Playlist
Show Playlist
Hide Playlist
Regulation of ADH: Response to Water Deprivation


-
Slides RegulationADHandSIADH RenalPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
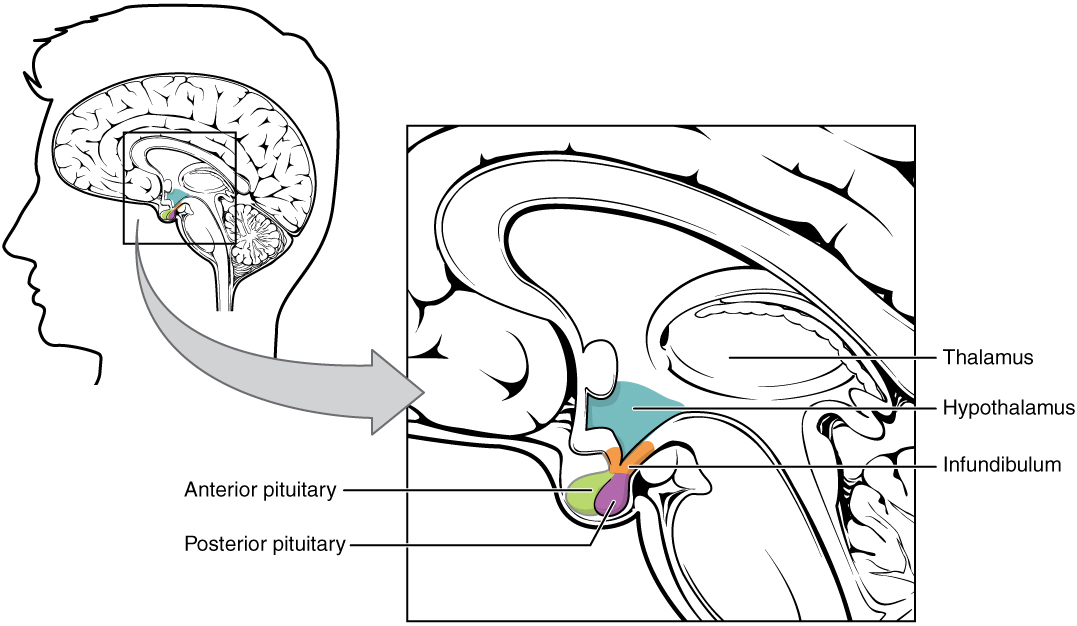
00:01 We are into a topic where students tend to have once again, problems with organization, but likely have done the entire time the more organized you are with your thoughts, the more methodically you can go through the material and the more number of times you do this, then it becomes part of your reflex and this brings us to the concentration of urine. And with this lecture series, we will be getting into issues of ADH either, too much or too little. At first, let us say that you have a patient that is deprived of water. The best thing to do before you go through all of these chronological order, you want to pay attention or predict as to what you can expect in your patient. Once you have done that, then you take a look at the chronology and all of it will make sense. You deprive your patient of water. 00:58 What does that mean to you? It means that your plasma osmolarity is going to increase, doesn't it? Once your plasma osmolarity increases, then the osmoreceptors by the hypothalamus will be triggered and you will be releasing your ADH. That ADH then runs down to the collecting duct that works to then insert these aquaporins via V2 receptors so that you can reabsorb that water, so that you can bring the plasma osmolarity back down to normal, right? So in essence, it is exactly what this illustration is showing you. Deprivation of water, increased plasma osmolarity. What happens next? Operative word, stimulation of your osmoreceptors. Next, you increase ADH. That ADH will then run down to the collecting duct, they'll work through V2 receptors. It will then insert the aquaporins so that you reabsorb water purely. 01:56 As you do so, it then causes the urine osmolarity to do what? Increase, good. And by removing the water and putting into the plasma, it is bringing the plasma osmolarity back to normal. Response to water drinking. This is the opposite scenario so even though the graph might look similar, the starting event, completely the opposite of what we just discussed. Here let us say that you are drinking water. Then what happens to your plasma osmolarity? Almost immediately, it drops a little bit. Now your plasma osmolarity is low, so, therefore, tell me about those osmoreceptors, they are not going to respond because there is no osmolarity to attend to. So, therefore, what happens to ADH release? It is suppressed. If there is no ADH, then as far as your urine is concerned, you tell me is it dilute or concentrated? If the ADH isn’t working, then the fluid within the collecting duct is then going to be in fact diluted urine. So, therefore, your urine osmolarity would be? Good, decreased. Now if you are not going to then reabsorb that water, then you can expect your plasma osmolarity to come back up toward normal. This is, in essence, the overall mechanics of ADH in response to plasma osmolarity. Now, ADH has three major actions in the renal tubule. This we have talked about plenty. On the principal cells, in addition to aldosterone, it has the ability through V2 receptors and putting those aquaporins so that you can then bring out the water. But take a look at this. Remember the sodium-potassium- 2 chloride, where are you? The sodium-potassium- 2 chloride cotransporter it is located on the thick ascending limb and what does that have to do with ADH, Dr. Raj? Well, a lot actually. Remember those diseases called Bartter and Gitelman. You are bringing them up again? Yes, I am. And the reason that I am bringing up now specifically which one of these diseases have we discussed the results in dysfunction of that sodium-potassium-2 chloride cotransporter. 