Playlist
Show Playlist
Hide Playlist
Heart Failure (HF): Pathogenesis and Etiologies





-
Slides CongestiveHeartFailure CardiovascularPathology.pdf
-
Download Lecture Overview
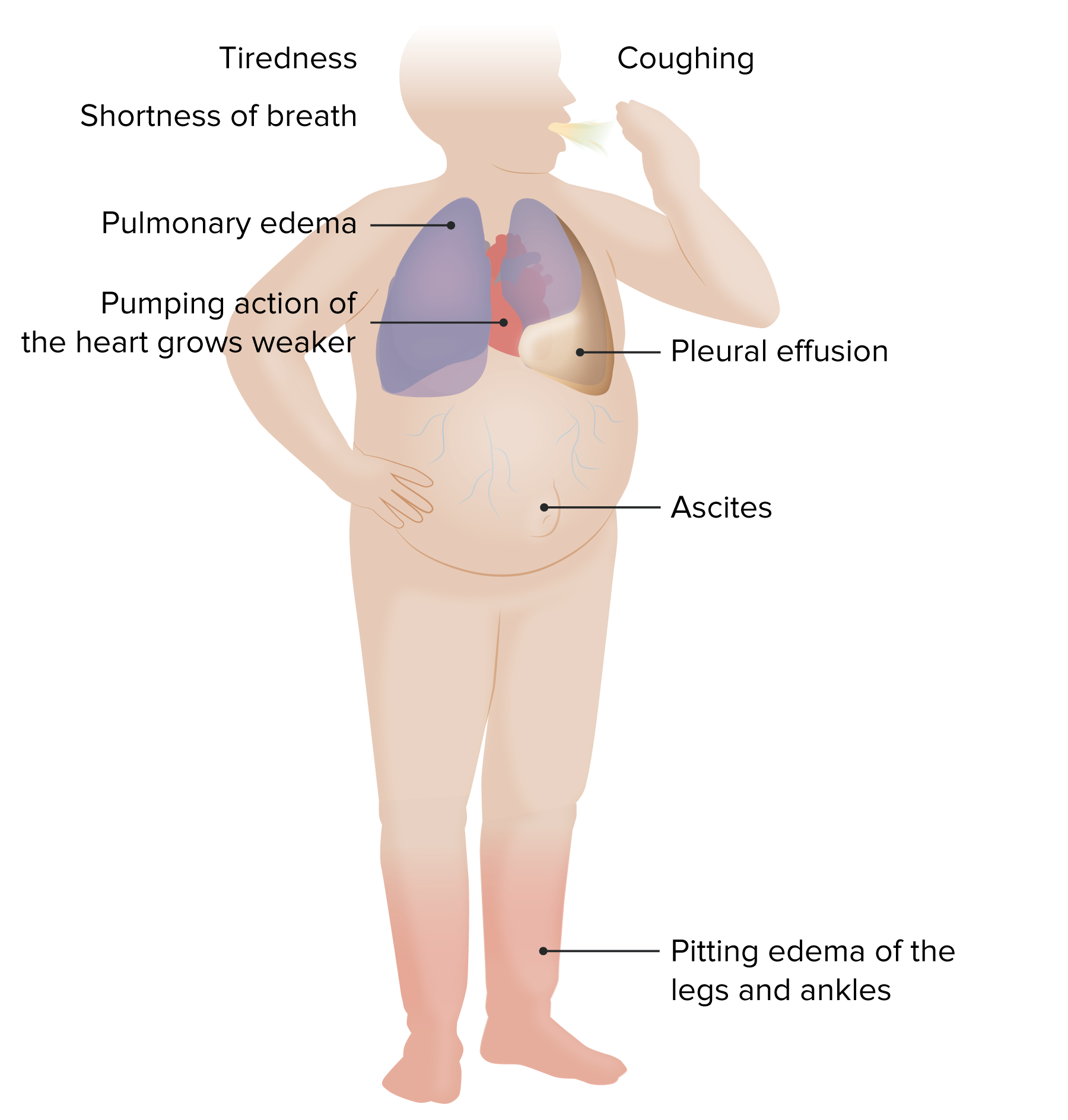
00:03 We will take a look at the myocardium. With the myocardium, it is the fact that we are working with the middle part of the heart. If it is endocardium, then you are thinking more along the lines of valvular heart disease perhaps. It is exactly what you are doing. 00:17 So let's take a look at the myocardium and the categories of pathologies that come under or affect the myocardium. We will take a look at CHF, congestive heart failure. You know this as being end-stage heart disease. So, anything that causes damage to the myocardium from dilated cardiomyopathy to hypertrophic cardiomyopathy to restrictive cardiomyopathy and so forth, eventually if there is enough death that is taking place in the myocardium, are you not going to result in CHF? The most common cause of CHF is going to be ischemic. 00:53 So, if your patient has something like an ST elevation in leads V1, V2, and V3, and then you know there is a transmural myocardial infarction affecting which coronary artery? The left anterior descending and at some point later on down the road, your patient may develop congestive heart failure. You see my point. So ischemia would be a very common cause or actually it is the most common cause of CHF. CHF final and common pathway of myocardial disease. Now the way that we will approach this is dilated cardiomyopathy and hypertrophic cardiomyopathy would be relatively common at least in developed countries. Is that clear? You want to think that a dilated cardiomyopathy as being end-stage heart disease just like you have cirrhosis being end-stage liver disease. Listen to what I am saying. I am drawing a lot of parallels here and I will keep doing this for you so that you don't waste as much time memorizing details when you should have been looking at the big picture the whole time. Or honeycomb lung. You have heard of that before, which means excessive fibrosis and more along the lines of end-stage lung disease. So here, dilated cardiomyopathy including certain conditions that you would find with restrictive cardiomyopathy and you all know about hemochromatosis. If you don't, you should and you will. With hemochromatosis, you know that the heart is being encased by iron. Think about as such. So it may result in restrictive cardiomyopathy, but if there is enough damage that is taking place to the myocardium may you not result in dilated cardiomyopathy clinically? Of course, you will. So how can you distinguish between the two? Well, you should see. Alcohol-induced dilated cardiomyopathy. 02:50 Alcohol is, unfortunately, a common cause of this. Idiopathic, dilated. Hypertrophic cardiomyopathy. We had discussed hypertrophic obstructive cardiomyopathy with asymmetrical hypertrophy of the intraventricular septum resulting in obstruction of the outflow tract between the left ventricle towards the aorta. Did we not? And when we did, we talked about the different maneuvers. Restrictive cardiomyopathy, secondary to infiltrating diseases such as number 1 hemochromatosis, such as amyloidosis, which is then going to infiltrate the