Playlist
Show Playlist
Hide Playlist
Types of Diarrhea

-
Slides Small and large bowel.pdf
-
Download Lecture Overview
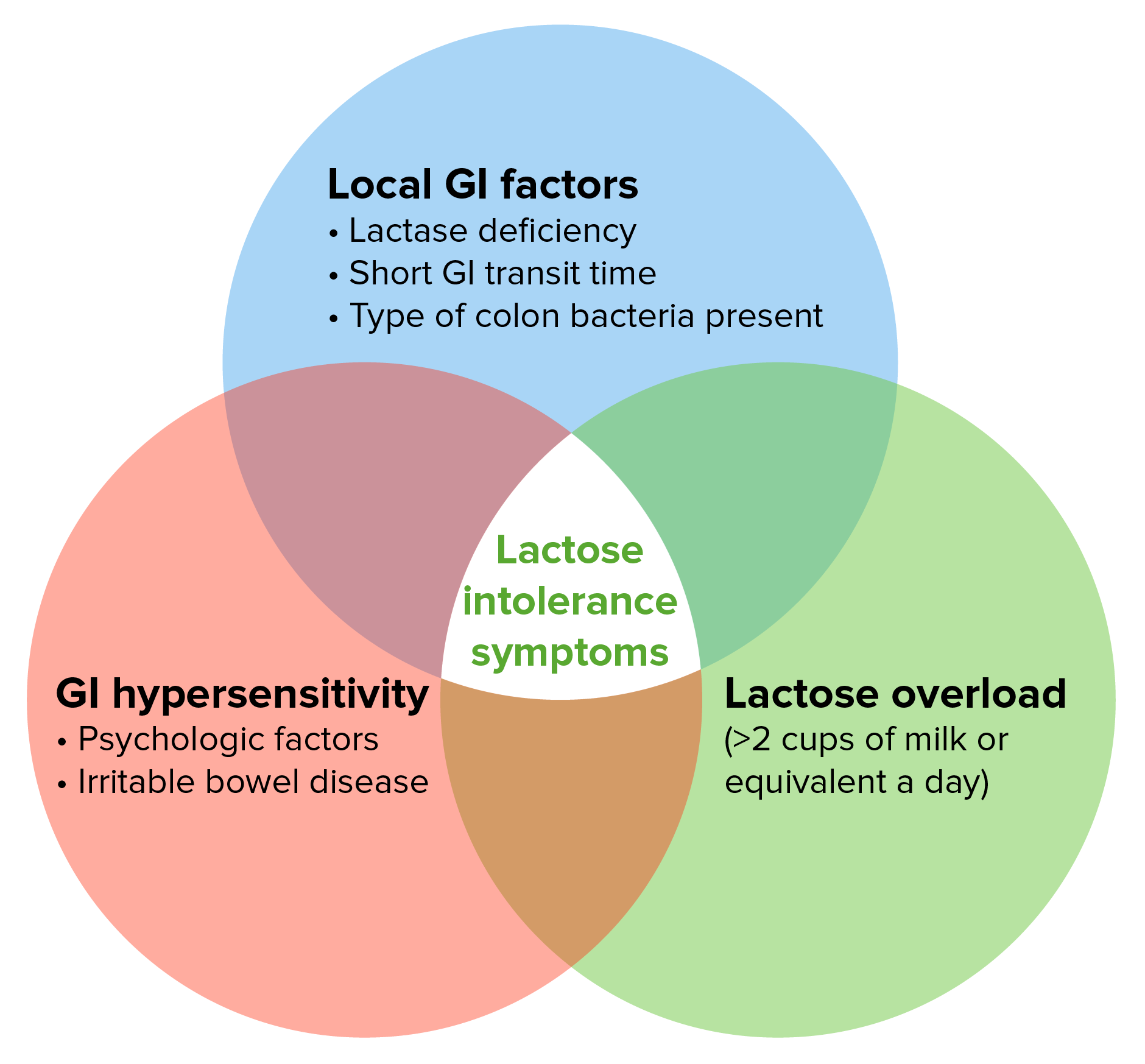
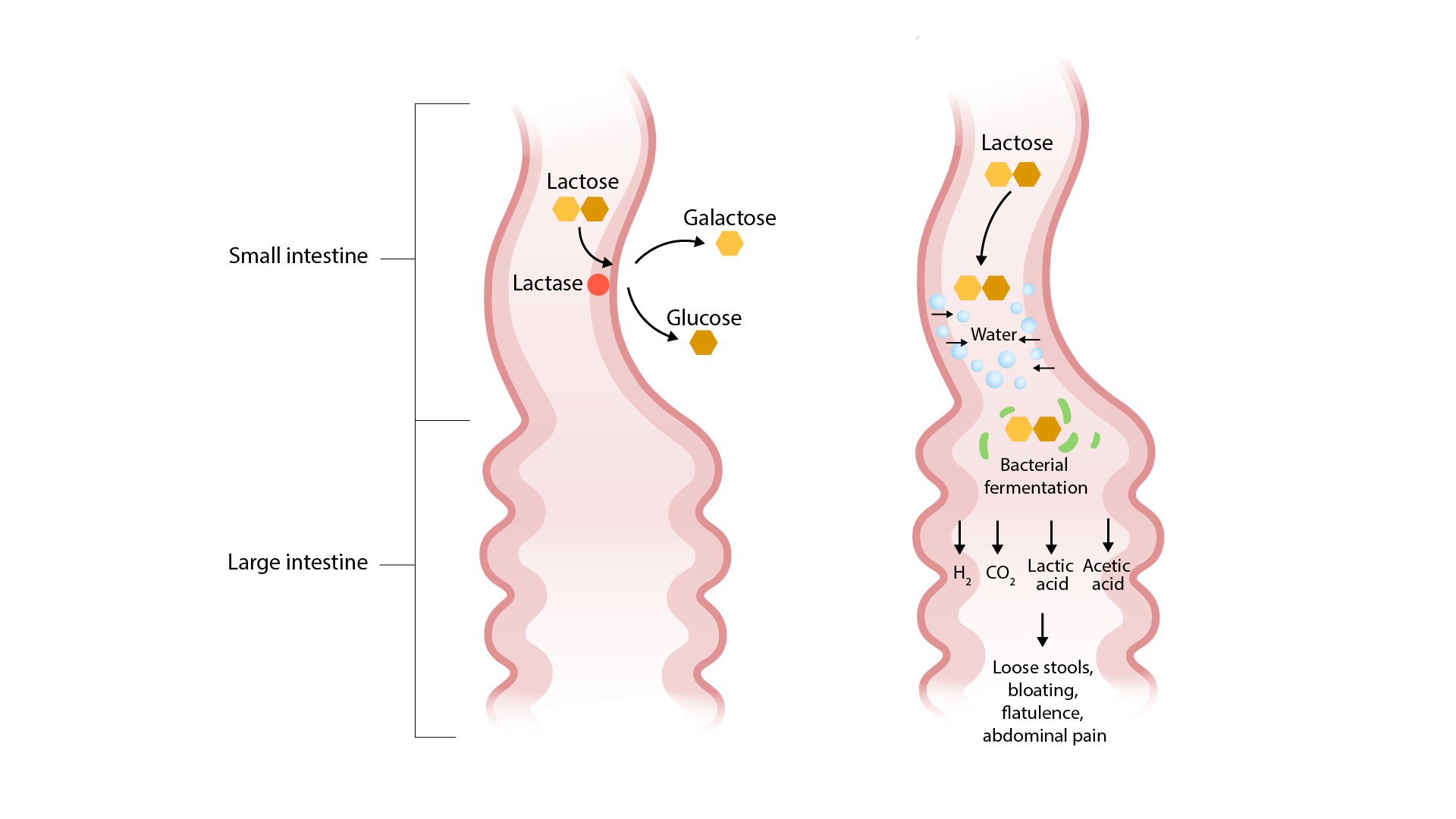
00:01 At this point, we will then categorize our diarrhea. 00:05 This is important table for you to able to properly organize your thoughts. 00:09 The category of the type of diarrhea, clinical conditions and the important comments of each one of these. 00:16 Osmotic diarrhea. 00:19 Or you can have a patient who is actually lactase deficient. 00:24 What does that mean to you? Remember that if you are reabsorbing your glucose from your intestinal lumen, you have to have it in the form of monosaccharide. 00:37 The type of monosaccharide that becomes the most important to you physiologically and then here pathologically will be glucose. Others include galactose as well. 00:46 The combination of glucose and galactose gives you an interesting disaccharide and that being the lactose. The lactose, of course, being the major carbohydrate that is contained in dairy. The reason that we're able to metabolize our lactose so very well is because of this very enzyme that we´re seeing, lactase. 01:10 Quickly, physiologically and biochemistry, as we consume our carbohydrate or dairy, we have amylase within our mouth salivary, begins the digestion but obviously does not complete the full digestion. 01:24 In the stomach further, we have acid and such which then further breaks down the carbohydrate. 01:29 By the time we get in to our duodenum, first and second part which is highly, highly concentrated with finger-like projections called microvilli which then you can refer to as being your brush border. 01:41 Literally, the finger-like projections are like your brush borders. 01:45 This brush border then contains a type of disaccharidase, another name for your lactase will be the enzyme that breaks down disaccharide. 01:54 Be smart about how your approach of material. 01:58 Therefore, a lactase is called a disaccharidase which it does exactly as to what the name implies which is to break down your disaccharide. 02:04 Which one is it when we consume milk or dairy? Lactose. 02:08 What if your patient is lactase deficient? Then, you´ve left behind lactose and disaccharide back in your intestinal lumen. 