Playlist
Show Playlist
Hide Playlist
Ventricular Tachycardia: Torsade De Pointes




-
Slides Tachyarrhythmia VentricularTachycardia CardiovascularPathology.pdf
-
Download Lecture Overview
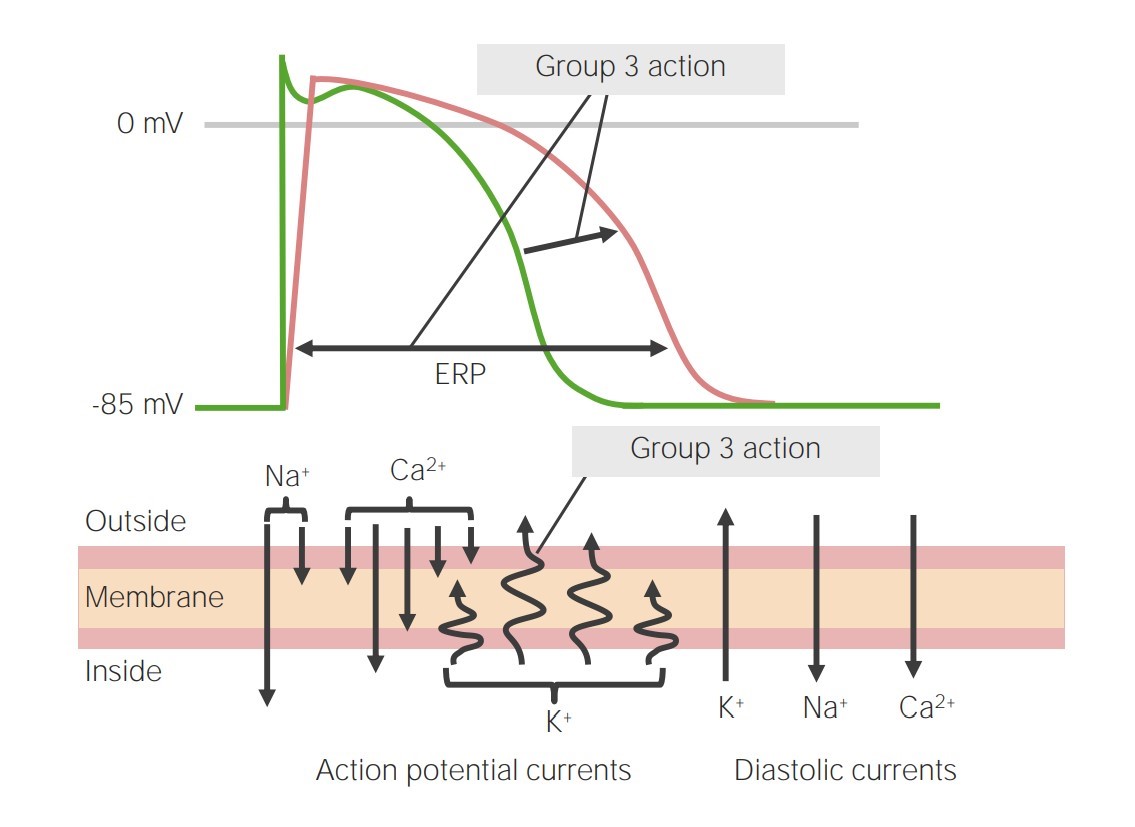
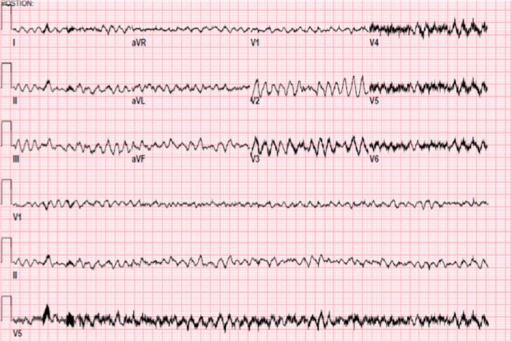
00:02 Now on this ECG, take a look at this. Twist, twist, twist, narrow point; twist, twist, twist, narrow point. What is the other name for this? It is called polymorphic ventricular tachycardia. Allow the name to speak to you. Polymorphic, various changes in shape of whom? The ventricular representation of your ECG is your QRS complex. 00:38 The most common type of polymorphic ventricular tachycardia that you will be responsible for is this one, it's called torsade de pointes. Now with torsade de pointes, what preceded this? What is the predisposing factor? Well the QT, which is all ventricular activity. Let me give you some important points. Pay attention. QT, all ventricular activity. Let's do QRS complex first. What does that mean to you? Ventricular depolarization. What does that mean to you? The ventricles are going to contract. Which action potentional are you bringing into play here? 01234, or 403, which one please? 01234, do that for me. It will make your life heck of a lot easier clinically. Please do that for me. With that QRS complex and let us say that you want to block it for whatever reason, you want to block it. What kind of drug might you be thinking? I want you to block that depolarization. A phase 0 blocker. What is that phase 0 in 01234 with mechanical top actual potential? Good. It is a voltage-gated sodium channel. What if you gave too much of that voltage-gated sodium channel class I type of antiarrhythmic? If you gave too much, then what may then happen? Prolong the QT. Let me give you another one. 02:01 Tell me about that T wave. I told you QT is what you are paying attention to. Tell me what T wave represents. Ventricular repolarization. Let us talk about that actual potential again. 02:15 01234, which phase of actual potential 01234 represents the T wave and ventricular depolarization? It is phase 3, isn't it? Think about that. Of course, it is. Repolarization, potassium efflux. I want you to block the potassium channel, a class III drug. Drug such as amiodarone, what may then happen? You prolong the T, means you prolong the QT. What do you know about 1 and 3? What do you know about class I and class III antiarrhythmics? Are you seeing as to how beautifully we are able to walk through the physio, the disease, and the management. 02:53 Adverse effects. Class I and class III may then cause long QT syndrome that you already know. Now you are putting it together and you're predisposed to this sucker, which is your torsade de pointes. Or you are born with this genetically and one you definitely want to you is romano-ward. Why did I say romano like that? It is because I need you to know the Romano has no deafness. Romano-ward is congenital long QT syndrome. Couldn't help it, born with it, but there's no deafness where you have another one where Lange-Nielsen is involved. 03:34 That is also congenital long QT syndrome and that is involved with deafness. There is a lot more going on here than meets the eye and you know that. You can't just look at this and be like, "That must be torsade de pointes, that was such a simple question." No such thing. There is history behind this and we walked through some important ones. Let us continue. 