heart and, therefore, cause restrictive type of cardiomyopathy. Or perhaps there is something called EMF, which is endomyocardial fibrosis and there you go. What if you have fibrosis of the heart? May result in restrictive cardiomyopathy. What kind of countries and what kind of populations might you then be looking for when you dealing with endomyocardial fibrosis? You are looking at intense eosinophilia that may be occurring in your patient. Maybe later stages of Löffler syndrome. And looking at countries such as Africa, such as South India the subcontinent, with lots of restrictive cardiomyopathy and fibrosis. Endomyocardial fibrosis not to be confused with endocardial fibroelastosis found in young infants and we will talk about those differences when the time is right Restrictive. Probably one of the trickier in terms of diagnosis because students tend not to be familiar with or not understand the full pathogenesis. Once again to repeat hemochromatosis, sure it could result in restrictive. But if there is enough damage to the myocardium may result in dilated cardiomyopathy. Please do not ever forget that. Specific cardiomyopathies, ischemic, we talked about may result in dilated cardiomyopathy, CHF, valvular induced, hypertensive. 05:01 Well, with hypertensive may result in concentric hypertrophy of the left ventricle in which the sarcomeres are going to duplicate in parallel, resulting in what? Well, decreased size of the chamber of the left ventricle thus what kind of dysfunction? A diastolic dysfunction. 05:18 Physiologically what may then happen to your ejection fraction early on in hypertension? Are you able to preserve? Are there instances in which ejection fraction is preserved with heart failure? Sure there are. Hypertension early on, aortic stenosis early on. It is actually called heart failure of preserved ejection fraction, ejection fraction being approximately normal at 55 percent. Is that clear? These are important points and we have discussed this a couple of times. We will continue to do so that we would reinforce this constantly. We have inflammatory. So, here your myocarditis might be thinking about viruses such as Coxsackie. You might be thinking about adenovirus in myocarditis, viruses. Maybe even perhaps part of rheumatic heart disease. "Dr. Raj, I thought that was endocarditis and valvular heart disease and you even told me the four valvular disease of the rheumatic heart disease, acute type of regurgitations and the chronic type of stenosis. Why all of a sudden are you talking about myocarditis?" Because rheumatic heart diseases, pancarditis. You would have Aschoff bodies and Aschoff cells. 06:29 Myocarditis. Infections. HIV, enterovirus, Chagas. You sit there or actually stand up with me and do Chagas dance. What am I referring to? What was the Chagas? Dilated, dilated, dilated. Three different places obviously I am going to repeat this in three different organ systems. But Chagas from head-to-toe dilated esophagus. 06:54 What is this? Achalasia, acquired type. Where am I? Taking a cruise. Where? Down the South America and I ended acquiring trypanosoma cruzi. You picked this up and you have Chagas and it may result in acquired type of achalasia. What happens to the proximal esophagus? Dilation. 