Playlist
Show Playlist
Hide Playlist
ECG Findings with Bundle Branch Blocks and V-tach





-
Slides Tachyarrhythmia VentricularTachycardia CardiovascularPathology.pdf
-
Download Lecture Overview
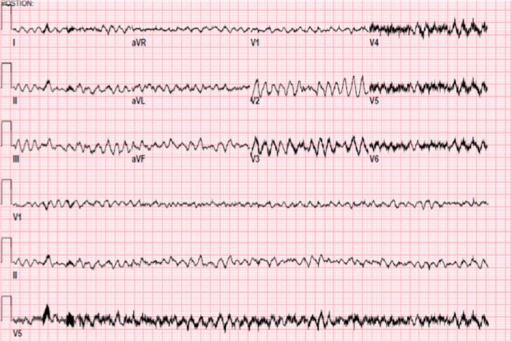
00:00 Let us take a look at a typical LBBB pattern, left bundle-branch block. Slow down for one second, now before we go and dive into the EKG, which at this point I would not recommend. I would first pay attention to what kind of changes you would expect to see or hear from the history of the patient. For example, if you are to do a cardiac ausculation with the left bundle-branch block, this would mean that you have a delayed conduction through the left bundle branch. 00:27 So, therefore, the first depolarization will pass through the right bundle branch. If that happens, then the pulmonic valves will closed first prior to the aortic, thus you have a paradoxical split. That would be the most important aspect of left bundle branch block. 00:45 Now, when it comes to EKG, you have been given a 12-lead ECG, well you are looking at your V2, V3, V4 in which the QRS complex at this point, in fact, has been widened, but it is much more important that you pay attention to the EKG upcoming with RBBB. Now, with right bundle-branch block here, you are going to have a delayed conduction passing through your right bundle branch. So, you have a depolarization passing through left bundle branch first as you would have normally. However, now because it takes the pulmonic valve to close a little bit later, you are not going to have a fixed split. You will have a wide split. 01:24 A fixed split would be upon inspiration, expiration that the length in the span of your S2 between A2 and P2 would not be changing and that would be something like your atrial septal defect as being the most common type of differential. However, if you find a right bundle-branch block, well you would have a widening, but the size of the span between A2, P2 would change between inspiration expiration, but it would be widened in nature. Now, I want you to pay attention on EKG now, based on feedback, a 12-lead ECG and what has been circled here? You notice rabbit ears is what they are called. You have a RSR' pattern. 02:09 This I need you to be able to identify on your EKG, on a 12 lead and with that type of historym with the wide split, no doubt, your diagnosis RBBB. This is the EKG at this point that you pay attention to. Then when you get a moment, go back to that electrocardiogram that I showed you with LBBB, but as I said with LBBB, you'd pay attention to the paradoxical split. Is that clear? Let us now move on. Now we move on to what's known as ventricular tachyarryhthmia, your focus should be the fact that the ventricles are involved. The ventricles, which means that you are going to find issues with which wave? QRS complex. 02:55 I want you to take a look at the bottom lead. Also, what I am doing here with this entire section of arrhythmia is I am trying to get you into the habit of looking at all 12 leads. 03:06 Gone are the days where they are just going to give you a simple rhythm or simple lead. 03:10 It just being one lead in which you need to interpret that. Gone are those days. Even with flutter, fibrillation any one of those, there is a difference between, let us say a licensing exam giving you one lead versus giving you all 12. Because now all of a sudden even you didn't know about your ADHD kicking in. Dr. Raj, I didn't even know I had, but they gave me 12 leads. I don't even know what to look at because this is too much. That is why you get conditioned. You take a look at 12 leads. Here we go. Don't panic and you focus on things which you definitely know. So we will take this opportunity to pay attention to lead 1, 2 and 3. What does that mean to you? Lead 1 left side, lead 2 you are looking at 60 degrees approximately and once that you want to pay attenion, you grouped together based on myocardial infarction, we have done this before. II, III, aVF, inferior portion. 04:04 Welcome to right coronary artery. Lead 1, aVL, V5, V6 that would be the left circumflex, that will be lateral side. If it is medial side and then you are looking at a septal portion looking at V1, V2, V3, V4 that will be intraventricular down and then towards the apical and there would be something like your left anterior descending. You see the pattern. So each one of these 12 leads that you are going through, establish a pattern for yourself and I would like you to move in a serpentine nature, meaning lead 1, lead 2, lead 3 go up to aVR, aVL, aVF go to V1, V2, V3 and I want you to move in a snake-like manner with every single 12-lead ECG that you get. Then at the bottom that is the seperate strip. That is a seperate lead that you pay attention to because that would be the one that shows you the pathology. Is that clear? This is how you need to read ECGs for any licensing exam. 04:58 And by the way, you have cardiologists and experts that will call that ECG and EKG, it's the same thing. In Germany, it is EK cardio whereas it in English, it is EC. Ultimately do not get confused on that. It is the same darn test. Let us move on.
About the Lecture
The lecture ECG Findings with Bundle Branch Blocks and V-tach by Carlo Raj, MD is from the course Arrhythmias: Basic Principles with Carlo Raj.
Included Quiz Questions
What conduction defect results in paradoxical splitting of the second heart sound?
- Left bundle branch block
- Right bundle branch block
- Atrial fibrillation
- Wolff-Parkinson-White syndrome
- Atrial septal defect
What conduction defect is as an RSR’ pattern in leads V2 and V3 on a 12-lead ECG?
- Right bundle branch block
- Left bundle branch block
- Long QT syndrome
- Torsades de pointes
- Atrial septal defect
Which of the following ECG leads represents the distribution of the left circumflex artery?
- I, aVL, V5, V6
- II, III, aVF
- V1, V2, V3, V4
- Lead II
- V1-V5
Author of lecture ECG Findings with Bundle Branch Blocks and V-tach

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
