Playlist
Show Playlist
Hide Playlist
Hyponatremia: Management

-
Slides Water Balance Hypo and Hypernatremia.pdf
-
Reference List Nephrology.pdf
-
Download Lecture Overview
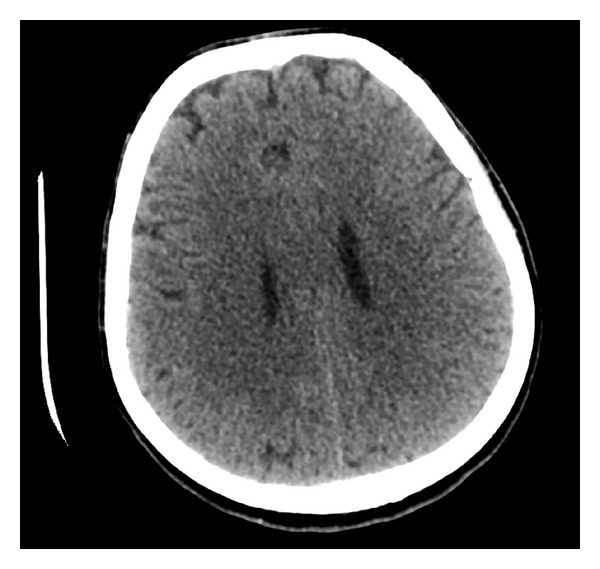
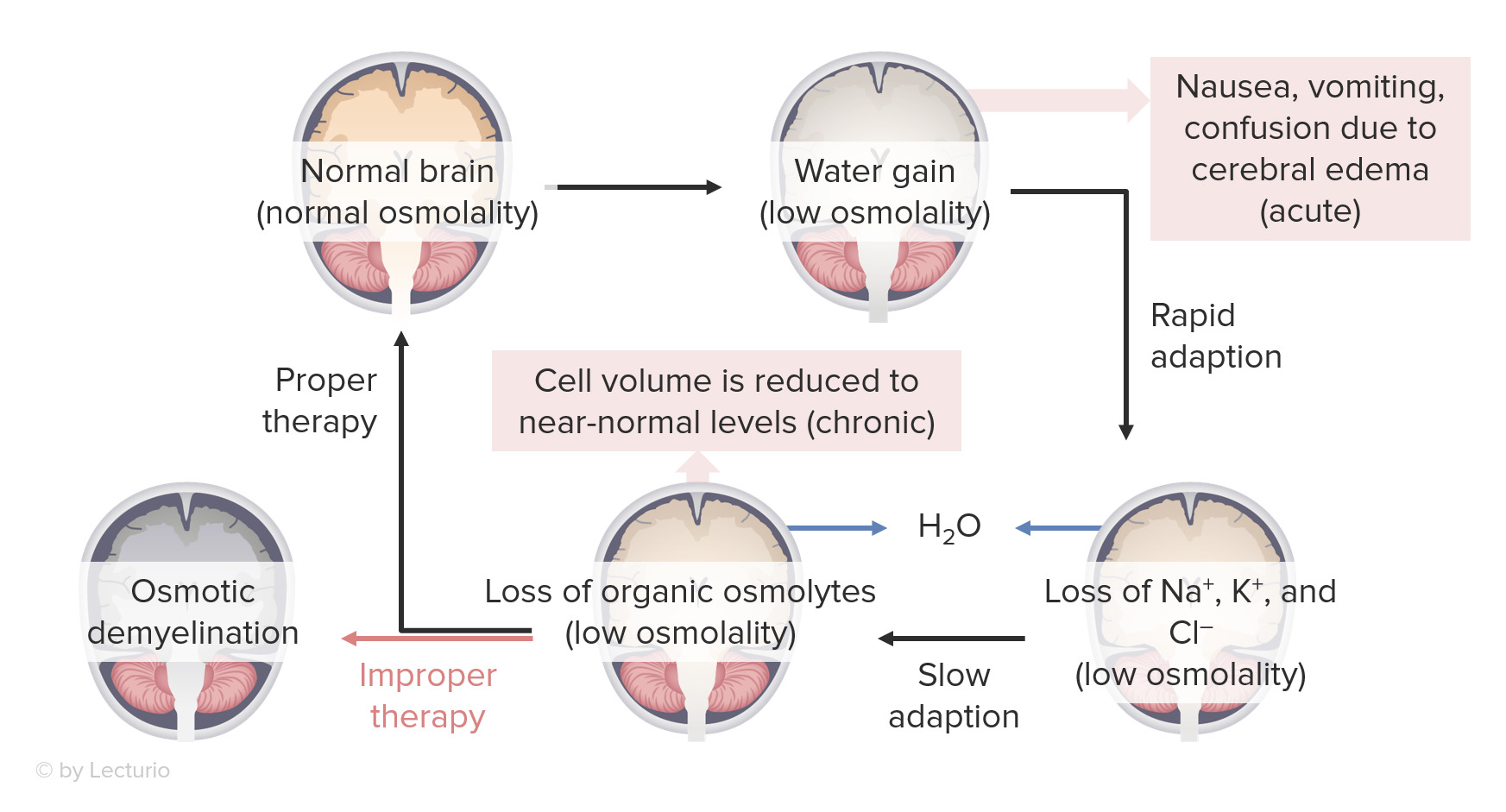
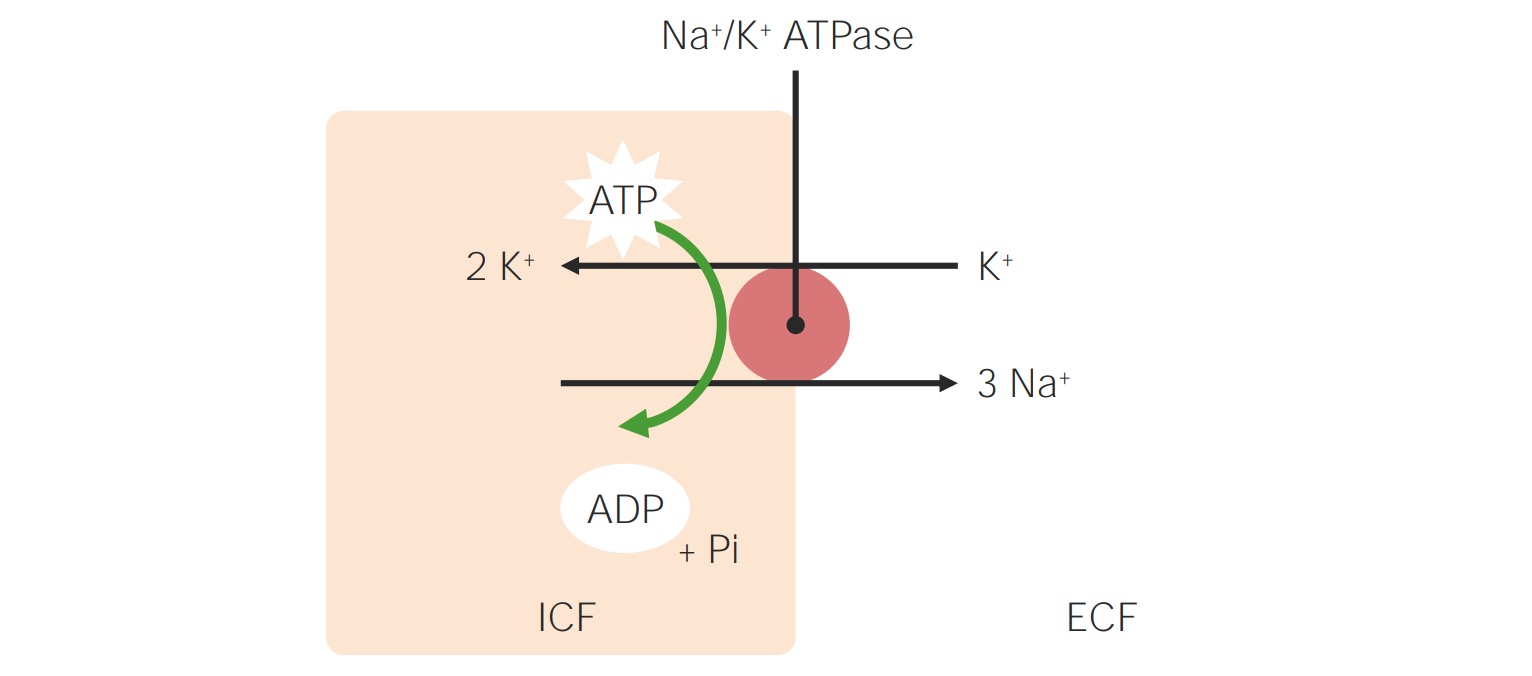
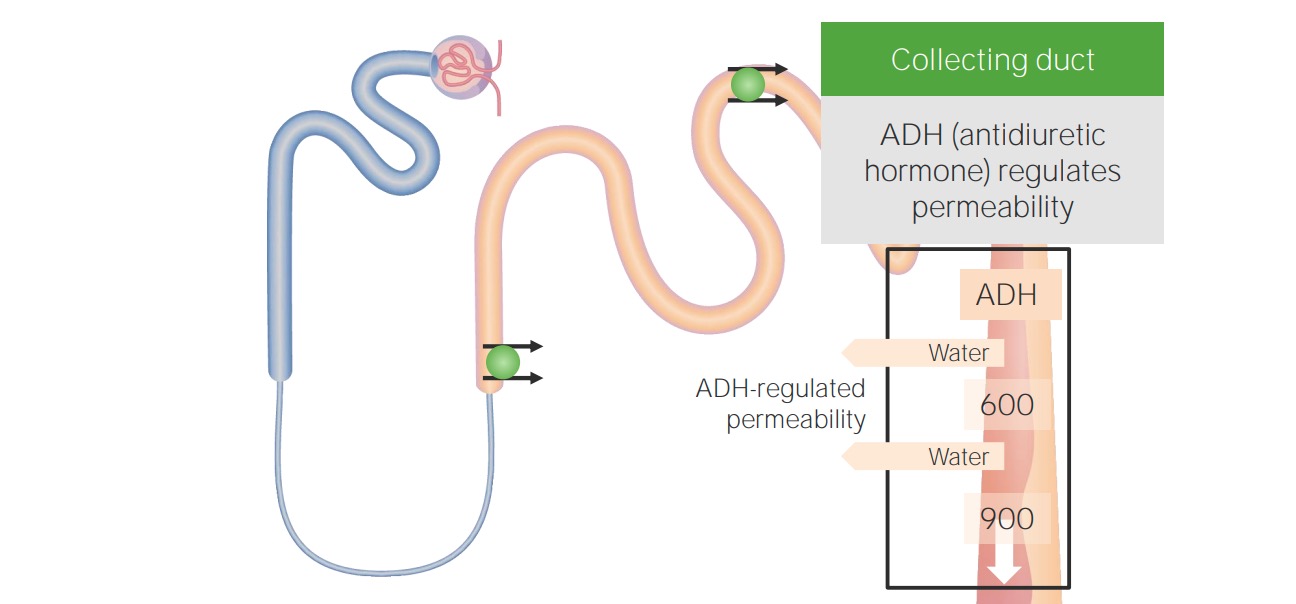
00:01 When it comes to the management of our patients with hypotonic hyponatremia, then it's really going to depend on the underlying cause. 00:10 So in our patients who have hypovolemic hypotonic hyponatremia, what we want to do is correct the intravascular volume with isotonic fluid. 00:19 By doing that we will release the stimulus for ADH. 00:23 So typically in that situation, we want to give our patients isotonic fluids like 0.9% or normal saline. 00:30 Now, we have to be very careful when doing so because remember, as you start to repeat that patient's vascular volume, you will turn off ADH. 00:39 And that patient will now have a significant water diuresis. 00:43 So you will have to follow their serum sodium very closely so that you don't overcorrect those patients. 00:49 In our patients who have euvolemic hypotonic hyponatremia, it's important to correct the underlying cause, so treating hypothyroidism. 00:56 Or having patients increase their solute intake. 00:59 If they are tea and toast dieter, or somebody who has beer potomania. 01:04 For SIADH, we strive to correct the underlying cause if it's identifiable. 