07:16 Dilated esophagus. In the heart, what kind of issue? You might have a dilated infectious myocarditis. What else may happen? Dilation. I said three times Chagas, Chagas, Chagas; dilation, dilation, dilation. The third and final dilation would be down in your intestine. 07:34 May result in acquired type of toxic megacolon. Is that clear? Chagas is important for us. 07:41 Endocarditis. Infection, metabolic disturbances. Well if your patient feels and tells you "Hey doc, I feel like my heart is going to jump out of my chest," and you find your TSH levels being ridiculously low. What is your diagnosis? And maybe even perhaps on a radioactive iodine test, you find diffuse uptake of radioactive iodine. Without a doubt your diagnosis, please? Good. Grave's disease. We have diabetes mellitus, of course, may result in issues in the heart. 08:14 Infiltrating. Hemochromatosis, amyloidosis and do not forget the sarcoidosis not only could affect your lungs resulting in non-caseating granuloma in which there might be bilateral hilar lymphadenopathy, which you can find these known cases in granuloma perhaps in the liver maybe as you see here in the heart. Do not forget that please, ever. 08:39 Now with rheumatologic disorders, SLE sure. You know about SLE and you might have the autoimmune disease, in which you have malar rash, but you could also have other types and other manifestations could be affecting the heart. You have polyarteritis nodosa may also affect the heart. It is usually medium sized may be perhaps small sized type of blood vessels might be affecting the heart. Scleroderma you are thinking about fibrosis immediately and dermatomyositis in which you find skin lesions. You have heard of Gottron lesions over the knuckles, heliotrope and then muscle in which finally it might affect your heart.
About the Lecture
The lecture Heart Failure (HF): Pathogenesis and Etiologies by Carlo Raj, MD is from the course Heart Failure: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following is LEAST likely to cause congestive heart failure in a patient who has never left the US?
- Chagas disease
- Valvular heart disease
- Sarcoidosis
- Rheumatic heart disease
- Alcohol
What is the most common cause of congestive heart failure in the US population?
- Ischemic heart disease
- Rheumatic fever
- Mitral valve prolapse
- Hemochromatosis
- Coxsackievirus
Which of the following is NOT associated with rheumatic heart disease?
- Staphylococcus infection
- Aschoff bodies
- Valvular insufficiency
- Pericarditis
- Myocarditis
Which of the following conditions is one of the consequences of congestive heart failure?
- Hepatic congestion
- Asthma
- Diabetic neuropathy
- Hematuria
- Hemorrhagic stroke
Which of the following is NOT a cause of restrictive cardiomyopathy?
- Alcohol
- Sarcoidosis
- Hemochromatosis
- Amyloidosis
- Endomyocardial fibrosis
Author of lecture Heart Failure (HF): Pathogenesis and Etiologies

Carlo Raj, MD
Customer reviews
4,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
1 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Not bad, it seems to jump around and rush a little bit. It would be good if CHF in general was properly defined and explained before etiologies were spoken about
points out the important points and links with other knowledge
