Playlist
Show Playlist
Hide Playlist
Transpyloric Plane

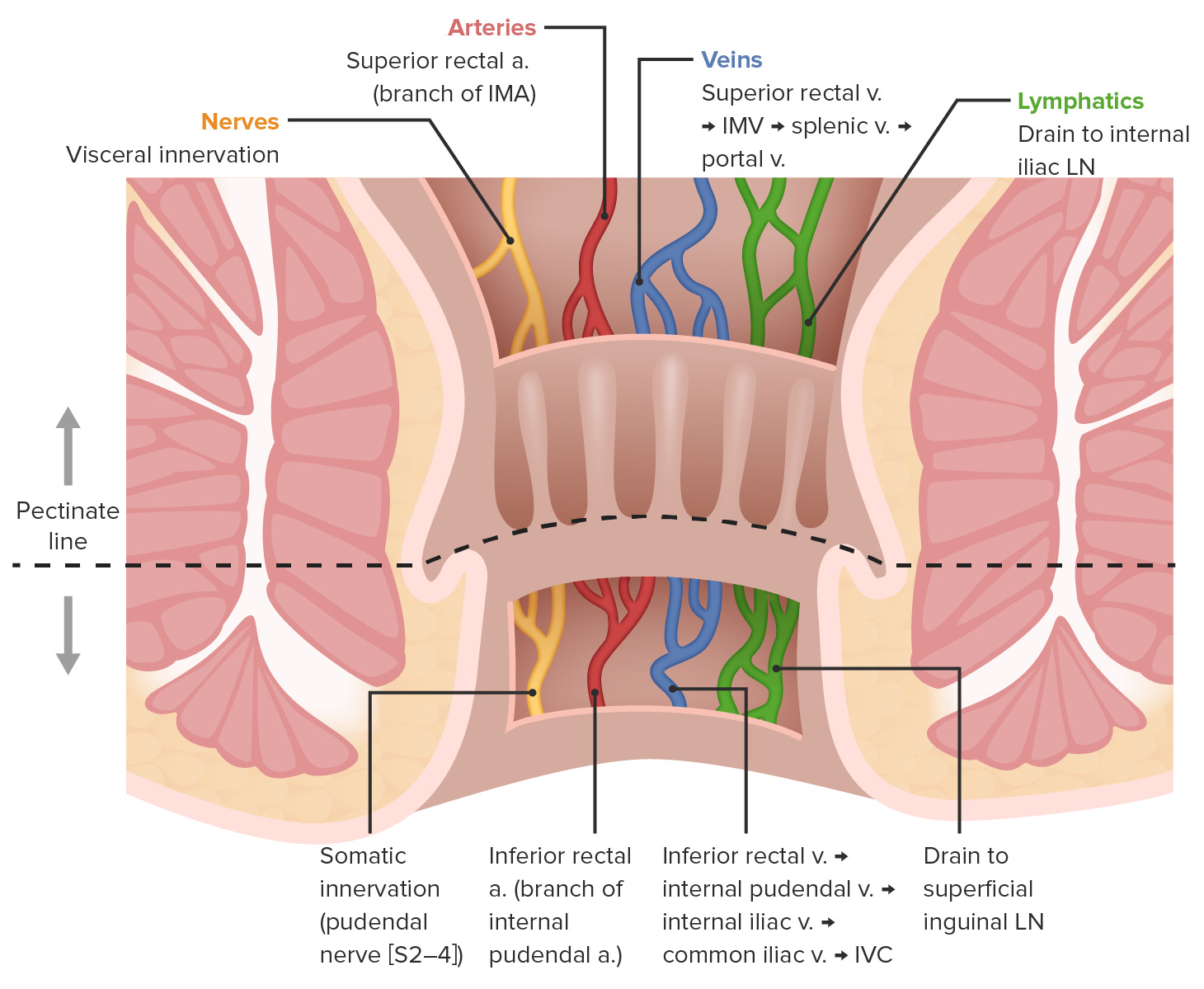
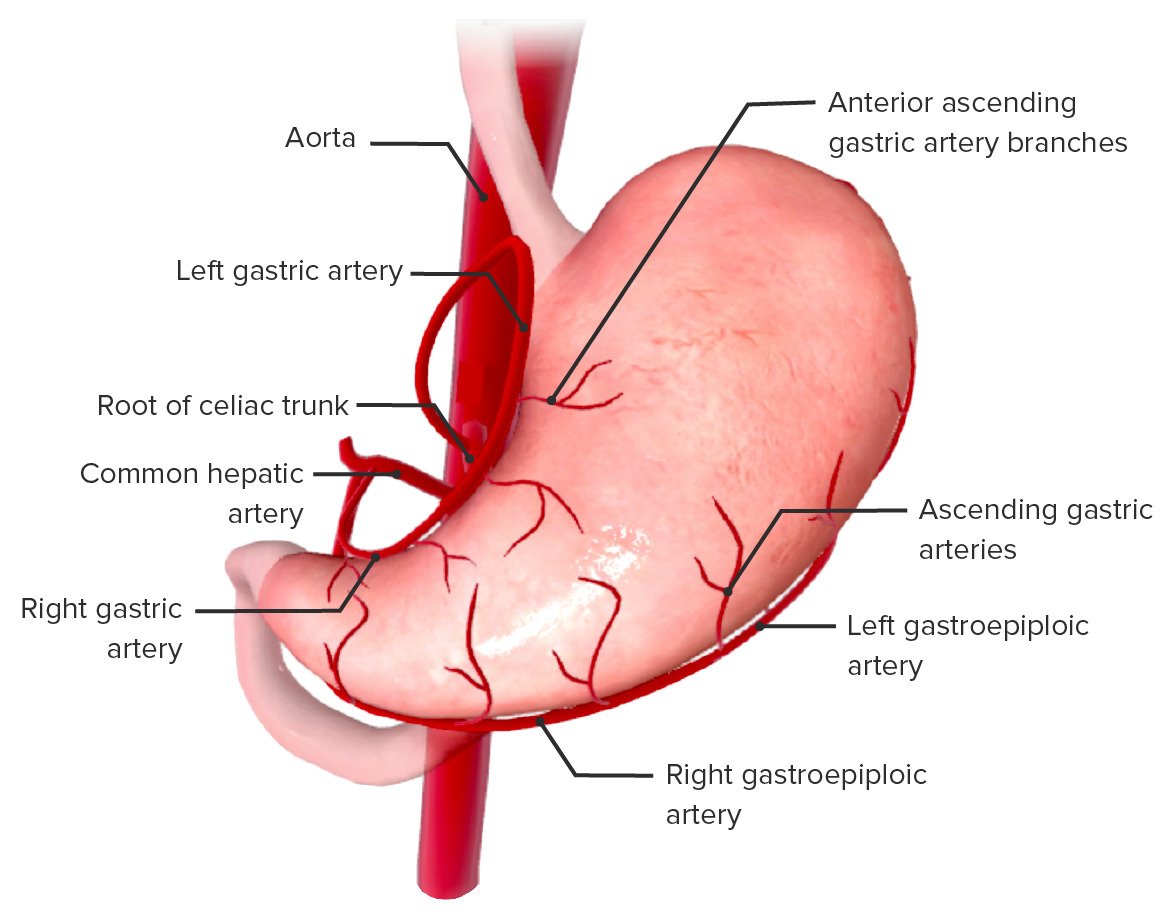
00:00 Going back to the abdomen, I said the T12 vertebal level, your abdominal aorta comes out. 00:20 That's the transpyloric plane. 00:23 The moment the abdominal aorta comes out through the diaphragm, what's the first branch? You're right. Before that, the inferior phrenic. 00:32 That’s the small branch going to the diaphragm, inferior phrenic. 00:35 The next is celiac branch. 00:36 Your MCQ question will be anatomical level of celiac trunk. 00:40 Where does the celiac trunk come from? What anatomical level, vertebral level? Lower border of T12 or upper border of L1. Celiac trunk. 00:52 What are the branches of the celiac trunk? Common hepatic, splenic, left gastric. 01:04 These are the three big vessels coming off the celiac trunk. 01:09 You come a little bit lower down and you come to the transpyloric plane. 01:13 And then you have the superior mesenteric artery coming off the lower border of L1, coming out this way. 01:23 What are the branches of the superior mesenteric? Middle colic, ileocolic, are you feeling cold? Which one? Right colic, okay. 01:44 In the exam, you shouldn't be thinking so much because it's very simple logic. 01:49 Your celiac trunk is the artery of the foregut. 01:54 Where does the foregut stop and where does the midgut begin? The second part of the duodenum. 02:01 What's the anatomical landmark there? No. The ampulla of vater. 02:07 The pancreatic duct and the bile duct open into the ampulla of vater. 02:11 That is your anatomical landmark for the cut-off between your foregut and the midgut. 02:19 Foregut essentially means your spleen, liver, stomach, and first part of the duodenum. 02:28 All these will have to be supplied by celiac trunk hence your blood supply to the stomach has to be from branches from the celiac trunk. 02:40 Don't think of anything more than that because it has to be from the celiac trunk. 