Playlist
Show Playlist
Hide Playlist
Seizure: Diagnosis

-
Emergency Medicine Bord Seizure.pdf
-
Download Lecture Overview
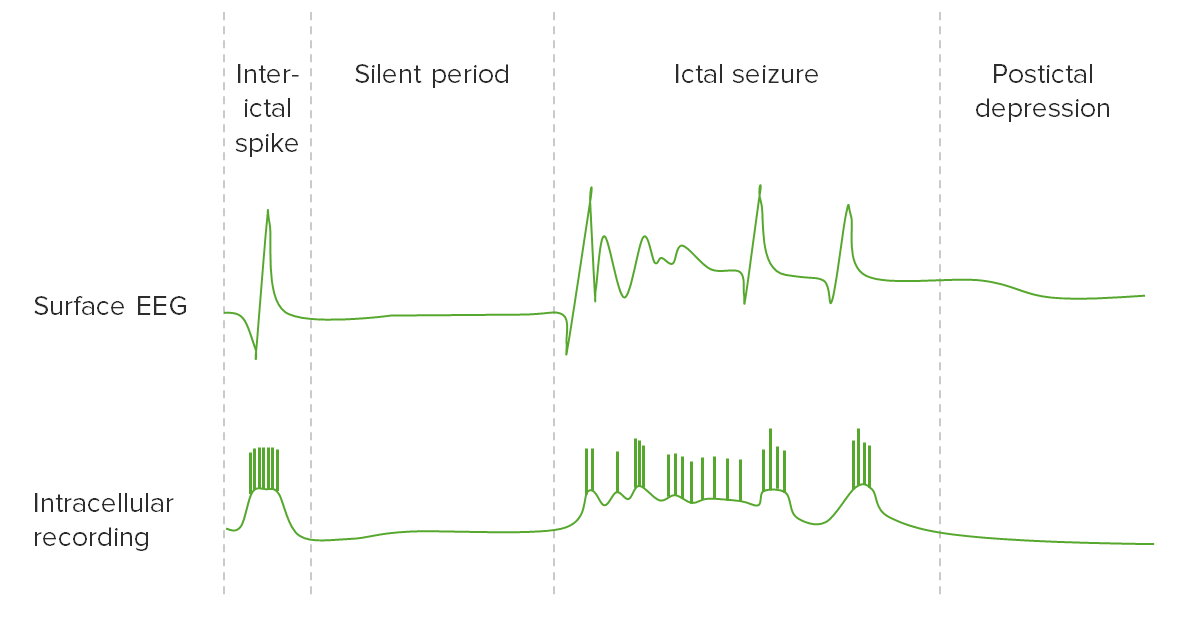
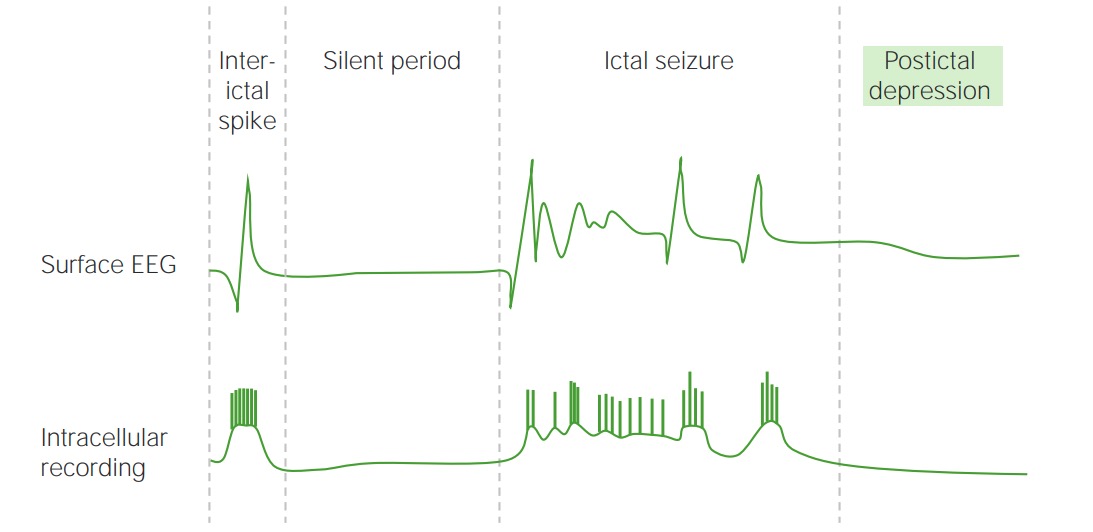
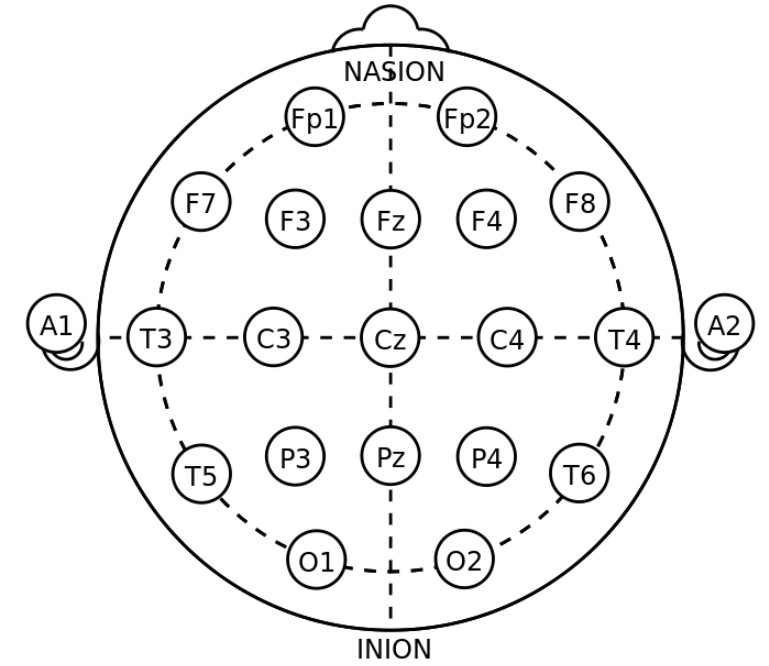
00:01 Now, other things on the differential here, with the big thing that we try to distinguish seizure and syncope. 00:09 So did they have an episode where it was the seizure or did they have a syncopal episode where they passed out? There can sometimes be convulsive activity associated with syncope. 00:19 This is one of those situations where it’s very important to try and talk to someone else who saw the event, someone else who witnessed it. 00:26 If someone does have that convulsive activity associated with syncope, that's most commonly associated with bradycardia, so that the patient were gonna have a low heart rate. 00:36 Now, a big way that you can distinguish syncope from seizure, few big ways are that syncope, the patient doesn't have post-ictal confusions. 00:45 So they don't have that period of time after the event where they're confused. 00:48 They also generally don't have the bigger tonic-clonic movements. 00:52 So the convulsive activity that you'll see with syncope is generally a little bit minor than the bigger movements. 00:57 And then again, syncope should not be associated with incontinence of urine or stool and syncope generally patients do not have trauma to their tongue or their mouth. 01:06 So those are other ways that you can distinguish those two entities. 01:10 Another component on the differential diagnosis is something called Psychogenic seizures and what this basically is, is that the seizure doesn't come necessarily from the brain tissue itself. 01:20 Now, this is a complicated entity, it can be challenging to distinguish from a true seizure disorder. 01:27 There's a few ways that the neurologist use using various lab tests, but for the most part, it can be hard to distinguish, is this a seizure, a real seizure, or is this a psychogenic seizure? So a seizure related to an underlying psychiatric process. 01:44 And then the last big important thing here is alcohol withdrawal seizures and it's alcohol withdrawal and also possibly benzodiazepine withdrawal seizures. 01:53 Alcohol withdrawal can be actually quite fatal and can be very, very serious. 01:58 So if your patient had a history of alcohol user abuse or benzodiazepine user abuse and they have not taken those medications for a period of time or you’re unsure if they have, and they come in with seizure activity, then you wanna definitely start thinking about this, and you wanna make sure that you treat it early and you treat it aggressively. 