02:17 You´ve now created an osmotic force which is then diffusing water out from your tissue or from the ECF and coming into the intestinal lumen. 02:32 Literally drawing water in and take a look at how much volume you´re losing. 02:38 It´s going to be a large amounts of volume and here you have an osmolar gap greater than 100. 02:47 Stops with fasting and here you might find the pH to be less than 6. 02:54 Welcome to an osmotic diarrhea lactose intolerance. 02:59 The second type is secretory type of diarrhea. 03:03 The ones that you should be quite familiar with or those that are peptide-like. 03:05 For example, the one type of tumor that produces too much serotonin and company would be carcinoid and whenever you think about carcinoid tumor, you should be thinking about residing within the intestines. 03:17 That´s where the carcinoid tumor begins. 03:19 Therefore the type of stool that you are going to examine and which you are examining in the stool would be for your 5-hydroxyindoleacetic acid (5-HIAA). 03:30 One type of secretory, VIPoma, the important acronym here that you will know or should know is WDHA and WD stands for watery diarrhea. 03:42 With all that diarrhea, your potassium levels drop like crazy, the H stands for hypokalemia and then finally, the A stands for achlorhydria but this would be a secretory type of diarrhea. 03:54 Now a far from tumors and including a gastrinoma here, a far from tumors that also produce your secretory diarrhea. 04:00 You can have certain organisms. For example, say that you drink contaminated water that contains the organism, the bacteria, vibrio cholera. 04:08 A Vibrio cholera then works upon your intestinal cell. 04:14 In other base, a lot of membrane cause what's known as ADP-ribosylation if you remember from biochemistry. 04:20 That ADP-ribosylation is then going to insert or open up these chloride channels and lumina membrane and what is it going to do? You've heard of rice water stools. 04:31 This is a secretory type of diarrhea. E. coli, there´s something called 'ETEC'. 04:39 Remember from micro, E. coli could also result in a secretory type of diarrhea. 04:43 You also have laxatives such as Senna and all these may result in secretory. 