Playlist
Show Playlist
Hide Playlist
Hepatitis: Pathology

-
Slides Hepatitis.pdf
-
Reference List Infectious Diseases.pdf
-
Download Lecture Overview
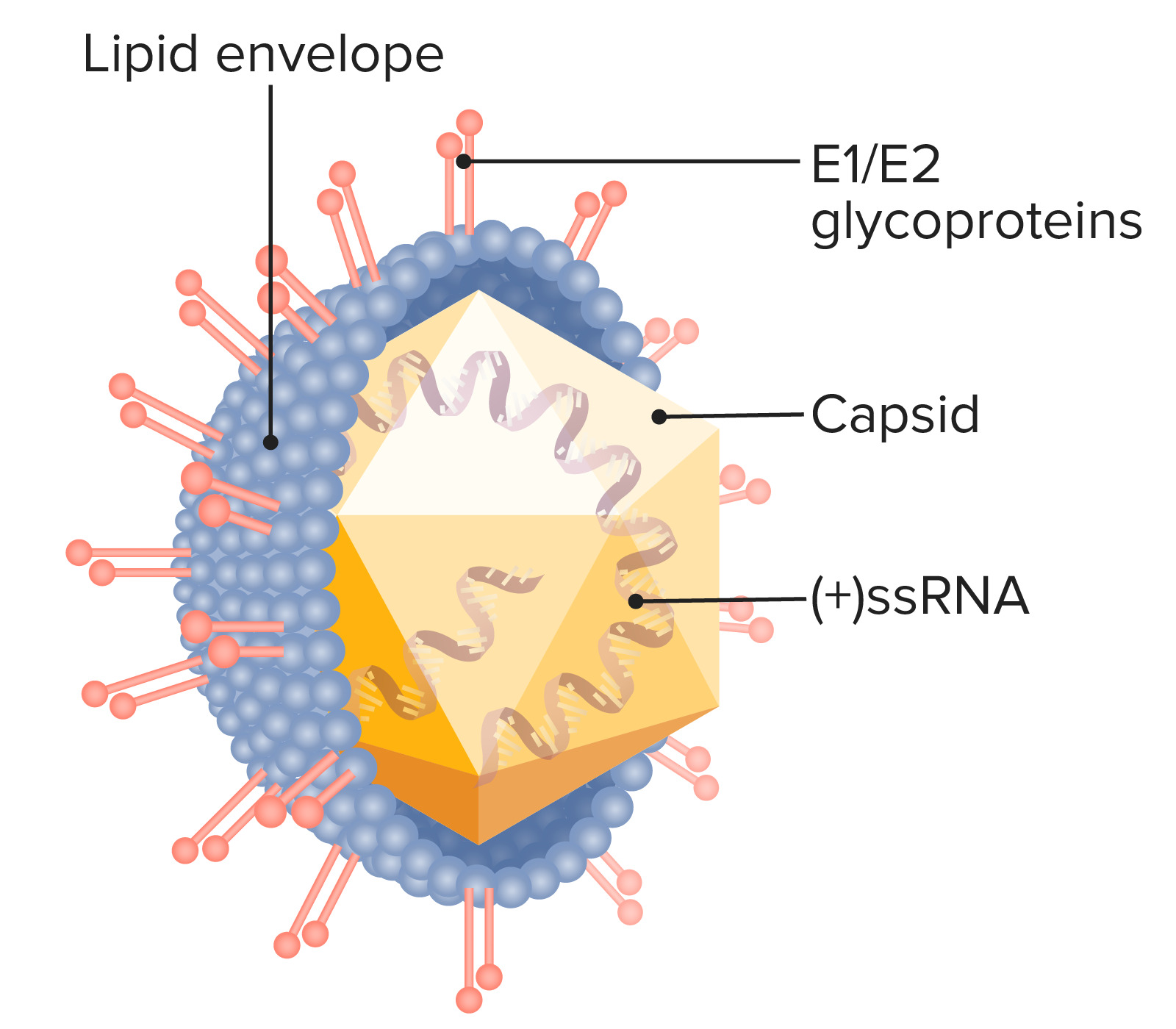
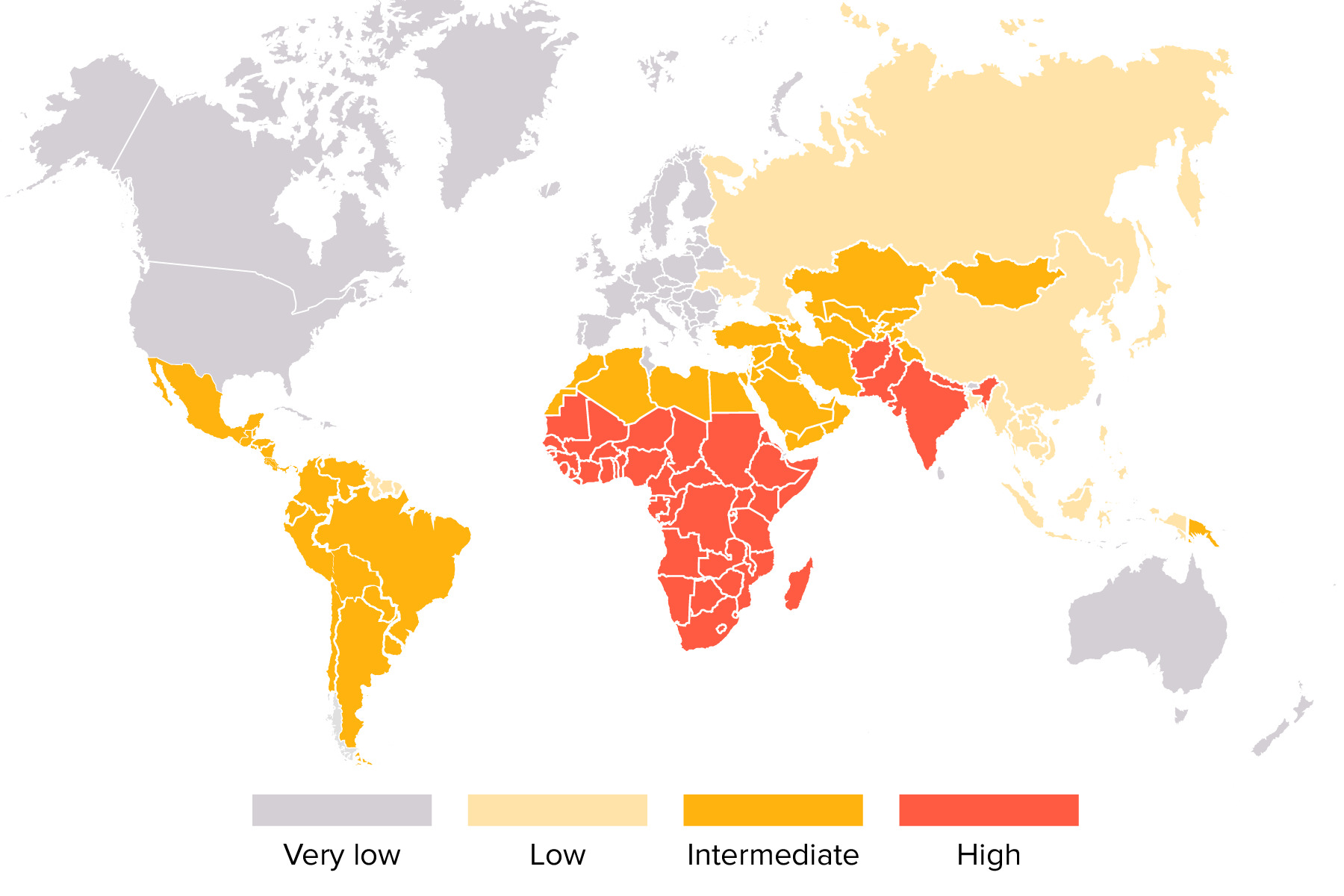
00:00 So let's about the pathogenesis of hepatitis A. The incubation period is from 15 to 50 days. 00:10 This virus is acid resistant and therefore gets through the stomach and is able to replicate in the lower intestine and that's the tract to the liver. Once it gets into the liver, it replicates in hepatocytes in the liver sinusoids and canaliculi and then goes back into the intestine and is excreted in the feces which is why it is contagious through the fecal-oral route. Now, it's our immune system that explains the pathogenesis. When we develop cell-mediated immunity, then our immune system actually causes the liver damage because our immune system attacks liver cells that contain the virus and these are CD8 cytolytic T cells and questionably natural killer cells. Once we develop humoral immunity, that keeps it from spreading to uninfected liver cells. 01:20 So it's a combination of cell-mediated for the destruction and humoral immunity for the protection. Hepatitis B virus has a generally longer incubation period, 1 to 6 months, and remember that the bloodstream is teaming with this virus and so therefore it is primarily transmitted by cutaneous and mucosal exposure to blood and bodily fluids containing the virus and look how many there are per mL of blood, 10⁸ to 10¹⁰ virions/mL. There also are variable amounts in semen, thus it can be a sexually transmitted disease. Saliva, cervical secretions and even tears. Interestingly, the virus is not found in urine, sweat, or stool so it's not transmitted by the fecal-oral route. Hepatitis B virus has a real high prevalence of perinatal transmission in underdeveloped countries and it can be transmitted both horizontally and vertically. In the low prevalence areas, it's primarily through sexual intercourse and IV drug use and once again it's the immune system that does the damage. Now, hepatitis B develops in more than 90% of newborns born to mothers with chronic hepatitis and remember these newborns have immature immune systems. So in infants, there is most likely the failure of the initial innate and adaptive immune response. So their immune system cannot kill the infected liver cells and so they often are left with a chronic infection. By the time you reach adulthood, you have immunocompetency and so therefore you're able to pluck out the cells that contain the virus. 