02:43 What are the blood supply to the stomach? Just name the big vessels. 02:46 Left gastric, gastroepiploic, so the right and the left gastroepiploic, left gastric and the right gastric, and short gastric arteries. 02:55 They're all mainly coming from the celiac trunk. 03:01 Then you go to the superior mesenteric territory, superior mesenteric arteries are artery of the midgut. 03:08 Where does the midgut stop, end? The lateral 2/3 of the transverse colon, so somewhere around there. 03:16 This much are the transverse colon, ascending colon, cecum, appendix, iloecolic junction, whole of the ileum, jejunum. 03:27 They're all supplied by the SMA territory. 03:29 You can just remember the names now. 03:33 You can remember jejunal arteries, ileal arteries, ileocolic arteries, cecal artery, appendicular artery, right colic and middle colic. 03:45 All this will be from the superior mesenteric. 03:49 You also have the inferior pancreaticoduodenal. 03:53 Remember this part of the duodenum? That is also belonging to the midgut. 04:01 This is supplied by the inferior pancreaticoduodenal artery. 04:06 If you’re asked names, that's all you need to remember. 04:11 Staying on the gut, foregut, midgut and the hindgut is supplied by the inferior mesenteric. 04:18 If this comes down a bit further down L1, that’s L2. 04:25 What do you get in L2? What arises at L2? Renal arteries. When you listen for renal bruit, this is the vertebral level you need to be listening for, renal arteries, paired renal arteries. 04:40 What else do you get? Gonadal, gonadal, testicular or ovarian artery, paired testicular gonadal arteries going down that way. 04:50 That is lower border of T2, sorry, L2. 04:53 Then you come down L3, you have the inferior mesenteric. 04:59 Name some branches from the inferior mesenteric. 05:03 Left colic, superior rectal, and no, inferior rectal is not, sigmoid. 05:12 Three vessels. This part, left colic, sigmoid, and the superior rectal artery. 05:23 That part is quite significant. 