Playlist
Show Playlist
Hide Playlist
Thrombolytics and Procoagulants

-
Slides Thrombolytics Procoagulants.pdf
-
Reference List Pharmacology.pdf
-
Download Lecture Overview
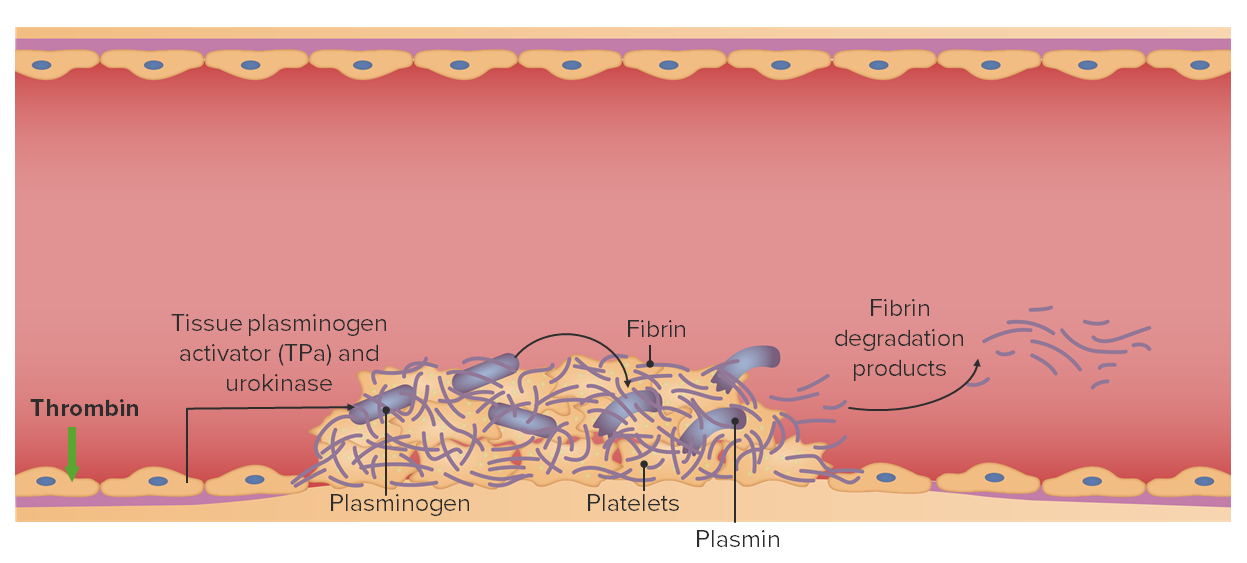
00:01 Thrombolytics are a different drug category that we use in coagulation cascades. 00:07 Now, thrombolytics are different from anticoagulants in that they are active against clots that have already formed. 00:14 So thrombolytics are a completely different class of drugs. They catalyze conversion of plasminogen to plasmin, and plasminogen to plasmin causes breakdown of fibrin. So the fibrin blood clot is actually broken down. 00:29 It is used often in acute stroke after you've confirmed that there is no hemorrhage on the CT scan. 00:36 We also use it in acute MI but that's more replaced by catheterization. Adverse events of course are bleeding and intracerebral hemorrhage. Now, I'm going to give you a clinical pearl that won't be useful on your exam but it's going to be useful in the real world. When you have a person who has an acute intracerebral hemorrhage, they will tell you somebody hit me in the back of the head with a baseball bat. They are so emphatic about how swiftly the headache came on and how severe it is that it's quite shocking. And I had a patient when I was a medical student who was put on a thrombolytic and they ended up developing an intracerebral hemorrhage. She told me it was as if somebody came and hit her on the back of the head. We were quick, we consulted neurosurgery, we put a Burr hole in, drilled a hole in her skull and took of the pressure and we preserved brain function and she lived. 01:30 Had we not done that quickly within at least an hour of treating the patient that patient would have died. 01:39 So, clinical pearl, intracerebral hemorrhage from these drugs, treat it very quickly with neurosurgery consult. 01:48 Streptokinase is the prototypical drug and generally on exams we'll talk about streptokinase but we also talk about other ones in the real world. It does not show an affinity for fibrin-bound plasminogen. There are tPA analogues which are replacing streptokinase and they show affinity for fibrin bound plasminogen. Alteplase is the prototypical drug with the tPA analogues. Tenecteplase is a recombinant variant of human tPA that has a longer duration of action and has now become probably the most commonly used thrombolytic out there. 02:24 Reteplase is another recombinant variant of human tPA which has a faster onset and longer duration, and may end up replacing the other drugs. Let's talk about procoagulants. 02:35 Let's talk about drugs that are given to patients who are bleeding excessively and we need to fix it. 02:41 We'll start of first with vitamin K. So if you remember when we were talking about warfarin, I was telling you that warfarin inhibits vitamin K dependant clotting. Well, if you give more vitamin K, you are going to reverse that effect. 02:55 Remember that vitamin K is fat soluble. So A, D, E, and K are fat soluble vitamins. Remember that most vitamin products will contain vitamin K even though they don't list it on the bottle, and that's because it's hard to extract vitamin K from vitamin A, D, and E. 03:12 So vitamin K is activated through the liver. 