01:09 But if not, an ADH remains present, there's a couple of things that we have to keep in mind. 01:14 Number one, we want to free water restrict our patients. 01:17 So that means really reducing water intake, and that's all hypotonic fluids to somewhere between 0.8 and 1.2 liters of water daily. 01:27 We want to increase their solute intake. 01:29 Remember, by increasing solute intake, we increase our osmolar generation. 01:34 And the more osmoles we make then the more water we can excrete, because of that obligate osmolar excretion. 01:43 We can give our patients things like loop diuretics. 01:46 That's going to abolish the medullary gradient, and that will help us also excrete more free water. 01:52 And then finally, we can give our patients V2 receptor antagonists. 01:55 Medications like conivaptan or tolvaptan, which directly antagonize V2 receptors. 02:01 Now, they're available, but they are costly. 02:03 And it's something that we can use in our patient population. 02:06 In our hypervolemic hypotonic hyponutrimic patients, remember they have total body sodium access or ECB access. 02:14 So we want to manage those patients with diuretics. 02:16 And we also want to fluid restrict them as well. 02:20 Now, there is something I want you to keep in mind when it comes to correcting patients who have chronic hypotonic hyponatremia. 02:26 That means that they've been hyponatrimic for greater than 48 hours period of time. 02:31 That sodium correction should never exceed greater than 8 milliequivalents within a 24 hour period of time. 02:37 If it does, that patient can be at risk for osmotic demyelination syndrome. 