05:25 What does the superior rectal artery supply and what is the clinical significance of you knowing that both operative-wise as well as for exam? Yes. Well, the superior rectal artery supplies the whole of the rectum, doesn't it? It supplies the whole of the rectum and up to the dentate line of the anal canal. 05:49 Beyond that is supplied with the middle rectal and the inferior rectal. 05:53 Surgically, that's relevant because when you do an anterior resection, that's the territory you go for, the dendate line. 06:03 If you do an abdominoperineal resection for a lower rectal cancer or anal tumor, then you may have to excise the whole thing because you are going to the different territory. 06:13 Another significance is portal venous anastomosis. 06:21 Since we are here, I’ll just go through that in detail because portosystemic anastomosis is important. 06:27 What are the sites of portosystemic anastomosis, sites of portosystemic anastomosis in the abdomen? For example, if somebody's got portal hypertension ascites, where are they going to bleed from? Hematemesis, melena, rectal varices, yes, that’s melena. 06:53 And then what else do you get? Caput medusae. 06:56 What are these? What is happening here? Why do you get all this? Yes, with the system of circulation. 07:13 Yes. Which vessels? Let me ask you this? Putting it in a different way, hematemesis and then you go in endoscopically to ligate those vessels. 07:25 Which vessels do you think are bleeding in portosystemic anastomosis? Yes, I guess, yes. 07:34 In your exam, you need to know which is a portal circulation and which is a systemic circulation. 07:41 To understand that, you need to understand the arterial supply first which will be very easy for you to understand.
About the Lecture
The lecture Transpyloric Plane by Stuart Enoch, PhD is from the course Upper Part of the Body Anatomy.
Author of lecture Transpyloric Plane

Stuart Enoch, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