04:18 Bartter and so therefore if you knock out this symport or cotransporter, you have lost ability to do what? To properly concentrate. Do you remember that? If you don't properly concentrate, then please understand you have also lost ability to properly dilute. If you don't properly dilute, where is your diluting segment? Going up the thick ascending limb and really moving up towards the distal convoluted tubule. So that is your diluting segment, if you can’t properly concentrate, you sure as heck can't properly dilute as far as its ability way down in the collecting duct for providing an environment for ADH to work properly may then be impeded. 05:03 And pretty much saw that both with the diluting ability in both Gitelman and Bartter if you remember correctly. But here understand that symport is absolutely required for proper functioning of the ADH later on down in the collecting duct. What else ADH do? Now this is important. Many students end up forgetting about this. Last time we have even talked about urea. It was rather insignificant. Alright. So no one likes to feel insignificant. That is for sure. Here urea with the help of ADH, in the medullary collecting duct, where are you? Way down deep, in the kidney, medullary collecting duct. ADH sure it brings up water, but what do you know about water? How do you move water? Osmosis. 05:55 Has to be. There is no way that you could move water with that osmosis in the body. 05:59 Do you understand that? So tell me as to what kind of gradient this is? It is moving from low solute concentration to high solute concentration, isn't it? What is this solute that water is following in the collecting duct? The urea. So ADH is the third and final function really to assist in reabsorption of water is going to be the fact that it actually places urea into the interstitium thus creating an osmotic gradient to then reabsorb the water. 1, 2 and 3, three major actions of ADH. Beautiful table here for us to truly understand.
About the Lecture
The lecture Regulation of ADH: Response to Water Deprivation by Carlo Raj, MD is from the course SIADH.
Included Quiz Questions
Which of the following is true regarding the changes that occur in dehydration?
- Increased activation of osmoreceptors in the anterior hypothalamus.
- Decreased activation of osmoreceptors in the anterior hypothalamus.
- Decreased plasma osmolarity.
- Increased activation of osmoreceptors in the anterior pituitary gland.
- Decreased activation of V2 receptors in the distal tubules.
Which of the following would increase in response to hydration?
- Urine volume
- Plasma osmolarity
- ADH release
- Insertion of aquaporins.
- Urine osmolarity
Which of the following substances acquires more permeability due to ADH activity?
- Urea
- Potassium
- Calcium
- Sodium
- Chloride
Which of the following is false regarding the actions of the antidiuretic hormone?
- It increases the permeability of urea in the outer medullary cortical duct.
- It increases the water permeability of the principal cells in the distal convoluted tubule.
- It increases the water permeability of the principal cells in the collecting duct.
- It increases the activity of Na-K-2Cl cotransporter in the thick ascending limb.
- It increases the permeability of urea in the inner medullary cortical duct.
Author of lecture Regulation of ADH: Response to Water Deprivation

Carlo Raj, MD
Customer reviews
3,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
1 |
really want to learn about SIADH, oh,,,, Dr. Raj. hard stop
Wonderful lecture explaining a difficult topic. I love Dr. Raj lectures! Looking forward to more Dr. Raj.
