Playlist
Show Playlist
Hide Playlist
Gas Exchange – Lung Physiology




-
Slides 02 LungPhysiology Basic.pdf
-
Download Lecture Overview
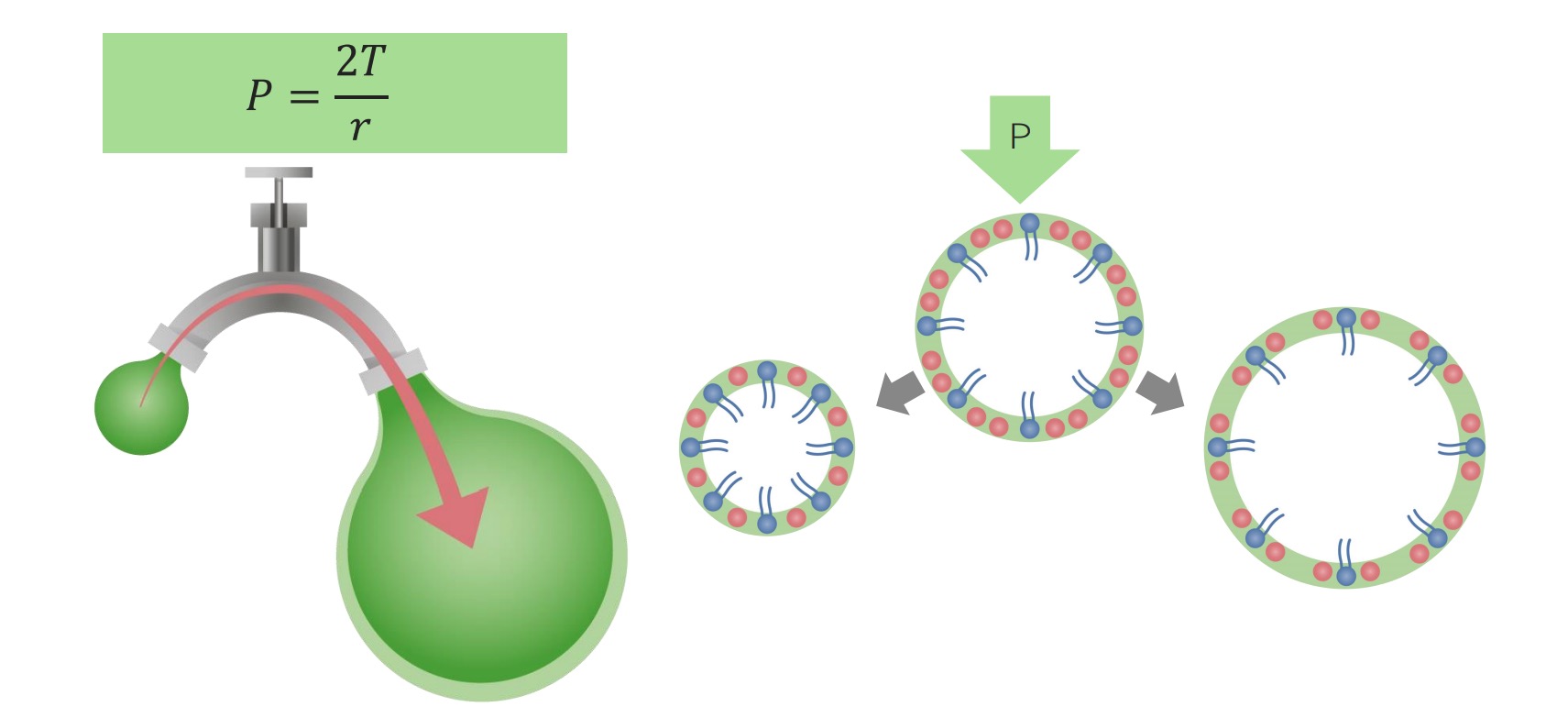
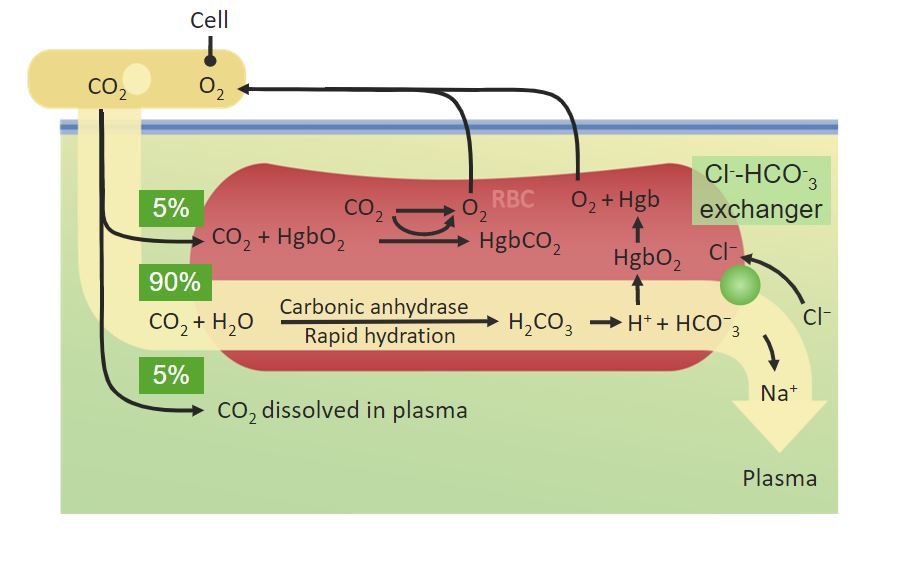
00:00 so that is ventilation. 00:05 The next step in the process is how does the gas delivered to the alveoli, the oxygen get from inside the alveoli into the blood vessel, the pulmonary capillary and how does the carbon dioxide being returned from the tissues, get out from the capillary and into the alveoli. 00:25 And this diagram shows the changes that normally occur in the normal function of the lung. 00:30 With deoxygenated blood coming in from the left hand side of the slide with relatively high concentration of carbon dioxide and on the right hand side of the slide you have got the oxygenated blood considerable two and a half times increase in the amount of oxygen present dissolved in the blood and a small decrease in the carbon dioxide but very important decrease. This occurs in the transit times as the blood crosses across the pulmonary capillary around the alveoli. How does this happen? Actually it is very simple, and it is not an active process. It just requires diffusion. So the high concentration of the oxygen in the alveoli allows the oxygen to diffuse into the blood vessel. The high concentration of the carbon dioxide in the blood vessel allows the carbon dioxide to diffuse out into the alveoli. This depends on the law called Fick’s Law. That defines the parameters that will allow efficient diffusion of these gases in and out of the alveoli. 01:32 And Fick’s law is one of those laws which actually is very obvious when you look at it. What it says is that the amount of gas that can transfer across a sheet of tissue in which case, in this case it's the alveoli membrane, is proportional to tissue area. 01:48 The bigger the tissue area the more the gas goes across, not surprisingly. Something called a diffusion constant which I will describe in a little while but essentially what that is, is how easy it is for particular gas in this case oxygen and carbon dioxide to move across that membrane and then is driven by the differences in the partial pressures of the gases. So if in, for example, you have a lot of high concentration of gas on one side of the membrane and low concentration on the other then that would drive diffusion across that membrane much more, if it is a high concentration and in a medium concentration on the other side. This can be drawn as this equation here. 02:28 There is another factor which is how thick the tissue there is. That again is fairly obvious if you have tissue which is this thick it is going to harder for oxygen to get in there to there. If it is very thin, it will be much easier. And in fact the alveolar membrane has as we described in the anatomy talk is incredibly thin. And it is thin to allow this diffusion process to be efficient. So the diffusion constant and that dictates how easily a specific gas can diffuse across any membrane and in this case the alveolar membrane. The diffusion constantly is proportional to the gas solubility. If the gas is very soluble, it would diffuse easily. This is why carbon dioxide diffuses better than oxygen because it is very soluble. 03:10 The other factor is inversely proportion to the square root of the molecular weight which means roughly speaking, the oxygen and carbon dioxide are about the same for that factor. 