1% with clinically apparent acute hepatitis have a less vigorous CD4 and CD8 T cell response and they can't clear it as well and it's still sufficient to injure the liver but it may lead to chronic hepatitis and is not really well known how a hepatitis B evades the immune system in some people. Hepatitis C has an incubation period of 4 to 20 weeks and IV drug users with contaminated needles explain the majority of infections in developed countries and there is mounting but still circumstantial evidence that the disease can be transmitted during sexual intercourse. A minority of infections are transmitted from healthcare workers. There used to be the concern that a surgeon would transmit it to his patient. That was in the day when we called hepatitis C non-A, non-B hepatitis because we hadn't isolated the virus yet but now that we are well aware of hepatitis C and take the appropriate precautions and test healthcare workers, we can largely prevent transmitting these infections from healthcare workers to patients. Interestingly, the acute infection in hepatitis C is usually asymptomatic 85% of the time; however, chronic infection also develops in 80 and even to 90% of the time. 05:26 The sad part about hepatitis C is that cirrhosis, severe scarring of the liver, occurs in up to 20% and you may remember that I mention this is sort of an unstable virus with antigenic variability and quasispecies. Well because of that, you can get repeated bouts of liver damage by one of the mutant strains that develops in your body. Hepatitis D is, remember, dependent upon hepatitis B and therefore in developed countries it is mostly transmitted by IV drug use but sexual and intrafamilial transmission also occur and as I mentioned it's a defective virus and its replication is dependent on the presence of hepatitis B virus. No hepatitis B, no hepatitis D. 06:25 Now, simultaneous hepatitis B and hepatitis D infection usually lead to an acute and self-limited hepatitis and chronic infection is much less common if there is simultaneous infection by both. 06:47 On the other hand, if a patient already has chronic hepatitis B and then develops hepatitis D superinfection, that leads to chronic hepatitis in 90% of individuals and unfortunately it leads to cirrhosis in 60 to 80%. Furthermore, fulminant hepatitis is 10x more common than just getting simultaneous hepatitis B and D infection. So it's bad if you superimpose hepatitis D on a patient who's already had hepatitis B. If they get the infection together, not so serious. 