Playlist
Show Playlist
Hide Playlist
Differential Diagnoses & T3-Resin Uptake – Euthyroid Conditions

-
Slides EuthyroidConditionsLaboratoryInvestigations EndocrinePathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
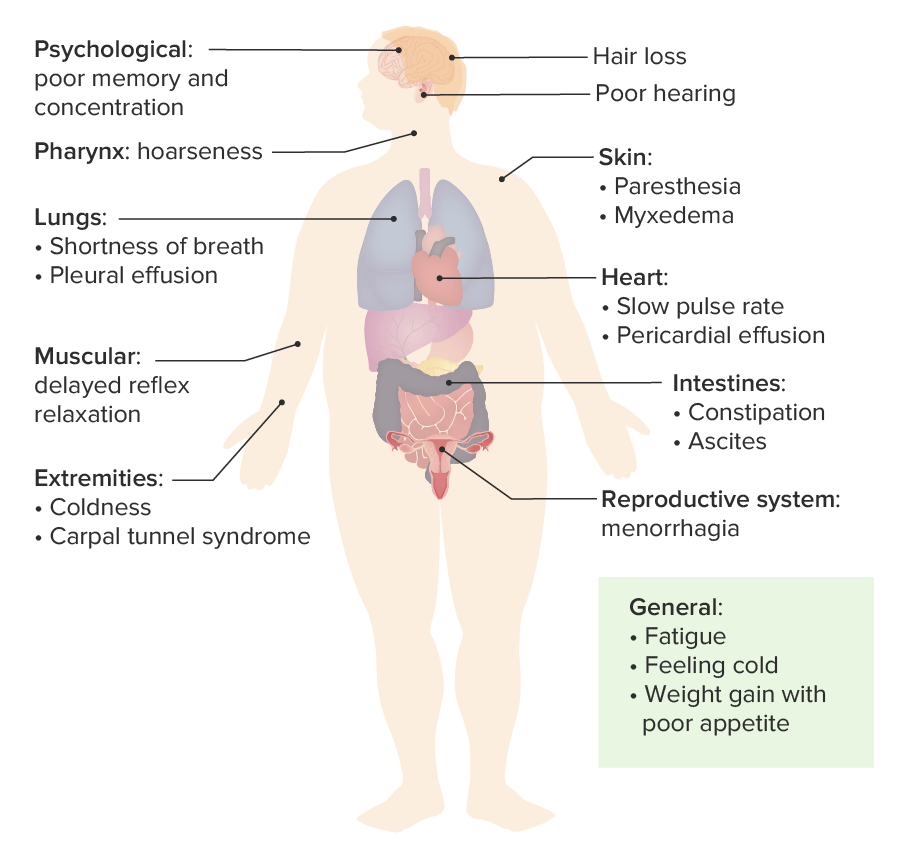
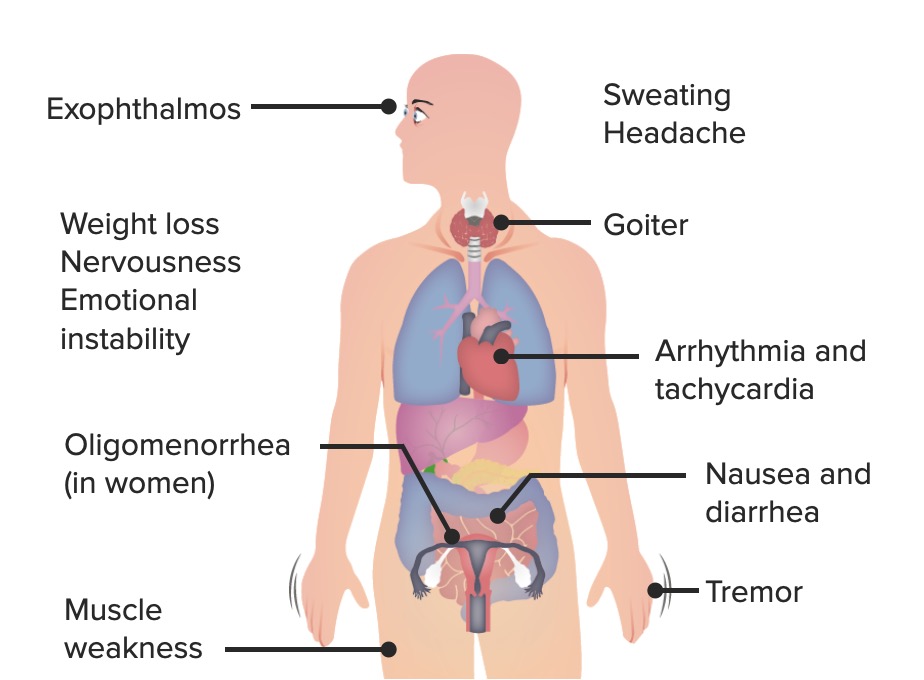
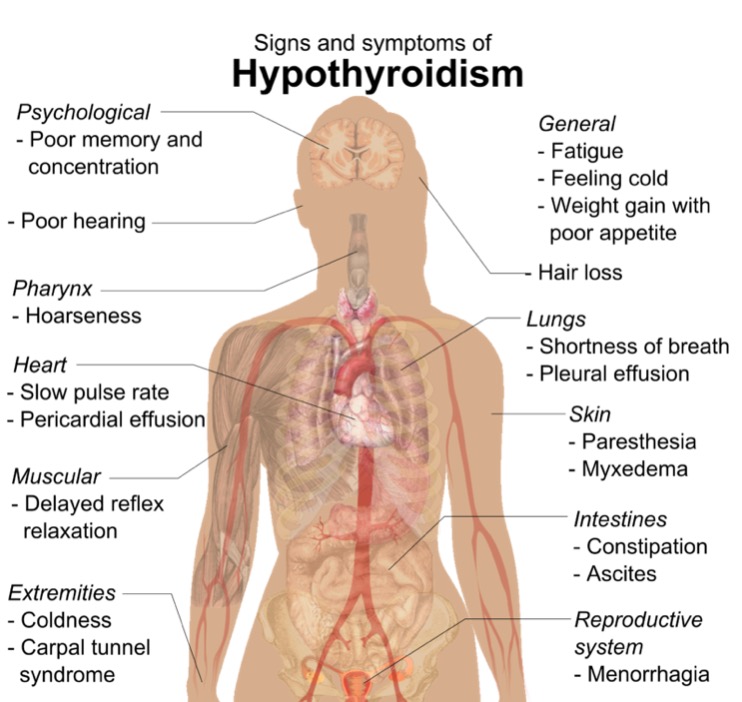
00:01 Diagnosis – hyperthyroidism, hypothyroidism. 00:05 Stop there. 00:07 We haven’t gotten into great detail, specifically of Graves’ disease or Hashimoto to give you an example of hyper/hypothyroidism, but what we have done in this discussion is talk about TBG excess and TBG deficiency. 00:24 At this point, I need you to focus upon the bottom two differentials. 00:27 In addition, the topic is differential diagnosis in summary of results of T3-resin uptake. 00:37 Stop. 00:38 Resin. 00:39 Picture that. 00:40 I’ve shown you resin. 00:42 What is it going to bind to? T3. 00:46 Do not confuse the resin with your TBG. 00:50 Where’s thyroglobulin bind to? T4. 00:55 What you’re going to be using, as a clinician, is the T3-resin uptake to give you further confirmation for your diagnosis. 01:03 Is that understood? None of this would make any sense to you, unless you’ve understood the discussions that we had prior. 01:11 In TBG excess, think about a common example – pregnancy and estrogen. 01:16 TBG deficiency – drugs that displace the T4 from your TBG or heparin that I showed you earlier that increases lipoprotein lipase activity. 01:26 That increasing free fatty acid inhibits the binding of T4 to TBG. 01:33 Those are your differentials. 01:34 Let’s move on to next column. 01:37 If it is pure hyperthyroidism, we know that the serum free T4 index is increased. 01:47 Example – Graves’s disease. 01:50 Graves’ disease. 01:52 Hypothyroidism – as a differential –Hashimoto. 01:57 We know that the free T4 index is decreased. 02:02 The topic for this entire section was what? It wasn’t hyper or hypo. 02:08 It was euthyroid. 02:10 When you say euthyroid, what does that mean? Take a look. 02:15 Either TBG excess or TBG deficiency showing you what with free T4? Notice. 02:23 Normal. 02:24 Normal. 02:25 What’s the clinical representation of normal? Eu-. 02:32 Eu-. 02:33 So, how can you possibly tell what’s causing the normal, but yet resulting in hyperthyroxinemia or hypothyroxinemia? Let’s take a look at it further. 