03:22 So as a consequence carbon dioxide and carbon monoxide diffuse more efficiently than oxygen. 03:28 Conversely nitrogen the other major gas component of the lung as well as the oxygen is not soluble and has very low water solubility, and so it diffuses very poorly. And nitrogen diffusion across the alveolar membrane into the blood only rarely occurs when you are breathing air under high pressure. And that occurs in divers and leads to the bends but is not going to happen in normal situations of atmospheric pressure. 03:56 So the alveolar membrane, as described in the anatomy talk, the alveolar membrane is very thin. It is consistent of the surfactant layer, the alveolar epithelium itself which is a very thin type-1 pneumocyte for the majority of the surface area of the alveolus. The interstitial space which again is minimal with a little bit of connective tissue with occasional fibroblast but not a significant amount of interstitial tissue. Then we have the capillary endothelium it's basement membrane and then there is the blood itself in the capillary, the liquid phase and then there is the red cell membrane and then finally the oxygen will get into the red cell itself. The thing about this is that gap between the oxygen molecule in the alveolus and the haemoglobin in the red cell is very small. That allows diffusion to occur very rapidly. Of course if that gap is increased and the two main diseases with that increase is pulmonary oedema where in fact the alveolar fill up with equivalent of water, displacing the oxygen further away from the alveolar membrane, or in pulmonary fibrosis where the interstitial space becomes expanded or considerably more connective tissue and so then the diffusion process becomes much poorer, much slower. 05:08 Now the other important thing about alveoli is the massive surface area, 75 Sqm depending on your size, roughly 50 to 100 mSq depending on whether you are small or big person. And that massive surface area provides a very large area for oxygen diffusion to occur a very rapid process and clearly that surface area would be reduced if you resect somebody’s lung. And it is also reduced if the alveoli is destroyed and merged to form larger units than the very small grape-like clusters that we have at the end of the terminal bronchioles. 05:41 And that occurs in emphysema, a disease related to smoking. 05:48 The business about the gradient of the gas concentrations to drive the diffusion process. 05:55 Well, if you look at the numbers mixed venous blood is the blood that is returning the gas concentration, returning in the pulmonary arterial circulation to the pulmonary capillaries. 06:08 You can see the values there. And then the alveolar concentration of the gas is and you can see the oxygen is considerably higher. The difference with carbon dioxide is much less. Of course carbon dioxide has a diffusion constant which allows it to be more rapidly diffused across the alveolar membrane than oxygen, so that is less of a problem. Now importantly by picking up oxygen, that gets into the blood, haemoglobin helps drive the process of oxygen being transferred across the alveolar membrane. Because it maintains this partial pressure difference between the alveolar oxygen content and the content dissolved in the blood. 