04:50 Now, here, yes, it´s also large volume stool, however the osmolar gap is not going to be as significant as to what you find with osmotic diarrhea. 05:01 That is important for you to pay attention too and even though your patient might be fasting, it doesn´t matter because this is a secretory biochemical activation. 05:16 Just because you stop eating doesn´t mean the diarrhea stops. 05:20 That is very dangerous 'cause what´s your next step of management. 05:24 That´s a lot of fluid loss that the patient is experiencing so you need to make sure that you do supportive therapy with IV fluids and company. 05:31 Next, we have abnormal motility and here, you should be thinking about dumping syndrome that we have discussed earlier. 05:43 For example during surgery there is every possibility that the pyloric sphincter might be compromised. 05:49 There is an increase of dumping of this chyme into the intestine. 05:53 We´ve talked about the symptoms where there might be things like hypoglycemia and the fact that there is going to be flushing and sweating and tachycardia and company. 06:03 With all those dumping taking place with abnormal motility, you can only imagine that there is going to be a diarrhea. In fact, thyroid issues, increase motility. 06:13 Thyroid issues, hyperthyroidism would cause more or less diarrhea Though we normally associate decreased motility with constipation, in some cases it can cause diarrhea. The mechanism for this is due the bacterial overgrowth, which then subsequently cause diarrhea. 06:29 Exudative. Example for this, inflammatory bowel disease such as ulcerative colitis. 06:34 Infection. Diverticulitis, is exudative. Diverticulitis, we´ve talked about diverticular disease. 06:41 So we'll begin by looking at it by referring to diverticuli and then we'll go into diverticulosis and some point with diverticuli with fecalith accumulating in there. 06:51 My goodness, just a matter of time before your patient goes into state of diverticulitis and as for the inflammatory, that's pretty exudative by the time the stool then comes out. 07:01 Here once again, variable quantity and with exudative think of once again ulcerative colitis which almost always begins in the rectum. 07:09 With all that ulceration taking place and in your stool, then you might be looking for blood.
