Playlist
Show Playlist
Hide Playlist
Hemothorax and Cardiac Injury

-
Slides ThoracicInjuries Surgery.pdf
-
Download Lecture Overview
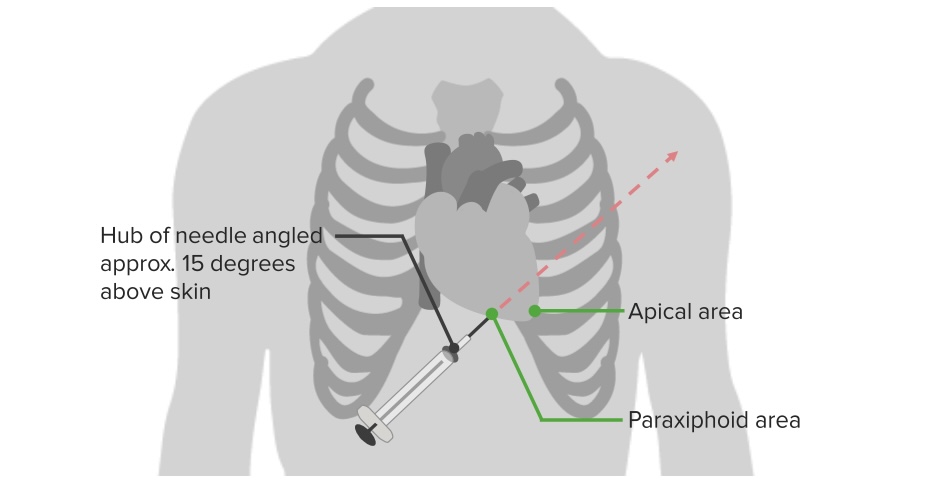
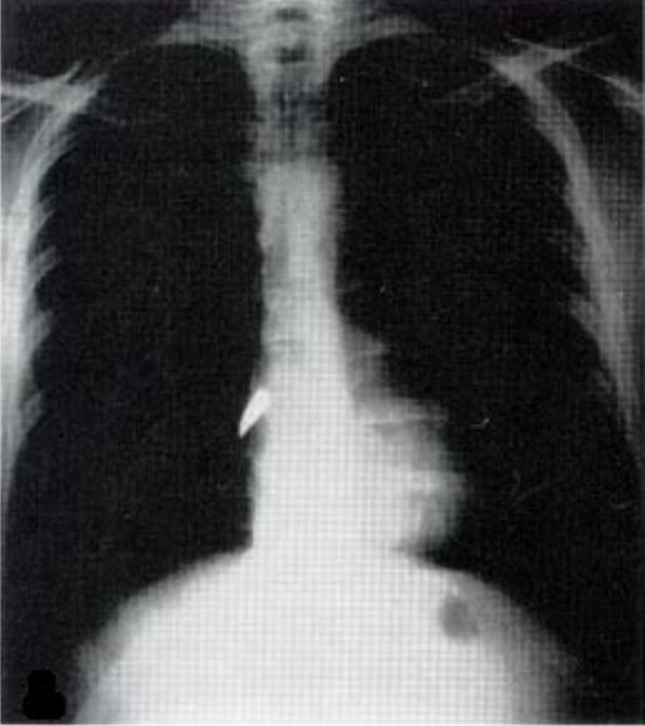
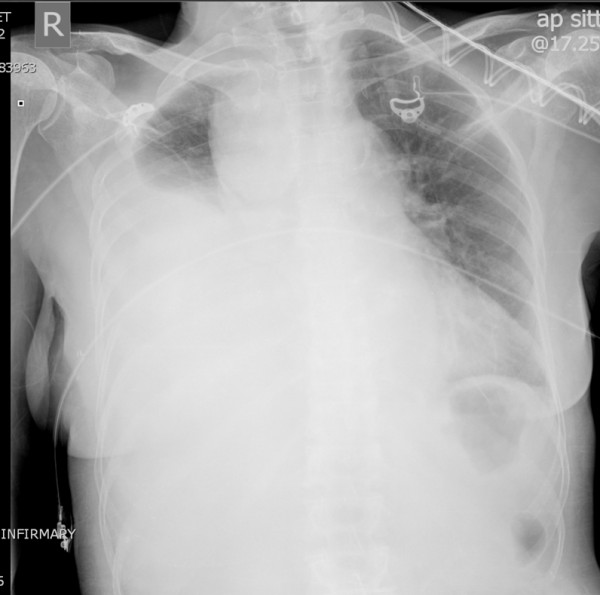
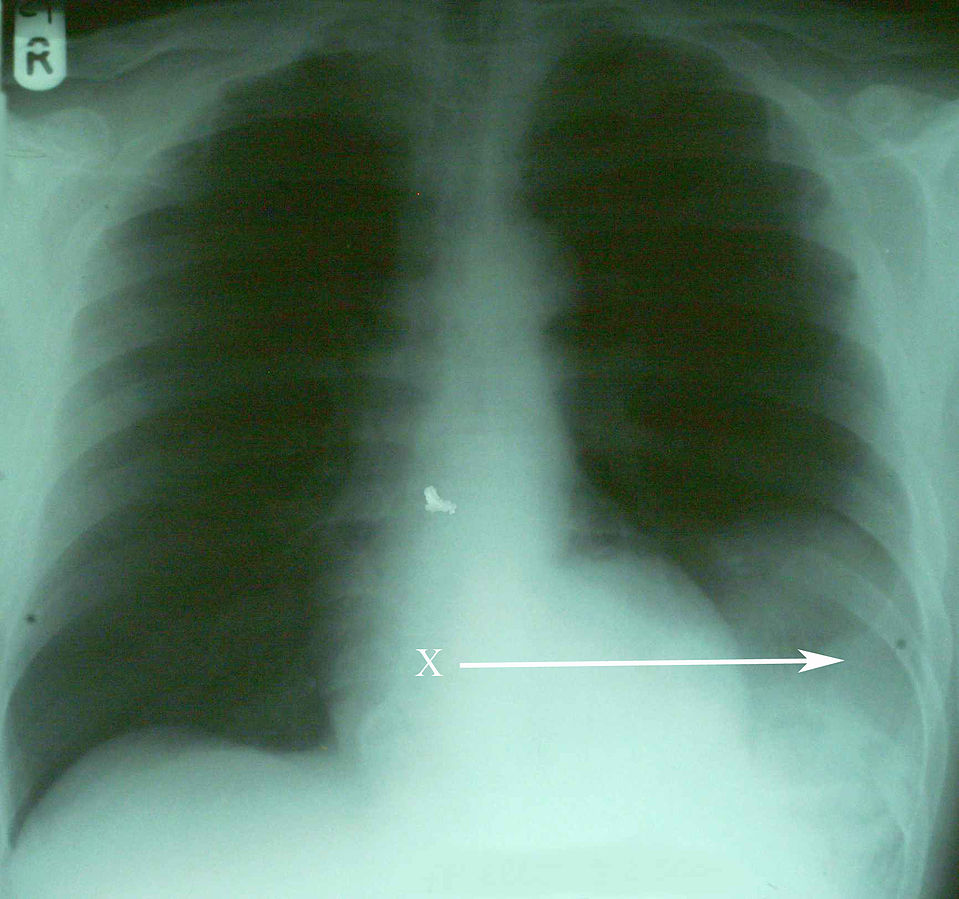
00:01 Now, let’s move on to a different topic, although it’s related, hemothorax. 00:06 Hemothorax on the initial x-ray is usually described as a complete white out. 00:11 Again, clinical context is very important. 00:14 If you’re in the intensive care unit and you have this similar chest x-ray, you may think that the patient actually had a large mucus plug. 00:21 But in a traumatic patient, this right side is completely whited out is considered hemothorax until proven otherwise. 00:29 The hemothorax needs drainage. 00:31 If you leave blood behind, you can imagine it would clot and it may lead to a retained hemothorax requiring additional surgery if not appropriately drained. 00:41 Let me pose a question to you. 00:43 Now that you’ve defined or diagnosed a hemothorax, what’s the next step in management? I’ll give you a second to think about this. 00:52 That’s right, chest tube. 00:53 Just like in pneumothorax and make sure that your chest tube is large bore and adequately drains all of the blood. 01:02 Next. 01:04 What if there’s greater than 1.5 liters or 1500 ccs of blood or continued high output from the chest tube that you placed for this hemothorax? What’s your next step in management? I’ll give you a second to think about this. 01:19 That’s right. 01:20 The patient needs a thoracotomy. 01:22 Whatever is bleeding is going at a pretty good rate and it’s unlikely to stop on its own. 01:27 If it were just small veins or small arteries that were bleeding from the chest wall itself, it should stop by now. 01:34 Therefore, the patient requires a thoracotomy. 