02:43 We'll talk about that in just a moment. 02:45 Alternatively, what I do want to tell you is that if the patient is symptomatic, and they have life threatening seizures because of cerebral edema. 02:52 It is okay to raise their serum sodium rather quickly by about four to six milliequivalents to get them out of the danger zone with hypertonic saline. 03:00 Now, let's review what happens with osmotic demyelination syndrome. 03:05 Just to remind us what happens in the situation of hyponatremia. 03:09 Remember, water is going to be primarily distributed to the intracellular fluid volume. 03:14 Now that's fine, but when it comes to our neuronal cells, they are enclosed by a rigid calvarium. 03:21 Therefore, when they expand, patients will experience cerebral edema. 03:25 They might feel nauseated, they might vomit or have confusion because of that cerebral edema. 03:31 And our bodies being elegant as they are have that adaptive mechanisms. 03:35 So acutely, we will use things like sodium, potassium, and chloride to the extracellular fluid volume, water follows and shrinks those cell volumes down to the normal size. 03:45 If this is happening chronically, meaning greater than 48 hours, then we start to lose organic osmolytes into the extracellular fluid volume. 03:52 Again, water follows. 03:54 So it brings our cells back to the normal volume. 03:57 Now, let's think about what happens if we all of a sudden try to restore patient's serum osmolality back to the normal. 