About the Lecture
The lecture Types of Diarrhea by Carlo Raj, MD is from the course Small and Large Intestine Diseases: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following statements regarding an osmotic type of diarrhea is NOT true?
- Lactase levels are high in patients with this condition.
- The osmolar gap is > 100 in patients with this type of diarrhea.
- Stools are acidic in nature.
- The diarrhea is usually the self-resolving type.
- A large volume of stools is a common complaint.
An elderly woman says that she is unable to pass stools unless she takes laxatives twice daily. What type of diarrhea is expected when laxatives are overused?
- Secretory
- Exudative
- Abnormal motility
- Osmotic
A 30-year-old man picked up food from a take-out restaurant that was selling fried rice, which he consumed later. He presents with nausea, vomiting, and voluminous diarrhea with no change in the osmolar gap. What is the probable cause of his diarrhea?
- B. cereus-induced food poisoning
- Colon cancer
- Lactase deficiency
- Laxative abuse
- Inflammatory bowel disease
What causes diarrhea in patients with decreased intestinal motility?
- Bacterial overgrowth
- Bacterial toxins
- Breakdown of blood in the stools
- Breakdown of bile salts
- Increase in osmolar gap
An ultrasound scan shows a mass at the junction of the 2nd part of the duodenum and the head of the pancreas. The patient, who has increased 5-HIAA in the urine, presents with diarrhea that does not improve with fasting. What is the probable cause?
- Carcinoid syndrome
- Zollinger-Ellison syndrome
- VIPoma
- Crohn's disease
- Small intestine adenocarcinoma
Which of the following is NOT a cause of decreased gastrointestinal motility?
- Carcinoid
- Muscular dystrophies
- Scleroderma
- Hypothyroidism
- Amyloid
Author of lecture Types of Diarrhea

Carlo Raj, MD
Customer reviews
3,5 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
1 |
| 1 Star |
|
0 |
Very strange pauses while speaking, felt condescending at times. Not like his other videos, he seemed not confident in the material
fantastic teaching with instant impact to improve self confidence and boost knowledge