02:47 Serum total T4 is my third column. 02:51 What’s total mean to you? Bound versus free. 02:55 In hyperthyroidism, we can for sure expect there to be more T4, thus, there will be more bound; therefore, total is increased. 03:06 I want you to skip down to TBG excess. 03:10 In TBG excess, we talked about estrogen. 03:13 We talked about increased thyroglobulin. 03:16 What is it doing? It’s binding to more T4. 03:20 If your bound is increased, what about the total? Voilà! Increased serum total T4. 03:29 How can you confirm and how can you differentiate between the two? Give me a second. 03:34 Take a look at the hypothyroidism with decreased T4, obviously decreased bound. 03:41 You’ll have decrease in total T4, whereas if you have TBG deficiency, you have less of your T4 that is bound, because you have less TBG and you have decreased total T4. 03:54 This now brings us to our last and final column that I’ve highlighted in red for you. 04:00 What this is showing you is that resin and this is how you’re going to interpret and differentiate one type of pathology from another. 04:09 The T3-resin. 04:10 So, that’s what the resin is binding to. 04:13 And this is then referred to as your thyroid hormone binding resin. 04:16 If it’s hyperthyroidism, with all that increased T3 and T4 you can expect there to be more T3 bound to my resin. 04:24 It is increased. 04:26 Skip down to TBG excess. 04:29 Now, this is where you want to pay attention and this is where you’re going to take all that information that I’m giving you and put it all together. 04:37 That TBG excess, give me your differential. 04:39 Number one differential. 04:40 Estrogen excess. 04:41 Why? Oh, pregnancy or contraceptive pill, what have you. 04:44 There’s something going on with the liver that you have increase in TBG. 04:47 Let’s move a little bit faster now. 04:49 That TBG excess is bound to whom? T4. 04:53 T4. 04:54 T4 What happens to your total? That’s increased. 04:58 Take a look at hyperthyroidism. 05:00 The first row and the third row. 05:03 TBG excess. 05:04 Both of those are increased for total. 