02:17 Patients who have alcohol withdrawal will classically have an elevated heart, an elevated blood pressure, and also when they're not having a seizure event will be tremulous as well. 02:28 So let's say your patient presented with the first time seizure and they've never had a seizure before. 02:34 The work up for those patients are you wanna check a finger stick glucose. 02:38 Hypoglycemia is a common thing that can cause a seizure, so you wanna make sure you’re always checking that glucose level. 02:46 The other common electrolyte abnormality that's associated with seizure is a sodium level. 02:52 So hyponatremia or a low sodium can cause seizures as well. 02:56 Now, if you have hyponatremia related seizures, you wanna make sure that you check that level and that you increase that sodium level appropriately. 03:06 A pregnancy test, preeclampsia or rather eclampsia can lead to seizures. 03:12 So sometimes patients present with the big gravid belly when their, you know, in later pregnancy, but every so often you have a patient that doesn't necessarily have that. 03:22 So if you know, if you're not sure if your is pregnant and you're worried, you wanna start thinking about eclampsia as a possibility. 03:29 So always check a pregnancy test. 03:30 And then, a non-contrast head CT would be the last thing. 03:34 And the non-contrast head CT is to evaluate for mass or possibly a bleed. 03:38 You know that's a little bit debatable but for the most part you wanna make sure you're thinking about doing that non-contrast head CT or the very least discussing it with a neurologist. 03:50 The other big thing that does sometimes cause first time seizures are toxicologic substances. 03:55 So you wanna consider sending a tox screen or an alcohol level for those patients. 04:00 The other thing that's important is to really try and get a history from them as to whether or not they took any illicit substances or potentially even some over-the-counter or prescribed medications can also lead to seizures. 04:14 So getting a history on any kind of new medications that a patient maybe on is very important here and sending this blood test can potentially help you. 04:23 So what other testing do we wanna do? For patients who have a known seizure disorder, you wanna send medication levels if you're able to level their medications. 04:32 You wanna get an EKG, which will look for toxins, it can sometimes alter the EKG. 04:39 It can look for abnormal rhythms, if you're trying to distinguish was this a syncopal episode or was this a seizure, it can go ahead and look for that. 04:48 And it can also look for ischemia, very rarely someone could be presenting with a myocardial infarction and their presenting thing could be that they're having a seizure actually. 