01:39 Now, let’s return to our patient. 01:41 Remember that scary picture of the stab wound? What other injuries are you suspecting? Clearly, the patient can have any intrathoracic injury with a stab wound like this, not just the lung. 01:54 I’ll give you a second to think in your own mind. 01:56 What are the injuries are you suspecting? And then we’ll discuss some of them. 02:04 Let’s start by talking about cardiac injury and specifically, we want to mention cardiac tamponade and direct cardiac injury. 02:12 Let’s start with tamponade. 02:14 Here on this ultrasound image, the white arrow points to a large pericardial effusion. 02:21 Now, the clinical context is again very important. 02:25 Any traumatic situation particularly with stab wound, this is unlikely to be a chronic pericardial effusion. 02:31 It’s likely to be a bleed from a myocardial injury. 02:39 Now, do you remember the classic trilogy of symptoms associated with cardiac tamponade? I’ll give you a second to think about this. 02:49 That’s right. 02:49 This is called the Beck’s triad. 02:51 Beck’s triad, although classically described, is very difficult to diagnose particularly in the trauma bay but it includes jugular venous distention, distal heart sounds or often called muffled heart sounds due to the blood in the pericardial sac and because of decreased filling, hypotension. 03:10 Again, Beck’s triad: Jugular venous distention, muffled heart sounds, and hypotension. 03:18 Now, what’s the treatment? As you can see on this image, we have to do a pericardiocentesis. 03:24 If the pericardiocentesis, which is done in the subxiphoid space, shows blood the patient will likely need a sternotomy to fix the underlying injury. 03:34 Remember, this is in traumatic situation not in somebody who has a pericardial effusion chronically. 