05:05 How can you differentiate between the two? In hyperthyroidism, that T3 will be bound to resin in increased amounts, whereas why is it that it’s decreased with TBG excess? Because all that T4 is now then bound to my TBG and now, at this point, you’ll have less T3 that is now available to bind to your resin. 05:36 So, if you have T3 resin uptake, that’s decreased in TBG excess. 05:42 Let’s take a look at T3-resin with hypothyroidism and TBG deficiency. 05:48 In hypothyroidism, think of Hashimoto, you have less T3 bound to the resin. 05:54 It’s decreased. 05:55 In TBG deficiency, you have less T4 that is then bound to TBG. 06:01 You have more T3 that is available to then bind to my resin. 06:06 At this juncture, with that fourth and final column, it would behove you to go back to those previous illustrations that I showed you, where you can clearly see with TBG deficiency more T3 bound to the resin, whereas if it’s TBG excess, you have less T3 available to bind to your resin. 06:24 How important is this? Critical. 06:27 This is going to work for you on every single board exam that you can think of and as you walk into your residency program, you are interpreting this for the attending who will never pimp you ever again.
About the Lecture
The lecture Differential Diagnoses & T3-Resin Uptake – Euthyroid Conditions by Carlo Raj, MD is from the course Thyroid Gland Disorders.
Included Quiz Questions
Which condition is characterized by an increased free T4, increased total T4, and increased T3 resin uptake?
- Hyperthyroidism
- TBG excess
- Hypothyroidism
- TBG deficiency
- Euthyroid hypothyroxinemia
Which condition is characterized by a decreased free T4, decreased total T4, and decreased T3 resin uptake?
- Hypothyroidism
- Hyperthyroidism
- TBG deficiency
- TBG excess
- Euthyroid hyperthyroxinemia
In TBG excess, what will be the values of T3 resin uptake and hyperthyroidism, respectively?
- Decreased; increased
- Increased; increased
- Decreased; decreased
- Increased; decreased
- Decreased; no change
In TBG deficiency, what are the values of T3 resin uptake and hypothyroidism, respectively?
- Increased; decreased
- Increased; increased
- Decreased; decreased
- Decreased; increased
- No change; decreased
Author of lecture Differential Diagnoses & T3-Resin Uptake – Euthyroid Conditions

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Very clearly explained! Dr Raj is a wonderful professor. Thank you!