07:39 Hepatitis E virus has 4 genotypes. Type 1 is found mostly in the developing countries, type 2 Mexico and West Africa, type 3 also in developed countries and type 4 in China, Taiwan and Japan. Most cases we encounter are from Asia, Africa, the Middle East and Central America. 08:11 Like hepatitis A, this is fecally contaminated water in these endemic areas. It also can be transmitted by blood transfusion but person to person transmission is said to be uncommon. 08:30 Sexual and intrafamilial transmission also occur and this infection has an incubation period from 14 to 60 days. So after ingestion of the hepatitis E virus, it may be absorbed through the GI mucosa, goes to the portal circulation, gets into the liver where it can undergo amplification either there or in enterocytes. It interacts with hepatocyte receptors and enters the liver cell. 09:02 Then because it's a positive-sense RNA virus it acts, as I mentioned before, as its own messenger RNA goes to the ribosomes and off we go to the races with replication at the ribosome of new virus. All of these viruses are trying to make copies of themselves in the target cell and it produces a pathologic picture resembling both cholestatic and acute hepatitis.
About the Lecture
The lecture Hepatitis: Pathology by John Fisher, MD is from the course Gastrointestinal Infections.
Included Quiz Questions
Which type of hepatitis virus has the longest average incubation period?
- Hepatitis B
- Hepatitis C
- Hepatitis A
- Hepatitis D
- Hepatitis E
In hepatitis A infection, hepatocellular damage is mainly caused by which of the following mechanisms?
- Cell-mediated immunity
- Humoral immunity
- Viral toxin production
- Viral coding for cell apoptosis
- Direct cytopathic effect by the virus
What is infection rate of infants who are born to hepatitis B surface antigen-positive mothers and who do not receive hepatitis B immune globulin and hepatitis B vaccination at birth?
- Up to 90%
- Up to 50%
- Up to 65%
- Up to 20%
- Up to 5%
What is the most common transmission mode of hepatitis C in the United States?
- Intravenous drug use
- Blood transfusions
- Sexual intercourse
- Transplacental
- Fecal-oral transmission
Among the following patients with viral hepatitis, who is most likely to develop cirrhosis?
- A chronic hepatitis B patient who develops superinfection with the hepatitis D virus
- A person who contracts hepatitis B and hepatitis D simultaneously
- A person who contracts hepatitis A from contaminated water
- An adult who contracts hepatitis B from sexual transmission
- A person who contracts hepatitis E
Author of lecture Hepatitis: Pathology

John Fisher, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
