Playlist
Show Playlist
Hide Playlist
Congenital Vascular Malfunctions of the Aorta – Vascular Malformations


-
Slides 13 VascularMedicine advanced.pdf
-
Reference List Vascular Medicine.pdf
-
Download Lecture Overview
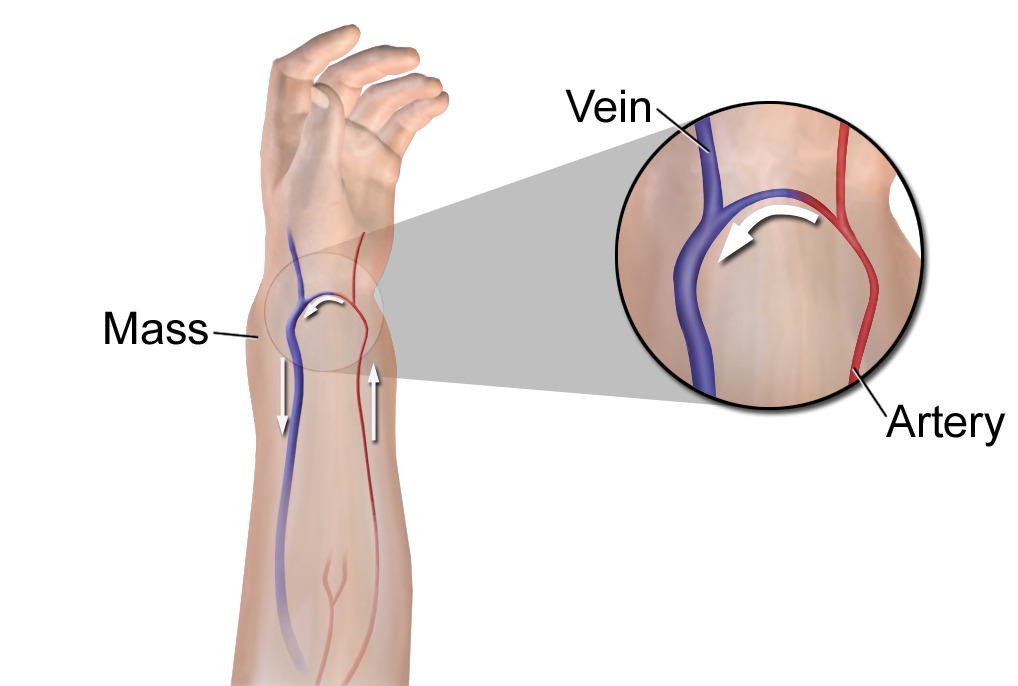
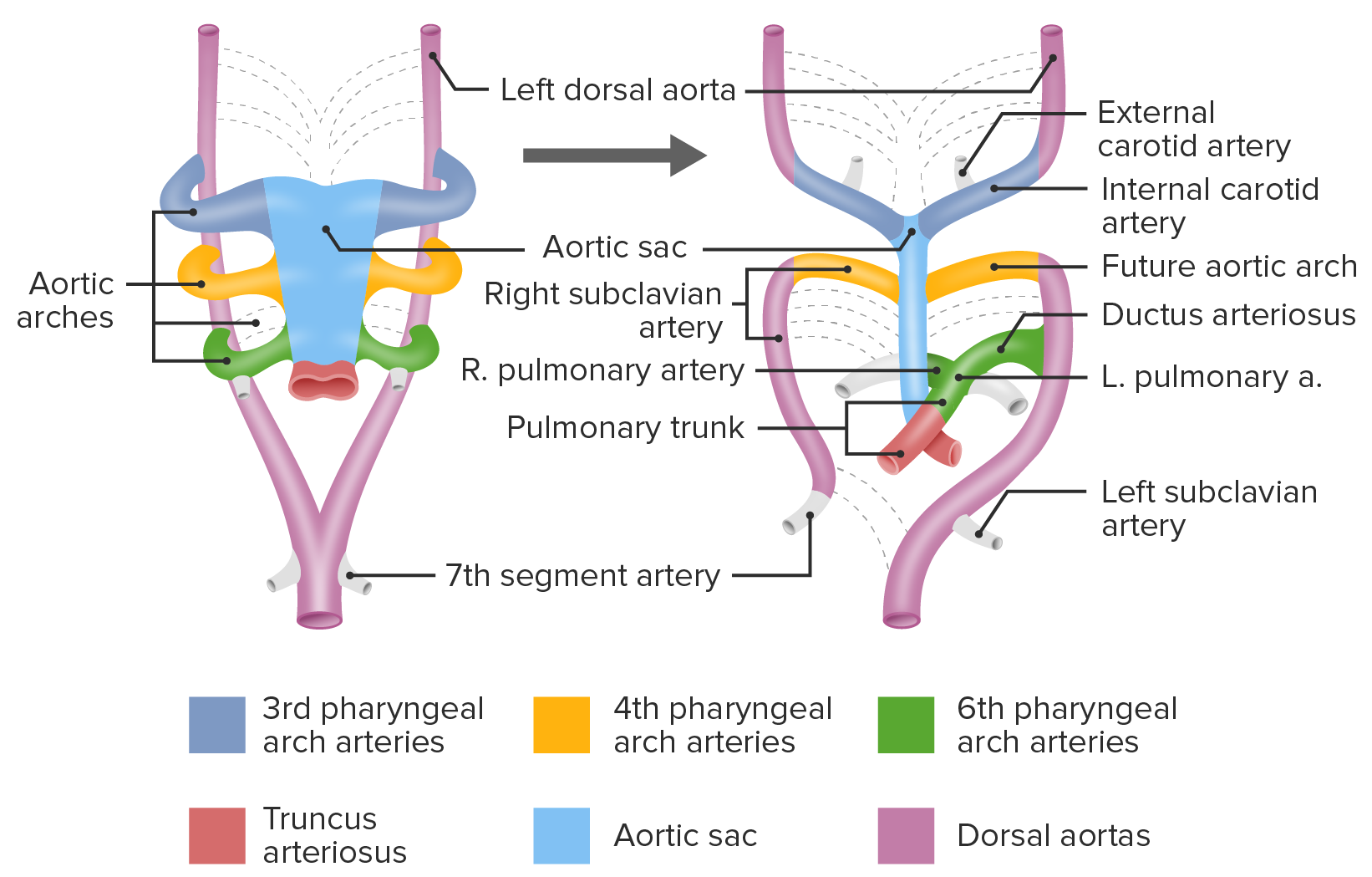
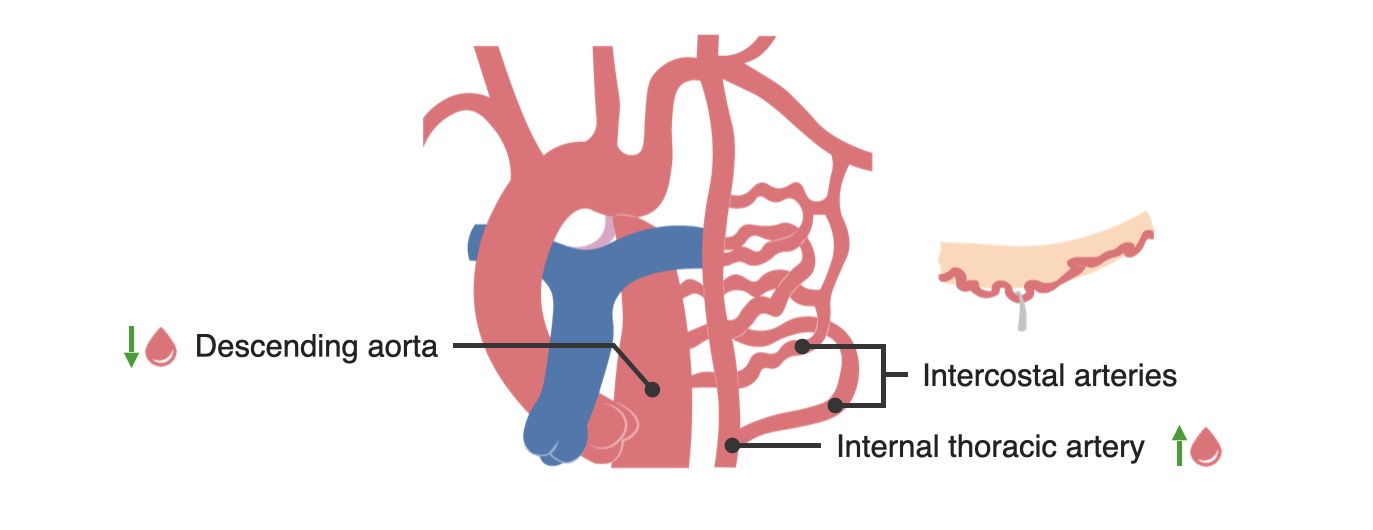
00:00 Let’s move then from these very nasty or potentially very nasty AV malformations to ones that may be of interest to the radiologist as a curiosity and, occasionally, cause symptoms and require surgical repair. And these are congenital vascular malformations of the aorta. 00:23 Let’s take a moment to consider what happens in embryonic life as the heart forms. 00:29 When the heart forms, the aorta is often seen as a series of arches just like one sees in the fish. And this has been commented on many times that, in embryonic life, the human fetus goes through earlier evolutionary stages that imitate animals that are more primitive shall we say compared to mammals. And you actually go through a period as a fetus where you have the aortic arches of a fish. And gradually all of those arches involute. They disappear except from one, which is the main aorta that remains. I’ll show you a diagram in a moment of all these arches that disappear. 01:12 Occasionally, they don’t disappear and one remains. And sometimes these arches will put pressure on the esophagus or on the trachea and can cause breathing or swallowing problems. 01:25 What you see in the x-ray figure here is a barium swallow. Barium looks white to the x-ray. And you’ll notice that there’s an indentation, a partial interruption of the esophagus. And that’s because there’s a persistent congenital aortic arch that should have involuted but didn’t. And it’s putting pressure on the esophagus. And this patient would have trouble swallowing because the food would get stuck where the aortic arch is pressing against the esophagus. And so this person would probably need surgery to remove that arch, to obliterate it. 02:01 And there may be also abnormalities in some of the vascular branches of the major blood vessels that can also cause some problems from compression because they’re in a place they don’t belong. 02:13 So here’s the cartoon. You’ll see the dotted lines there. All represent the embryonic arches that are supposed to involute. But in fact some of them may not involute as I said before and, if they’re persistent, they may cause problems by compressing either the esophagus or the trachea. 