Playlist
Show Playlist
Hide Playlist
Seizures (Emergency Medicine)

-
Emergency Medicine Bord Seizure.pdf
-
Download Lecture Overview
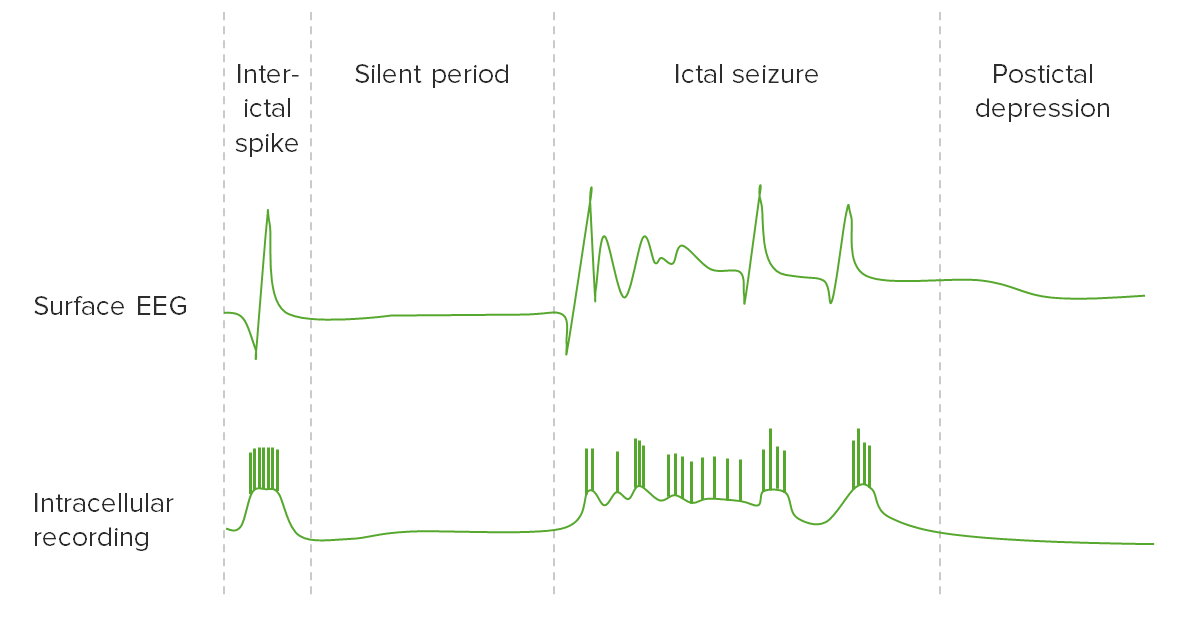
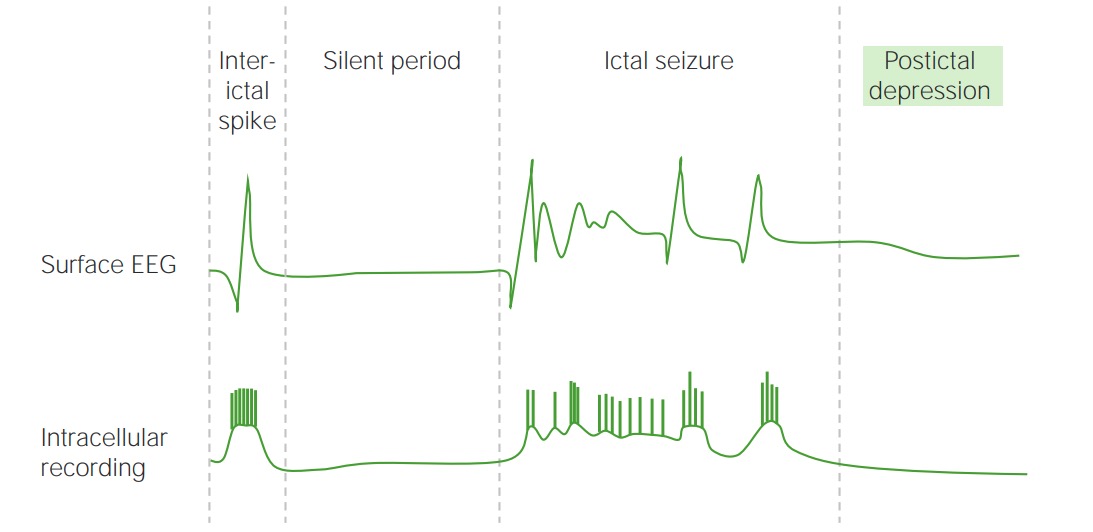
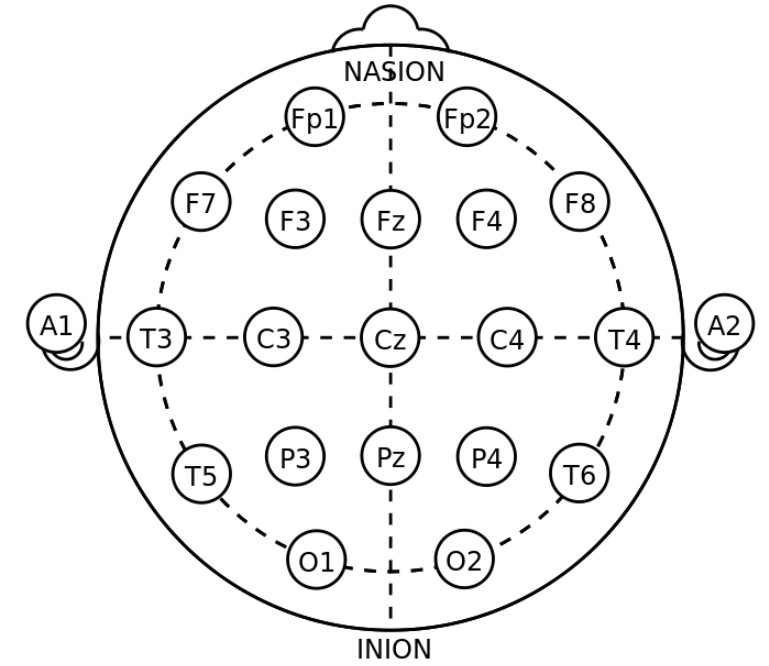
00:01 Hi, we’re gonna be talking about patients who present with seizures and how to manage them in the Emergency Department. 00:09 So what is a seizure? A seizure is when there is excessive abnormal neuron activity. 00:15 Seizures can be divided into three large groups. 00:18 A person can have a partial seizure which is also known as a focal onset seizure, a generalized seizure or a seizure of unknown onset. 00:26 Just some definitions before we get started. 00:29 So the ictal period is the time when the actual seizure is occurring. 00:34 So this is the time that the patient is having or undergoing that seizure activity. 00:40 The post-ictal period is a period of altered mental status following a seizure. 00:45 A post-ictal period can range in time anywhere from about 10 or 15 minutes up to hours or possibly even a day. 00:53 Status epilepticus is when a patient has seizure activity for more than 5 minutes, or a patient has recurrent seizure activity. 01:02 So they have another seizure without a return to baseline mental status. 01:06 The reason that it’s important to mention status epilepticus is because for those patients, you wanna make sure that you treat the seizures aggressively. 01:14 Because as time goes on and as the patient has consistent or continuous seizure activity, that can lead to an increased metabolic demand for the brain and in turn, can eventually lead to brain damage. 01:27 So we wanna make sure that we’re paying attention to how long a patient is seizing for and whether or not they're having another seizure before they turn back to their neurologic baseline, because in those patients, you wanna make sure that they’re treated more aggressively. 01:41 Epilepsy is an unprovoked seizure. 01:44 So that’s a seizure due to no provoking factor. 01:47 Sometimes it can be due to underlying structural issues in the brain. 01:53 Focal onset seizures can be further classified based on the patients level of awareness. 