell? Good. Small cell, perineoplasic. 02:17 ADH secreted autonomously, without an osmotic stimulus that could also occur. 02:23 So there is no osmoreceptor that is telling the ADH or posterior pituitary to release from the hypothalamus, but you are autonomously releasing it. 02:33 ADH is secreted when it is not needed. 02:35 So, generally speaking, important clinical situation is head injury and perhaps your small cell lung cancer and the fact that you might have autonomous secretion. 02:46 The level of ADH increase reabsorption of water from the distal tubule and CD, collecting duct. 02:54 You have hyperosmotic, urine. Stop. Hypoosmolar, plasma. 03:00 Clear. Two compartments for osmolarity always. 03:04 Keep those compartments separate. 03:07 Keep them organized so that you have proper differentials. 03:10 Hypoosmolar plasma inhibits the secretion of ADH. 03:15 It should. Listen. Hypo, normal individual. Let me give you an example. 03:21 Drinking too much water right now, all right, drinking too much water. 03:23 What is your plasma osmolarity? Decrease. 03:25 What should you do normally? Suppress my ADH. 03:28 But what if it doesn't? Then we have SIADH. 03:32 The feedback inhibition in SIADH, Syndrome of Inappropriate Antidiuretic Hormone, does not occur because ADH secretion is now autonomous. 03:42 How does this occur? Well, I gave you a prime example. 03:44 Head injury maybe a small cell lung cancer so on and so forth. 03:48 Now, what about management? In discussing treatment the first thing we need to consider is the patient's hyponatremia, and speed of correction. 03:59 It must be corrected slowly and if care's not taken during this process there's a real and significant risks for a central pontine demyelination. 04:06 Which results in permanent neurologic deficits. 04:09 The first-line therapy is generally considered to be fluid restriction. 04:13 Even without any additional intervention, fluid restriction alone can cause a rapid correction of sodium levels. 04:19 So careful monitoring of patient is very necessary. 04:22 Drugs like demeclocycline used to be first-line treatment for these patients. 04:25 But have since fallen out of favor in the EU and US. 04:28 Currently, the most widely accepted pharmacological agents are the Vaptans. 04:33 These drugs act as vasopressin-receptor antagonists that are generally only recommended if sodium levels don't normalize after 24-48 hours of fluid restriction. 04:42 So we have demaclocycline inhibits ADH action on the renal principal cell. 04:47 There is something that may behave like this on purpose. 04:52 The other big one would be something like lithium. 04:55 Lithium and demeclocycline actually induces nephrogenic diabetes insipidus. 05:03 So, let's step back here and make you understand what's happening. 05:07 SIADH is your primary pathology and this is how the questions and the stems and the things that are boarded may confuse you if you are not paying attention, you are going to choose the wrong thing. 05:20 Please, just let me walk you through this. 05:23 Your patient initially is coming with SIADH, you know that because of the labs that they have been giving you. 05:30 An increase in urine osmolarity, a decrease in plasma osmolarity. Fantastic. 05:33 You know your patient has small cell lung cancer most likely chest x-ray, next step of management and you try to look for that cancer, small cell lung cancer, there might be perineoplastic releasing your ADH. 05:46 Okay, fantastic. Now, with all that ADH being secreted into circulation, it has excess activity on your collecting duct. Excess activity on your collecting duct Would you tell me a step of management in which you are introducing a "disease" to deal with SIADH? Well, if ADH works on the principal cell, why not give a drug that is going to impair the action of the principal cell? Why not give a drug that actually kind of knocks out the ADH receptors? What are those receptors? V2 receptors on the kidney. Amazing. 06:26 So, here, you are going to induce, what does nephrogenic mean? The V2 receptors aren't working. 06:33 You're going to induce nephrogenic diabetes insipidus in a patient with SIADH. 06:37 Lithium could be a little interesting. 06:39 With lithium, yes, it may then cause nephrogenic diabetes insipidus. 06:43 Now, is that something that you want to use in a patient with SIADH, or just keep that in mind because you want to keep as many angles as possible so that you are open to possible questions coming at you in any direction. 06:59 My job here is to give you as many angles as possible. 07:01 At some point, where I will talk to you about lithium is going to be how you have a bipolar patient taking lithium. 07:10 Therefore, resulting in nephrogenic diabetes insipidus. 07:13 Not so much treatment for SIADH. 07:16 Keep that clear. Make sure you review this. 07:18 I've given you a bunch of information here that could be rather confusing, lot of terminology, but understand the topic at hand and deal with management and you will be in good shape.
About the Lecture
The lecture Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) by Carlo Raj, MD is from the course SIADH.
Included Quiz Questions
Which of the following is required in order to diagnose the syndrome of inappropriate ADH secretion after a head injury?
- Plasma osmolality must be very low, and urine osmolality must be very high.
- Plasma osmolality must be very high, and urine osmolality must be very low.
- Plasma osmolality and urine osmolality must be very high.
- Plasma osmolality and urine osmolality must be very low.
- Plasma osmolality and urine osmolality must be normal.
Which of the following statements is incorrect regarding SIADH?
- Plasma ADH concentration is low.
- Urine osmolality is high.
- Plasma ADH concentration is high.
- Plasma osmolality is low.
- It is a paraneoplastic syndrome associated with small cell lung cancer.
Which of the following conditions is induced by the administration of demeclocycline?
- Nephrogenic diabetes insipidus
- Central diabetes insipidus
- Nephrogenic diabetes mellitus
- Autoimmune diabetes mellitus
- Inappropriate secretion of antidiuretic hormone.
Author of lecture Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