04:04 So if we have something that is hypertonic to their plasma osmolality, then what's going to happen? Water is going to move from that intracellular compartment to the extracellular fluid compartment. 04:17 These cells remember, already have lost organic osmolytes. 04:21 So they start to shrink even further. 04:23 And when that happens that stimulates osmotic demyelination. 04:28 The way that patients manifest is it can happen anywhere from two to three days after the event up to two to three weeks. 04:34 And they oftentimes will have severe debilitating neurological symptoms, including choreiform movements or even locked-in syndrome. 04:42 So it's extremely debilitating. 04:44 And the people who are most at risk are going to be your malnourished patients and females that are typically middle to older age.
About the Lecture
The lecture Hyponatremia: Management by Amy Sussman, MD is from the course Water Balance: Hypo- and Hypernatremia.
Included Quiz Questions
What is the appropriate management of hyponatremia in acute gastroenteritis with diarrhea?
- Normal saline (0.9% NaCl)
- Hypertonic saline (3% NaCl)
- Half-normal saline (0.45% NaCl)
- Hypotonic saline (0.3% NaCl with dextrose)
What is the first-line treatment of primary polydipsia?
- Water restriction
- ADH antagonist
- Aldosterone antagonist
- SSRIs
- Salt restriction
Author of lecture Hyponatremia: Management

Amy Sussman, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
