Playlist
Show Playlist
Hide Playlist
Regulation of Fluid and Electrolyte Balance: Regulation Wheels

-
Slides RegulationofFluidandElectrolyteBalance IntegratedRenalPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
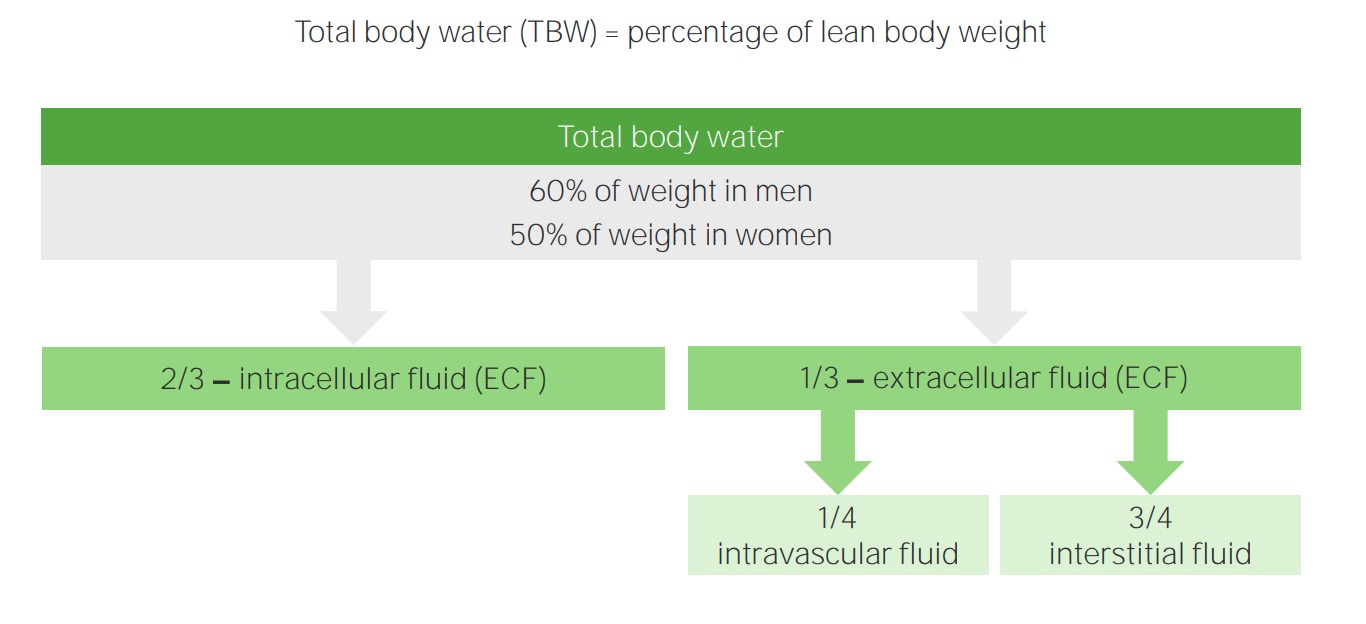
00:00 and these are the wheels that we shall see. Now, let me explain the wheels to you because these are beautifully done, well color coordinated and the way that it has an influence on each other. You should have these wheels permanently etched in your head, one in one eye, the other in the other eye. Now, towards normal, let us talk about tonicity, ADH, and excretion or retention. I do want you to pay attention to the colors. Okay. So let us begin on the area of osmolarity first. So we are going to take a look at the right circle first. 00:36 You find that the tonicity is increased. I want you to follow the red arrow, and what is in red only, at this juncture. How does that occur? Maybe they were sweating. What sweating mean to you? It is hypertonic loss of sodium, meaning you are losing more water than you are of your sodium. Thus, your plasma osmolarity increases. That we have talked about. Once the plasma osmolarity increases, immediately from the posterior pituitary, you are going to then release your ADH, of course, coming from the hypothalamus. Then what does this ADH do? I want you to go up to water, in red. You know that ADH is going to retain water. In other words, you are going to reabsorb water from the collecting duct technically. Doesn't it? In the hopes of doing what to tonicity? Bring it back to normal. 01:24 Are we okay? Let us take a look at the other example. What if your tonicity is decreased? Simple example such as drinking water. You drink water, excess. What happens to plasma osmolarity? You are drinking pure water. So all that you are doing is strictly increasing the total body water in the denominator. If that is happening, then you know that your plasma osmolarity is decreased. All I am doing here is integration of the topics that we talked about with the ratio. How do you determine plasma osmolarity? Serum sodium. 01:59 What does serum sodium mean to you clinically? It is the total body sodium over total body water. Our discussion with that, we talked about in great lengths. If that is not clear and you cannot recall that I would once again recommend. You go back and take a look at the lecture series. So your plasma osmolarity is decreased because of, well let us say excess water. Thus, what are you going to do with ADH? Suppress the release of it. Suppress the release, why? Well because you have too much water consumption. Don't you want to urinate this out? Of course, you do. So why don't we suppress our ADH? So now by suppressing ADH, in blue, what are you going to do with that water? Excrete it. You tell me what kind of urine you are producing? What kind of urine? Dilute or concentrated urine? Good. Diluted urine. So that you can bring the tonicity back up to normal. You see how important it is. 02:54 That is happening in us right now. Let us go over to the left. On the left, here we will be dealing with you begin with effective circulating volume. Let us go with the one in the red again. Say that you are losing effective circulating volume, what does that mean? Plasma. So what are you going to release? I want you to go down to the kidney. If you have decreased perfusion to the kidney, you're releasing renin and company. I want you to focus upon aldosterone. What is that aldosterone going to do in the collecting duct? Please go to red. The red saying sodium reabsorption. When you have sodium reabsorption, what are you doing to volume? You are then going to increase the volume back towards the normal. Are we clear? What if you increase your effecitve circulating volume because maybe perhaps you infused too much normal saline? You will infuse too much normal saline, increased effective circulating volume, what then happens to your perfusion to the kidney? Increased. What are you going to do with renin? You are going to suppress the release of renin. So, therefore, what are you going to do with sodium? You are going to excrete the sodium so that you can bring your volume back to normal. Interesting. Sodium, volume left circle regulated by aldosterone. 