Playlist
Show Playlist
Hide Playlist
Regulation of ADH: Significance of Clearance of Water


-
Slides RegulationADHandSIADH RenalPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
00:01 Significance of clearance of water. So tell me about water. Water, where? In the nephron okay. There are two types of water and by that we mean, it could be either free or it could be obligated, right. What does obligated mean to you? It is bound to electrolytes. In the thick ascending limb, are you there, what are you doing? We are moving the electrolytes. What are they? Sodium, potassium, 2 chloride. Thus in your nephron, what are you left with? You are left with free water. Let us now take one step further and we'll call this clearance of water. 00:46 Clearance can be zero. It could be positive or it could be negative. Before we move on, can you please tell me the concept of clearance? Clearance means what you are actually evacuating from the body. What is your urinating? What is your clearing? Remember all the terminologies that we did earlier, we have filtration, then at the PCT you can modify it, you can reabsorb or you can secrete and then finally you get clearance. So it could be either zero or it could be positive or it could be negative. What does that mean? It is important that you understand this clinically. The explanation of these values are the following. If the clearance of water is zero, what does that mean to you? It means that the clearance of water is zero when no solute-free water is excreted. What does that mean? That means that what you are here releasing is going to be what is called the isosthenuria. In other words, this is isoosmotic. What this means is it is obligated water. So it is isotonic. There is no solute-free. 01:52 So that means it is bound with sodium making it what? Isoosmotic, with plasma. You call this isosthenuria. Interesting. Last time we talked about isosthenuria and we will talk about this again. This is a big deal. Isosthenuria represents the fact that well let us say that you had urinary tract infection. I bring that up quite a bit because it is an excellent example to really highlight and demonstrate a lot of key issues. So if you have the ascending infection come all the way to the kidney, polynephritis and at some point that E. colis in my pelvis, there it is, then it might cause a little bit of destruction or lot of destruction. 02:40 It might have necrosis. Where are you in the kidney? You're in the papilla. What is in the papilla? What part of the nephron? How about the medullary loop of Henle? Say the loop of Henle, the medulla and it's responsible for doing what? Creating hypertonic urine and if you have something called renal papillary necrosis secondary to an ascending E. coli type of urinary tract infection, then, unfortunately, you won't be able to properly form hypertonic urine and you might have isothenuria. So the fact that you have isothenuria in terms of clearance of water, it'd be zero. But in terms of pathology and urinary tract infection, it could be a problem. Is that clear? Example here, treatment with a loop diuretic. So if you have a loop diuretic, what is it going to do? You are going to block off the sodium-potassium- 2 chloride in the thick ascending limb and all of that urination isn’t this the most potent diuretic? Of course, it is. All the urination is taking place subsequently taking this drug, what kind of water? Clearance of water is zero. Mean to say that it is not solute-free. It is bound to sodium. Clearance. Let us talk about further descriptions. 04:04 Clearance is zero. No free water is generated. NaCl reabsorption is inhibited by? Well maybe something like your loop. If free water is not generated, it cannot be excreted, can it? The ability to dilute the urine during water drinking is impaired, why? Or you can’t dilute the urine because of sodium-potassium- 2 chloride might be then impaired. The ability to concentrate the urine during water deprivation is impaired. It is all dealing with something like your clearance and you are giving your loop diuretic. Interferes with generation of corticopapillary osmotic gradient, understand what this is. Cortico, that's your Bowman space, PCT. I want you to go into the papilla, where are you now? In the medulla. Is that clear? So therefore if you have a loop diuretic as your prototype here and you have impairment of sodium-potassium- 2 chloride, what have you done? You have impaired the corticopapillary osmotic gradient. Therefore, what is your clearance of water here zip? You are not producing any free water.
About the Lecture
The lecture Regulation of ADH: Significance of Clearance of Water by Carlo Raj, MD is from the course SIADH.
Included Quiz Questions
Under normal circumstances, at what plasma osmolality would you expect minimum levels of ADH?
- 275 mOsm/L
- 285 mOsm/L
- 295 mOsm/L
- 320 mOsm/L
- 300 mOsm/L
Which of the following changes would not be seen in a patient with severe hypovolemia with more than 10% fluid loss?
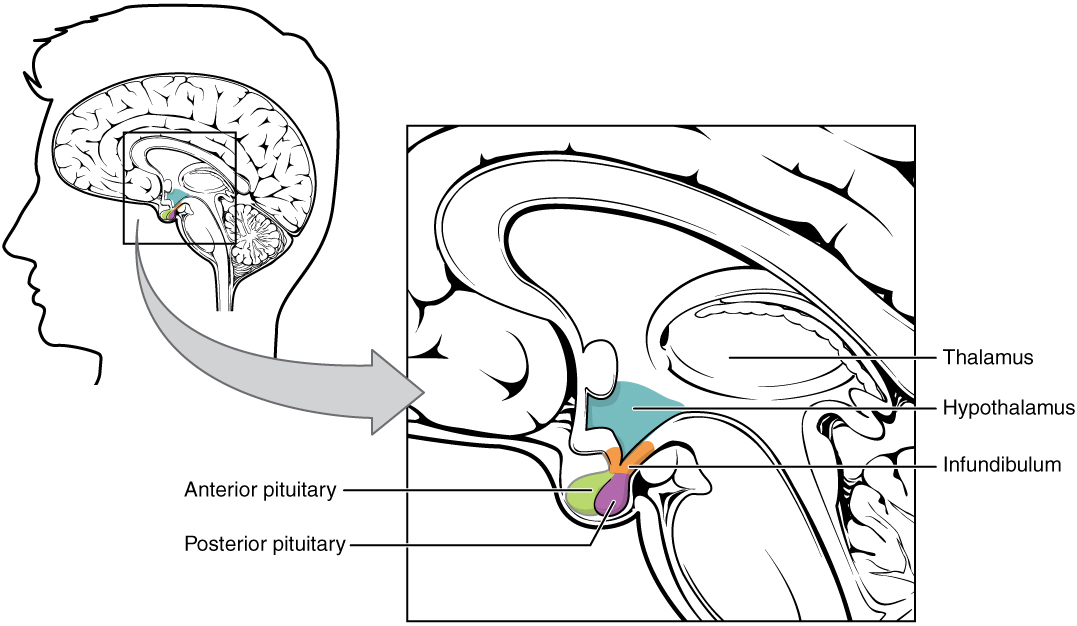
- An increase in the release of ADH from the anterior pituitary gland.
- An increase in the release of ADH from the posterior pituitary gland.
- Elevated plasma ADH level.
- Plasma angiotensin II concentration will increase.
- Activation of hypothalamic osmoreceptors.
Which of the following is not associated with isosthenuria?
- Increase in the ADH activity.
- Loop diuretics
- Urine is isotonic to plasma.
- Clearance of free water to zero.
If the clearance of free water is positive, which of the following must be true?
- Free water must be generated in the thick ascending limb.
- Urine must be hypertonic compared to that of plasma.
- More sodium must be reabsorbed.
- The countercurrent mechanism must be impaired.
- The diluting ability of the kidney must be impaired.
Which of the following statements is incorrect regarding hypertonic urine?
- It represents positive free water clearance.
- It represents negative free water clearance.
- It may be induced by severe hypovolemia.
- It may be induced by water deprivation.
- Urine osmolality is greater than plasma osmolality.
Author of lecture Regulation of ADH: Significance of Clearance of Water

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
