Playlist
Show Playlist
Hide Playlist
Treatment of Severe Hypercalcemia


-
Slides Hypercalcemia.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
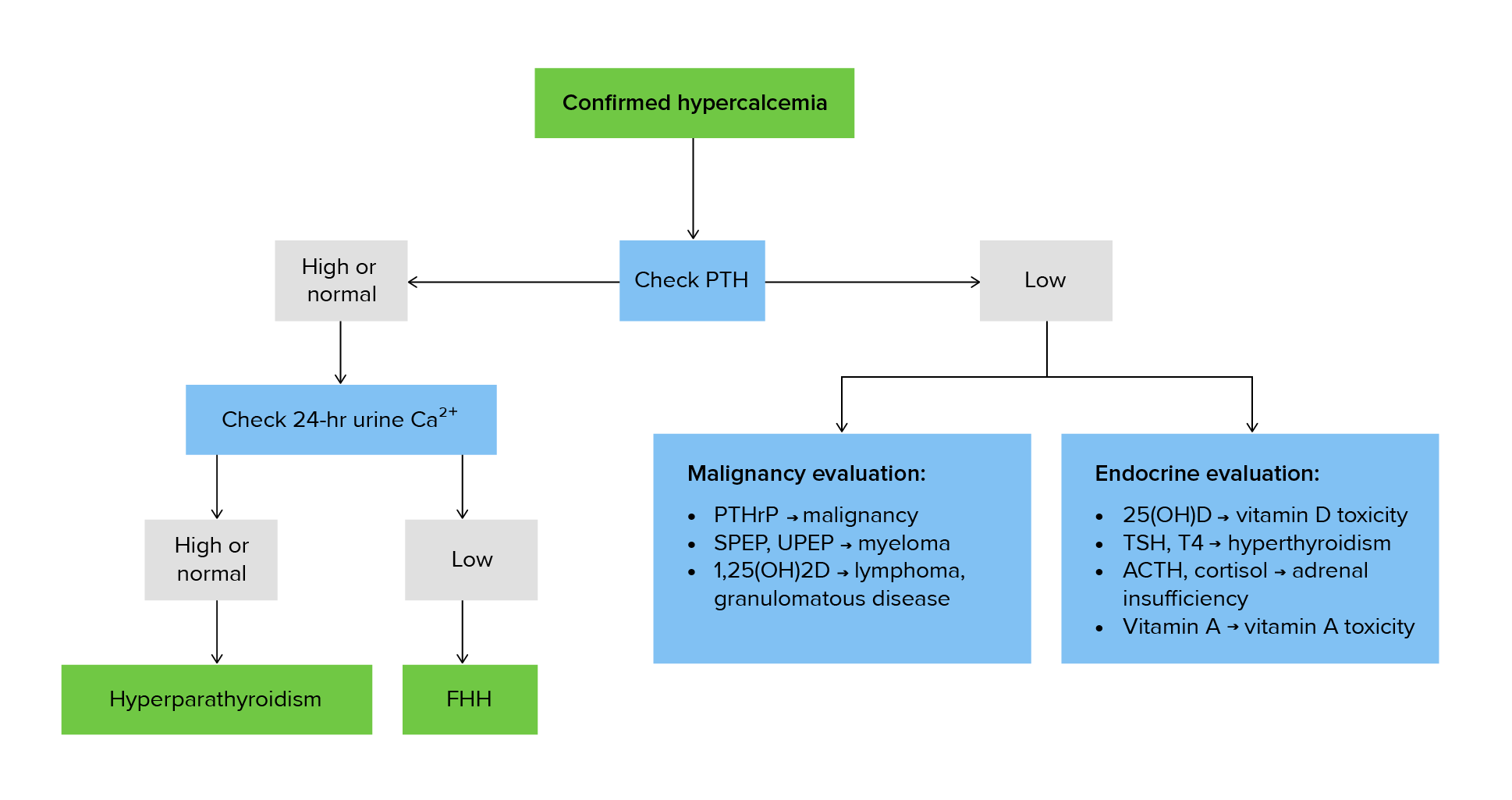
00:01 Severe hyp-hypercalcemia, what do you want to do? Remember, with the severe hypercalcemia, there’s quite a bit of calcium that’s being filtered into the urine. 00:09 Thus may result in osmotic diuresis and kind of like what we talked about earlier with uncontrolled diabetes haemolytis. 00:15 What’s one of the first steps that you’re doing? Replenish, replenish, replenish the fluid. 00:21 Mobilization, if possible. 00:24 Remember, that mobilization, lightweight to a certain extent, may then also help with severe hypercalcemia. 00:34 Bisphosphonates allows for proper mineralization of the bone to remove the calcium out of the circulation, inhibit resorption. 00:43 Effect begins within two days, maximum at a week for bisphosphonates. 00:48 Calcitonin, technically, at this point, it may inhibit bone resorption. 00:55 That’s all that I wish to say about this, but in pathology, please make sure that you keep in mind with calcitonin, parafollicular C cells and use as a marker with medullary cancer of the thyroid. 01:07 Denosumab binds to RANK-ligand, thereby inhibiting the formation of Osteoclasts. 01:12 This, in turn, inhibits bone resorption and reduces the amount of calcium that gets released from the bone. 01:18 Glucocorticoids, effective in Vitamin D-mediated hypercalcemia. 01:24 So, for example, your patient, African-American lady, young, maybe in her early 40’s and she has hypertension and upon chest X-ray, you find these granulomas. 01:34 In addition to that, you find hypercalcemia and glucocorticoids seem to be quite effective in those patients who has sarcoidosis. 01:41 It inhibits the conversion or inhibits calcitriol production in general.
About the Lecture
The lecture Treatment of Severe Hypercalcemia by Carlo Raj, MD is from the course Parathyroid Gland Disorders.
Included Quiz Questions
Bisphosphonates are an important part of the management of hypercalcemia patients. Why should this not be your initial treatment option in a patient with acute hypercalcemia?
- It takes a prolonged time to have an impact on calcium levels.
- It increases osmotic diuresis.
- It can lead to thromboembolism.
- It decreases calcium too quickly in a hypercalcemic patient.
- It inhibits the resorption of bone.
What is the most effective treatment for hypercalcemia for a patient with sarcoidosis?
- Glucocorticoids
- Calcitonin
- Bisphosphonates
- Vitamin D
- Magnesium
Author of lecture Treatment of Severe Hypercalcemia

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