04:13 On the right, water tonicity, regulated by ADH. Do you see anycross over here? No. In the previous statement, in the previous discussion, I brought the term or introduced the term crossover to you, we're not seeing it here yet. Here we go. So the crossover has taken place. So what does this even mean? At all times, it is imperative and of at most priority that you maintain plasma osmolarity within normal range. There is always an exception. Here it is. Say that you get into an accident unfortunately and you are losing tonnes of blood, massive hemorrhage. 05:01 You are losing so much hemorrhage that it is 10 percent of or greater than 10 percent effective circulating volume, which is depleted. The volume has been lost so much. It is now the body's responsibility to now increase the blood pressure as quickly as possible as dramatically and desperate as possible. It is desperate right. 05:25 So, therefore, aldosterone is being kicked in, and that out the sodium, you try to retain the fluid maybe perhaps that is not enough. You bring your angiotensin II from your left circle with enough volume loss. You are going to stimulate ADH in the hopes of doing what? To then retain and reabsorb that water so that you can bring blood pressure back to normal. 05:51 My recommendation for you to learn this is first you take a look at the circles seperately. 05:57 You go in the priority order that I had given you with organisation, which is tonicity first, then volume. Number 2, right circle, left circle. Once you’ve firmly implanted those circles in your head, then you move over to crossover, understand when that takes place that will be massive hemorrhage when you are losing greater than 10 percent of your effective circulating volume. What then takes priorty? The volume takes priority over osmolarity at this juncture.
About the Lecture
The lecture Regulation of Fluid and Electrolyte Balance: Regulation Wheels by Carlo Raj, MD is from the course Fluid and Electrolyte Balance.
Included Quiz Questions
Which of the following hormones directly stimulates water reabsorption through aquaporins in the renal tubules?
- Antidiuretic hormone
- Renin
- Aldosterone
- Angiotensin II
- Angiotensin I
Which of the following descriptions is most ACCURATE?
- Antidiuretic hormone increases urine osmolarity.
- Aldosterone Decreases plasma osmolarity.
- None are correct
- Antidiuretic hormone increases plasma osmolarity.
- Aldosterone decreases effective circulating volume.
With profound perspiration and resultant serum hypertonicity, which of the following hormonal changes is most likely?
- Increased antidiuretic hormone secretion
- Decreased antidiuretic hormone secretion
- Increased urinary excretion
- Urinary dilution
- Syndrome of inappropriate antidiuretic hormone secretion
Which of the following hormonal changes is most likely in a patient with decreased plasma osmolarity?
- Suppresion of antidiuretic hormone
- Suppresion of renin
- Suppression of sodium reabsorption
- Suppression of angiotensin II
- Suppression of aldosterone
Which of the following hormones plays the most significant role in restoration of effective circulatory volume during blood loss?
- Aldosterone
- Antidiuretic syndrome
- Cortisole
- Prolactin
- Norepinephrine
Which of the following is most likely to increase when the production of aldosterone increases?
- Blood pressure
- Urinary output
- Sodium excretion
- Renin release
- Heart rate
Author of lecture Regulation of Fluid and Electrolyte Balance: Regulation Wheels

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
One of the most confusing concept is explained very clearly in a short video!!