04:59 So it's rare but it definitely can happen, so getting an EKG can be beneficial. 05:05 You wanna consider a lumbar puncture if your patient has a persistent fever. 05:09 If they have a headache or if they have persistently altered mental status. 05:14 That post-ictal period should last on average between 15 minutes to a few hours, if it last for a longer than that or you have other concerns that's when you wanna start thinking about doing that lumbar puncture. 05:28 The last thing to think about doing for these patients in the Emergency Department is an EEG. 05:34 An EEG is a neurologic test where they put a lot of stickers on the patient's head and they hook it up to wires and they look to see if the patient is having seizure activity in their brain. 05:45 The times that you might wanna do this, is if you're worried that your patient is having persistent seizure activity. 05:50 This is often times done for the very sick patient who has status epilepticus, who has those recurrent seizures especially in a situation if you've sedated them and had to intubate them and put them on a breathing machine. 06:02 Those patients can be very hard to see if they're having underlying seizure activity on the outside. 06:07 So getting the EEG can see if they're having underlying seizure activity in their brain itself.
About the Lecture
The lecture Seizure: Diagnosis by Sharon Bord, MD is from the course Neurologic and Psychiatric Emergencies.
Included Quiz Questions
Which of the following is MOST suggestive of a seizure episode?
- Postictal confusion
- Triggered by prolonged standing or emotional stress
- Orthostatic hypotension
- Loss of consciousness with exertion
Which of the following is the most appropriate immediate step in the diagnostic workup of an adult who presents with a first episode of seizure?
- Finger-stick glucose test
- Cardiac stress test
- Brain magnetic resonance imaging
- Positron emission tomography scan
- Brain computed tomography scan
Which of the following is LEAST appropriate in the immediate evaluation of a patient who presents to the emergency department with a seizure?
- Contrast-enhanced computer tomography scan
- Finger-stick glucose test
- Serum beta hCG
- Medication history
- Serum sodium levels
Author of lecture Seizure: Diagnosis

Sharon Bord, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Fantastic overview and the differential between seizure and syncope. The visual graphics are very helpful.