03:40 Some things to remember in terms of clinical pearls. 03:43 Our discussion has been about acute cardiac tamponade due to injury. 03:48 Patients with chronic cardiac pericardial effusions may not be developing signs of tamponade as they have had time to adjust. 03:58 Next, let’s move on to direct cardiac injury. 04:01 That blade could have stabbed the heart in and of itself. 04:04 And not only have caused the cardiac tamponade but likely a cardiac arrest in this situation. 04:10 In this image, you see a large laceration of the heart. 04:17 In the trauma bay if you were to have performed an ED thoracotomy to access the heart, you do quickly sutures to close the heart defect. 04:25 Unfortunately in these situations, it’s pretty difficult to bring the patient back. 04:30 Sometimes you can use staples as well to close. 04:32 These images demonstrate a very, very well-repaired, probably an elective setting.
About the Lecture
The lecture Hemothorax and Cardiac Injury by Kevin Pei, MD is from the course Surgery: Trauma. It contains the following chapters:
- Hemothorax
- Cardiac Injury
- Direct Cardiac Injury
Included Quiz Questions
What is the classic triad of symptoms associated with cardiac tamponade?
- Jugular vein distension, distant heart sounds, hypotension
- Jugular vein distension, 3rd heart sound, hypotension
- Jugular vein collapse, distant heart sounds, hypotension
- Jugular vein collapse, dull heart sounds, hypotension
- Jugular vein distension, S4 heart sound, hypertension
Pericardiocentesis is performed through which of the following areas of the body?
- Sub-xiphoid space
- 3rd intercostal space
- 4th intercostal space
- Pleural space
- Pericardial space
Author of lecture Hemothorax and Cardiac Injury

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