02:33 Here are some examples of these persistent aortic arches. And you can see they can encircle the trachea, they can encircle the esophagus. And they can put pressure on both of them. 02:48 And you can see there’s a whole variety of different ones where they’ve been [Inaudible 0:17:08]. Atretic means involuted or disappeared or they can be totally persistent in a complete circle around the trachea and the esophagus. And the more encircling they are and the tighter they are, the more likely they are to cause trouble with breathing or with swallowing. 03:10 Here’s a typical example. It’s a double arch. You can see how it’s pressing on the oesophagus. It encircles the trachea and the oesophagus. It cause compression of both structures. 03:26 And the degree of compression of course varies. Sometimes, it’s only a little bit and so the patient doesn’t need surgery. They’re going to be able to breathe and swallow okay. 03:34 Usually, the right arch is larger and passes behind the esophagus. And the right common carotid and the subclavian arteries arise separately from the right arch as opposed to from the normal single arch. 03:49 In any case, if there’s obstruction to the trachea or the esophagus, these patients have to be operated on. Usually what happens is you interrupt the middle portion and then you put a graft in so that there’s a normal arch created surgically. And of course that eliminates the obstruction to the oesophagus and the trachea. 04:11 Another form of congenital abnormality we’ve talked about a number of times before because it’s a cause of hypertension and that is coarctation of the aorta. 04:21 This is a narrowing, or a constriction, in the aorta just beyond the left subclavian artery. It’s in the area where the ductus arteriosus that carries blood during embryonic life exists. And the area there right around the ductus fails to develop normally. And so you end up getting a constriction in the aorta at that point, usually just beyond where the ductus would have been. 04:49 And you can see it in the diagram in the green circle. It’s where the coarctation usually forms. 