01:58 The earliest detectable sign of behavior during a seizure or both. 02:02 These two levels of classifications are not higher article or mutually exclusive. 02:07 These terms can be added or excluded based on the information available about each specific patient. 02:13 Within the focal onset category, seizures can be classified as focal aware, or focal impaired awareness types. 02:20 These terms correspond to the old terms, simple partial and complex partial seizures. 02:26 Additionally, seizures can be classified as a focal onset seizure with any of several motor or non-motor signs and behaviors. 02:33 Some motor types include automatism, when patients perform coordinated, purposeless, repetitive actions such as suckling. 02:41 Other motor types are atonic, tonic, clonic and myoclonic. 02:46 Some non-motor types include behavior arrest, cognitive and emotional. 02:51 The category of generalized onset seizure is very similar to that of the previously used classification of 1981. 02:58 It does not use level of awareness as a distinguishing factor, because awareness is usually impaired in all generalized seizures. 03:06 Instead, these seizures are only classified in the generalized onset motor or non-motor seizures, based on the types of movements performed. 03:14 The classic tonic-clonic seizure previously called grand mal, is characterized by alternating episodes of generalized stiffening of the body, and sustained rhythmic jerking motion. 03:25 Generalized myoclonic seizures can occur in isolation in combination with tonic or clonic activity, with both or atonic activity. 03:34 Atonic seizures are usually characterized by a lost of leg tone. 03:39 Because all generalized seizures initially involve losing leg tone, atonic seizures can be distinguish because the patient usually falls on their buttocks, or into their knees or face. 03:49 All other generalized seizures usually make the patient fall backward. 03:53 Generalized non-motor seizure types includes several varieties of absent seizures. 03:58 And absent seizure is characterized by a sudden onset interruption of ongoing activities. 04:03 A blank stare, impossibly a brief upward deviation of the eyes. 04:08 An EEG maybe required to distinguish between atypical and typical absent seizures. 