Playlist
Show Playlist
Hide Playlist
Renal Case: 52-year-old Man with Depression

-
Slides Water Balance Hypo and Hypernatremia.pdf
-
Reference List Nephrology.pdf
-
Download Lecture Overview
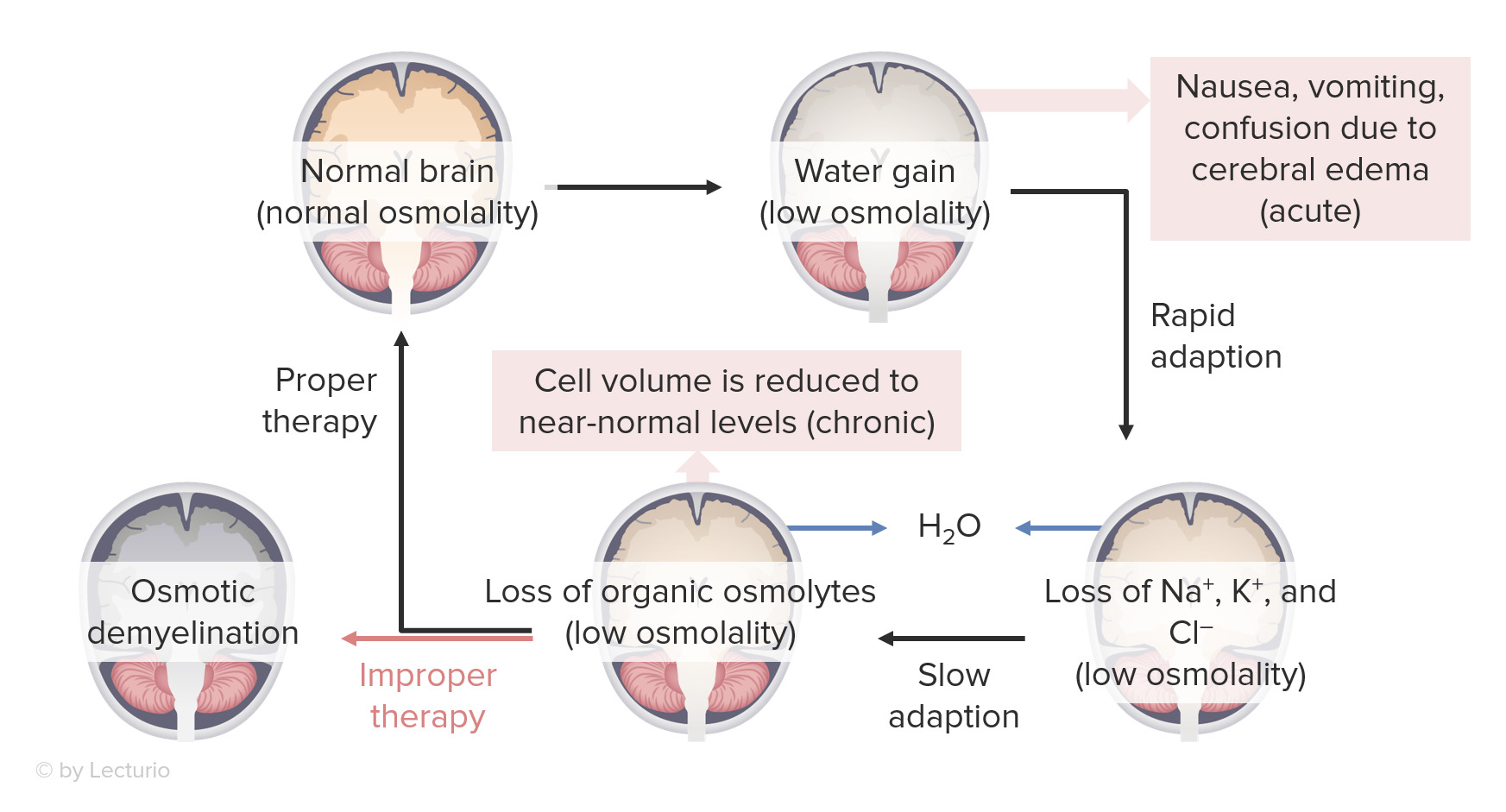
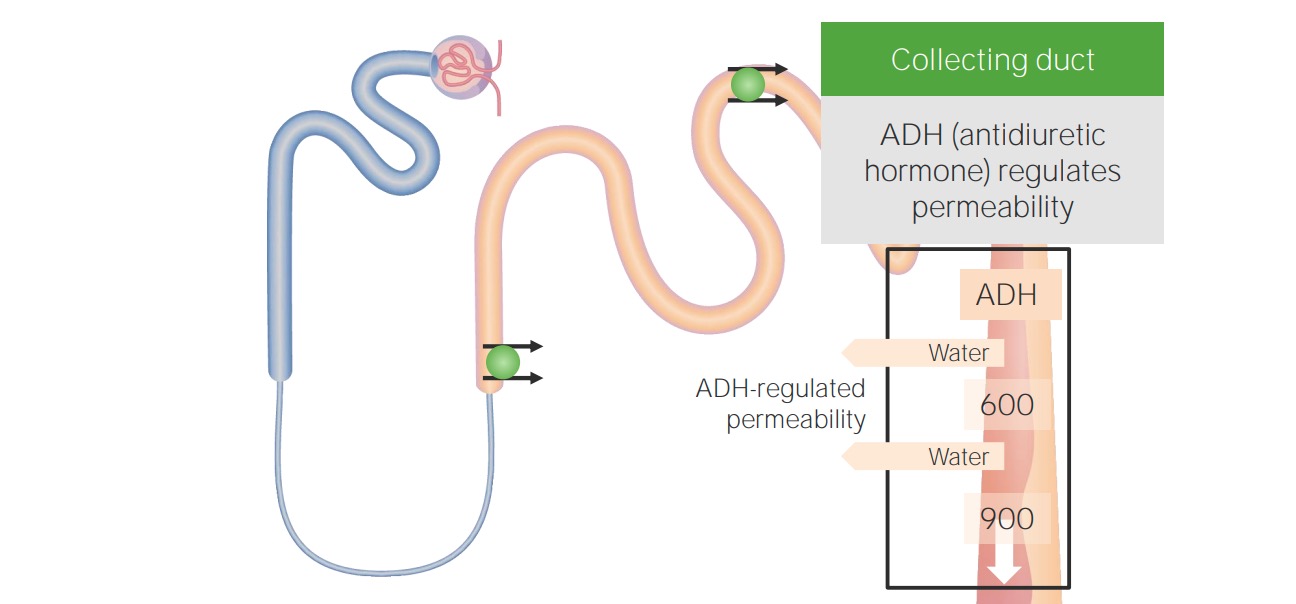
00:01 Let's run through another case. 00:02 So a 52-year-old man with depression was recently started on a Selective Serotonin Reuptake Inhibitor for his depressed mood. 00:10 Although, he has experienced an improvement in his mood, which is great. 00:14 He also has been feeling a little bit nauseated and slightly confused. 00:18 He's taken to the emergency department and on evaluation his serum sodium is noted to be 122 mEq/L. 00:26 He is normotensive on exam and he's noted to have a normal jugular venous pressure. 00:31 His serum osmolality is 260 mOsm/kg. 00:36 His urine osmolality is high at 600 mOsm/kg, and his urine sodium is 42 mEq/L. 00:45 So which statement is true regarding this gentleman's hyponatremia? Letter A. 00:50 There is appropriate ADH release due to a hypovolemic state. 00:55 Letter B. 00:55 This is due to translocational hyponatremia. 00:59 His total body water stores are unchanged, but there is a tonic effect from his SSRI that moves water from the intracellular to the extracellular compartment. 01:08 Letter C. 01:09 There is appropriate ADH release due to a low circulating arterial blood volume despite his hypervolemia. 01:15 Or letter D. 01:16 There is inappropriate ADH secretion or SIADH. 01:21 Let's go through our history and see if we can get some clinical clues. 01:24 So once again, remember our steps that we want to do. 01:27 Step one, we're determining the plasma osmolality. 01:30 Here we can see he actually is hypoosmolar. 01:33 His plasma osmolality is 260 mOsm/kg. 01:37 He is hypotonic. 01:38 So the next thing we want to do when we have a true hypotonic hyponatremia is determine the volume status. 01:45 And look at his exam. 01:46 He has normal neck veins. 01:48 He is normotensive. 01:49 So he is euvolemic on exam. 01:52 The third step is we want to evaluate the presence or absence of ADH. 01:56 The way we do that is by looking at the urine osmolality. 01:59 Here you can see, he has a very concentrated urine or a high urine osmolality. 02:03 It's higher than a serum osmolality. 02:05 That means that ADH is present. 02:08 And step four, we want to evaluate if the Renin-Angio-Aldo-System is activated. 02:14 Here we see that as urine sodium is actually greater than 20 milliequivalents, so it's actually in the 40s, this means that RAAS is suppressed. 