03:16 Replacement factors also include fresh plasma, purified human clotting factors. And they can be factor VIII concentrates for patients who have hemophilia A and factor IX concentrates for patients who have hemophilia B. 03:31 Octaplex and Beriplex are mixture of factors. Factor II, VII, IX, X, protein C. These are used in mixed coagulation deficiencies and in patients who have overdosed on the novel anticoagulant drugs, like rivaroxaban and apixaban. 03:51 There is a brand new class of drugs that you need to know about. They are called the monoclonal antibodies. 03:56 They are going to completely change medicine. One of the first ones that are out in terms of coagulation is idarucizumab, or Praxbind. These monoclonal antibodies are completely changing the way that medicine is being practiced in every single field. Hematology has Praxbind. It binds directly to the agent that is causing the anticoagulant defect. It is very very effective and has minimal side effects. Other procoagulants include the vasopressin agonists. Desmopressin is used commonly as a V2 agonist. It increases the concentration of von Willebrand's factor and the factor VIII. And it's also used to prepare hemophilia A patients or von Willebrand's patient for surgery. 04:43 Antiplasmin agents are also procoagulants. Procoagulant Amicar, or aminocaproic acid and these other agents are orally taken. 04:52 can be administered either orally or intravenously. 04:55 They inhibit fibrinolysis by inhibiting plasminogen activation. They increase the concentration of von Willebrand's factor and the factor VIII. They are used to treat hemophilia. They are used for prophylaxis in those high risk patients, and they are used in post-op bleeding. And the most common place where you are going to see them as a student or as a physician is in post-op bleeding cases. In terms of exams, it's important to know aminocaproic acid as the prototypical drug and that's the one that we are going to be using on questions.
About the Lecture
The lecture Thrombolytics and Procoagulants by Pravin Shukle, MD is from the course Pharmacology of Blood Coagulation. It contains the following chapters:
- Thrombolytics
- Procoagulants – Vitamin K
- Procoagulants – Replacement Factors
- Procoagulants – Vasopressin Agonists
- Procoagulants – Antiplasmin Agents
Included Quiz Questions
Which statement is most accurate regarding the comparison between alteplase and streptokinase?
- Alteplase shows an affinity for fibrin-bound plasminogen, while streptokinase does not.
- Alteplase is more widely used worldwide.
- Alteplase has a lower risk of intracerebral hemorrhage
- Alteplase has a lower cost.
- Alteplase is contraindicated in myocardial infarction, while streptokinase is not.
Which test must be performed prior to the administration of thrombolytics in a person with a suspected ischemic stroke?
- Head CT without contrast
- Head CT with contrast
- Platelet count
- International normalized ratio (INR)
- Cardiac biomarkers
Which of the following vitamins is water soluble?
- B1
- K
- D
- E
- A
Which procoagulant therapy exerts its effect by inhibiting plasminogen activation?
- Aminocaproic acid
- Idarucizumab
- Vitamin K
- Fresh frozen plasma
- Octaplex
Author of lecture Thrombolytics and Procoagulants

Pravin Shukle, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