04:13 Finally, seizures of unknown onset can be motor or non-motor. 04:18 The term unknown onset is usually used in cases where the beginning of a seizure was obscured or not witness by anyone. 04:25 These seizures are usually reclassified when the patient experiences another seizure while under observation. 04:32 Who primarily gets seizures or presents to the hospital with seizures? There's a bimodal life distribution. 04:39 So infants and young kids primarily will have febrile seizures. 04:44 These are seizures that are related to generally higher temperatures. 04:48 For the most part, they’re benign in nature and often times do not recur, although sometimes they do. 04:55 The other age of range are older people. 04:58 So patients who are greater than 75 years of age. 05:01 So you wanna think about the seizures or you know who presents with them are the young and the old. 05:06 There’s definitely a lot of people in the middle as well but those are kind of the biggest groups. 05:11 Recurring seizures occur in about half of patients with epilepsy. 05:15 So those patients may recurrently have these episodes.
About the Lecture
The lecture Seizures (Emergency Medicine) by Sharon Bord, MD is from the course Neurologic and Psychiatric Emergencies.
Included Quiz Questions
What most accurately defines status epilepticus?
- 5 minutes or more of continuous seizure activity or more than one seizure without recovery.
- 10 minutes or more of continuous seizure activity.
- More than two seizures without recovery in between.
- 10 minutes or more of continuous seizure activity or more than two seizures without recovery in between
- Alternating focal and generalized seizures with recovery in between the seizures.
Which statement regarding seizures is FALSE?
- Infants primarily develop absence seizures.
- Recurrent episodes occur in approximately 50% of the patients with primary seizures.
- Partial seizures can be simple, complex, or secondarily generalized.
- Absence, myoclonic, and tonic are examples of generalized seizures.
Author of lecture Seizures (Emergency Medicine)

Sharon Bord, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