06:52 The other thing that is very important for the diffusion to work efficiently is not only just the alveolar membrane have to be thin and the surface area large, but you have to have a lot of blood being delivered to the alveolar surface to allow the diffusion to occur. As described in anatomy lecture, if you look at the alveolar surface about 70% of it is covered in pulmonary capillaries, providing a very large surface for the gas exchange process to occur. Now these capillaries are under low pressure and the importantly they are highly distensible. That means they can increase in their volume but they cover the alveolus very easily. If you have an increasing cardiac output and this is what happens during exercise is that the stroke volume increases and the heart rate will increase, making the cardiac output increase. What actually happens with the transit across the pulmonary capillaries is not the speed by which blood crosses from the pulmonary arteries through the capillaries to the pulmonary veins increases, so it goes faster to make account of the increased cardiac output, but in fact what actually happens is that the transit time phase is relatively same but the amount of capillary volume that is crossing over the alveoli increases because they will distend. 08:18 So the transit time, this is how long it takes for blood red cell to go to from the pulmonary from one end of the alveolus to the other in the pulmonary capillary. And in fact that is about 0,75 seconds at rest but maximal oxygen uptake occurs within 0,25 seconds, so you only need 1/3rd of your transit time during rest to get the maximum benefit of oxygen uptake by the alveolus into the blood. During exercises I mentioned the transit time does not change hugely, but you do have that massive reserve of 0,5 seconds to increase the oxygen uptake during exercise if necessary.
About the Lecture
The lecture Gas Exchange – Lung Physiology by Jeremy Brown, PhD, MRCP(UK), MBBS is from the course Introduction to the Respiratory System.
Included Quiz Questions
What is the partial pressure of oxygen (PaO2) in deoxygenated blood?
- 40 mm Hg
- 45 mm Hg
- 50 mm Hg
- 100 mm Hg
- 140 mm Hg
What is the partial pressure of oxygen (PaO2) in oxygenated blood?
- 100 mm Hg
- 40 mm Hg
- 50 mm Hg
- 45 mm Hg
- 140 mm Hg
How much does the partial pressure of carbon dioxide (PaCO2) change after going through the pulmonary capillary bed?
- It decreases by 5 mm Hg.
- It increases by 40 mm Hg.
- It decreases by 45 mm Hg.
- It decreases by 100 mm Hg.
- PaCO2 does not change after going through the capillary bed.
What are the specific barriers that gaseous molecules must pass through by diffusion when moving from the alveolar airspace to the interior of a red blood cell?
- Six: the surfactant layer, the alveolar epithelium, the interstitial space, the capillary endothelium, blood in the capillary (liquid interface), and the erythrocyte membrane.
- Two: the alveolar membrane and fibrous tissue
- Three: the surfactant layer, alveolar epithelium and capillary endothelium
- Four: the surfactant layer, the alveolar epithelium, the interstitial space, and the capillary endothelium
- Eight. the surfactant layer, the alveolar epithelium, the interstitial space, the mesangial layer, the vessel wall, the capillary endothelium, blood in the capillary (liquid interface), and the erythrocyte membrane.
Author of lecture Gas Exchange – Lung Physiology

Jeremy Brown, PhD, MRCP(UK), MBBS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