03:55 Some clinical findings that are associated with ventricular arrhythmias include hypomagnesemia, bradycardia and a prolonged QT interval acquired long QT syndrome which can lead to ventricular arrhythmias, including torsades de pointe is seen in hyperkalemia, hypomagnesemia and some commonly used medications. 04:13 Bradycardia. What does that mean? You are slowing down your heart rate. The more that you slow your heart rate, you are predisposed to what? Twisting. Also what about that QT? We already talked about drugs. Let us take a look at few of them. We have antidepressants, phenothiazines. 04:33 Quinidine, a sodium channel blocker. Procainamide, sodium channel blocker. Disopyramide, sodium channel blocker. Why am I bringing these up? Because I just told you, class I, by blocking the sodium channel, you might be doing what? Creating a long QT scenario. Floroquinolone antibiotics and antifungals. Here is some ABCs, antibiotics, antifungal, antipsychotics, antidepressants, at least, know some of those and antiarrhythmics. You actually have ABCD. 05:08 Obvious I don't know my alphabet, but you do the alphabet and you'll walk through anti, anti-A arrhythmia, B biotics, C well you might want to pronounce it being psychotic if that helps, D is going to be depressants. Anyhow work with C there a little bit. Can you do that for me? Thank you, appreciate it greatly. Let us move on. 05:31 Ventricular tachy. We have torsade de pointes. What happens, worse case scenario? Look at this. Decreased cardiac output, syncope and is scary. The ventricle is not working properly may lead into v.fib. You don't want this at all. Right, this is no joke. You try to control this ASAP. Worried about cardiac arrest and death. Next well corrected with electrolyte imbalance, which one? Which electrolyte are you focusing upon most importantly again? Magnesium, good. So if you are hypomagnesemic, think of seizures. Next setting of hemodynamic instability, what is your next step of management? Good. Electrical cardioversion. What does hemodynamic instability mean to you? The stress, dizziness, syncope, low blood pressure. Isoproteranol or dobutamine, what about these? Well, these could be used to maintain a tachy, utilized, so just may be. Just keep that in mind. A nonselective beta agonist, isoproteranol. 06:38 Or dobutamine is selective beta-1 agonist. Now we are going to worse case scenario. Tried everything you could, maybe wasn’t effective enough and your patient still goes into v.fib. Very very obscure type of QRS complexes. This is not ventricular tachycardia. Your patient is very much at risk for stand still. Torsade de pointes, patient unconscious, result in sudden cardiac death. So this is no joke.
About the Lecture
The lecture Ventricular Tachycardia: Torsade De Pointes by Carlo Raj, MD is from the course Arrhythmias: Basic Principles with Carlo Raj.
Included Quiz Questions
Which phase of the ventricular action potential is altered by class III antiarrhythmic, and may have an adverse effect of causing a prolonged QT interval?
- Phase 3 – potassium efflux
- Phase 1 – sodium efflux
- Phase 4 – potassium influx
- Phase 2 – calcium influx
- Phase 0 – sodium influx
Which of the following can prolong the QT interval and lead to potential ventricular arrhythmias and Torsade de Pointes?
- Class IA and class III antiarrhythmic drugs
- Hypercalcemia
- Hyperkalemia
- Hypermagnesemia
- Atrial fibrillation
Which of the following is associated with prolongation of the QT interval?
- Bradycardia
- Supraventricular tachycardia
- Wolff-Parkinson-White syndrome
- Sulfa antibiotics
- Hyperparathyroidism
Author of lecture Ventricular Tachycardia: Torsade De Pointes

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