02:24 So let's go through our answers. 02:27 Letter A. 02:27 There is appropriate ADH release due to a hypovolemic state. 02:31 Incorrect. 02:32 This gentleman is euvolemic on exam and RAAS is suppressed based on his urine sodium. 02:38 So, letter B. 02:39 This is due to translocational hyponatremia. 02:41 His total body water stores are unchanged but there's a tonic effect from his SSRI that moves water from the intracellular to extracellular fluid compartment. 02:50 That's incorrect. 02:51 Translocational hyponatremia is hypertonic due to the presence of an effective osmole that exerts a tonic effect moving water from the intracellular to extracellular fluid compartment. 03:01 We're going to see that in cases of hyperglycemia or patients who received glycine as an irrigant, or potentially mannitol which is not osmotic diuretic. 03:11 What about letter C? There's an appropriate ADH release due to a low circulating arterial volume despite hypervolemia. 03:19 Also incorrect. 03:21 He is euvolemic on exam and if anything RAAS is suppressed based on his urine sodium. 03:27 So that leaves us with letter D. 03:29 There is inappropriate ADH secretion or SIADH. 03:32 And that answer is correct. 03:34 This is hypotonic euvolemic hyponatremia. 03:37 ADH is present again based on the fact that his urine Osm is greater than a serum Osm and RAAS is suppressed based on the fact that his urine sodium is high. 03:46 The cause in this situation is likely his SSRI. 03:53 So next question, how would we treat this patient? If his neurological status is stable, we can simply withdraw the offending drug so withdrawing the SSRI. 04:03 We want to free water restrict them anywhere between 0.8 to 1.2 liters. 04:08 And we want to ask him to increase his solute in his diet in order to increase water excretion through obligate osmolar excretion.
About the Lecture
The lecture Renal Case: 52-year-old Man with Depression by Amy Sussman, MD is from the course Water Balance: Hypo- and Hypernatremia.
Included Quiz Questions
Which of the following medications can cause SIADH?
- Selective serotonin reuptake inhibitors
- Carbonic anhydrase inhibitors
- Warfarin
- Biguanides
Which of the following is one of the three treatment components in the management of SIADH if the patient is neurologically stable?
- Increase salt intake
- Increase fluid intake
- Transsphenoidal hypophysectomy
- Desmopressin
Author of lecture Renal Case: 52-year-old Man with Depression

Amy Sussman, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