04:57 They can be mild or they can be quite severe. It’s usually picked up early in life because teenagers are found to have hypertension. You can get an infection in it – bacterial endocarditis. And it can even rupture but those complications are rare. 05:13 When it’s picked up beyond age 50, it’s often associated with brain bleeding because there are small aneurysms of the cerebral blood vessels that occur. And it is also associated with a bicuspid aortic valve. So you may developed dissection of the aorta. And, even when this is repaired either surgically or with a catheter stent, hypertension often persists in these individuals. 05:40 The clue as you may remember we talked about from the physical exam is: you feel the radial pulse and you feel the femoral pulse. And you notice that the radial pulse is occurring a lot earlier than the femoral pulse. Sort of, “thump, thump” as opposed to almost simultaneously in a normal person. And of course also the patient has hypertension in the upper extremities and usually hypotension in the lower extremities. So, if you did a brachial-ankle index, you would find marked decrease in the blood flow in the ankle compared to the arm. 06:14 Finally, there’s a very common cosmetic lesion called a port wine stain. And this results from areas of abnormal capillaries and small veins – venules. They’re dilated and filled with blood and they lie just beneath the surface of the skin and they’re present at birth. And they’re quite common. If they are disfiguring cosmetically like in the little cartoon here, one can in fact obliterate them with a laser. And dermatologists do this all the time. 06:51 They are called port wine stains because the colour is often that of a deep purple like the colour of port wine.
About the Lecture
The lecture Congenital Vascular Malfunctions of the Aorta – Vascular Malformations by Joseph Alpert, MD is from the course Vascular Malformations.
Included Quiz Questions
Which of the following is the most common presenting symptom of the coarctation of aorta in a teenager?
- Hypertension.
- Diabetes.
- Arrhythmias.
- Brain hemorrhage.
- Poor peripheral perfusion.
An abnormal finding in which of the following types of examinations is more suggestive of aortic coarctation?
- Palpation for radiofemoral delay.
- ECG.
- Auscultation for apex beat.
- Auscultation of thoracic cavity.
- Auscultation for blood pressure.
Author of lecture Congenital Vascular Malfunctions of the Aorta – Vascular Malformations

Joseph Alpert, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
