Playlist
Show Playlist
Hide Playlist
Osteopathic Considerations of the Upper Extremity


-
Slides Osteopathic Considerations of the Upper Extremity.pdf
-
Reference List Osteopathic Manipulative Medicine.pdf
-
Download Lecture Overview
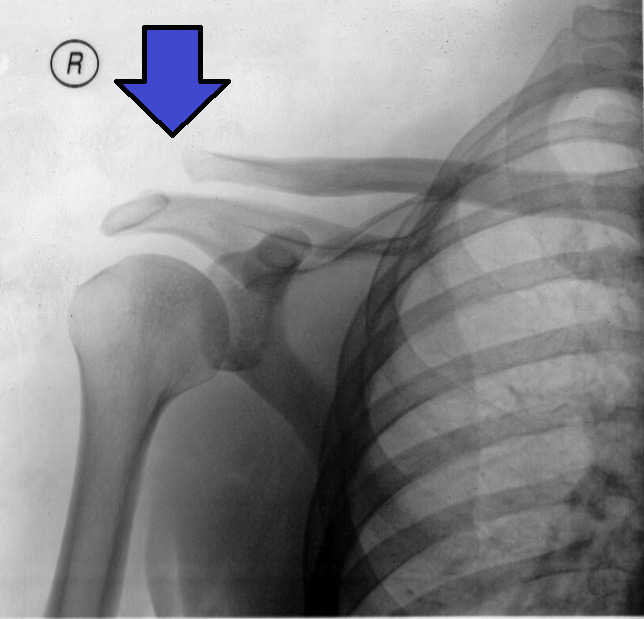
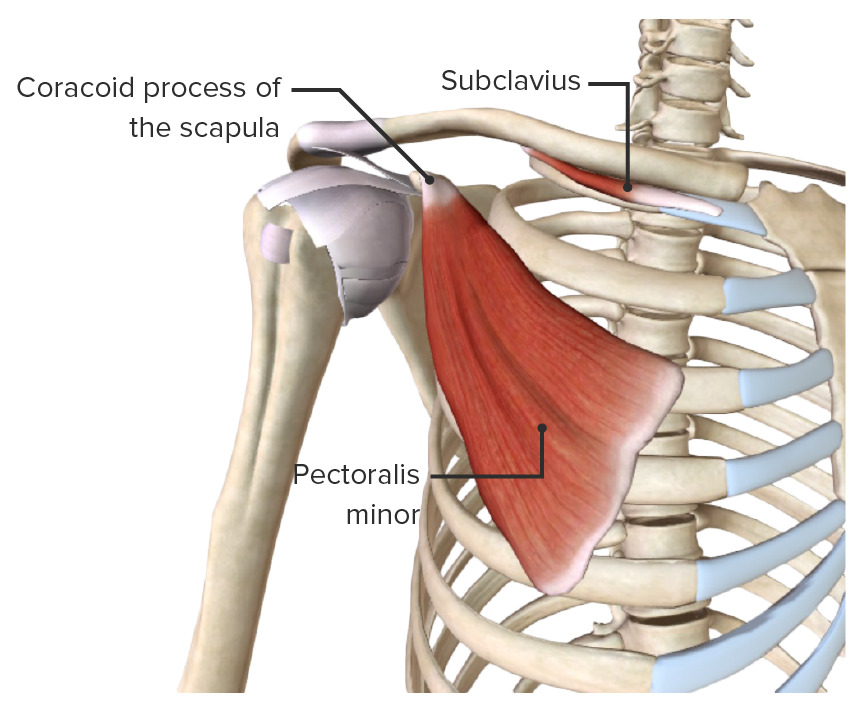
00:01 We're going to talk about the upper extremity and the osteopathic considerations when thinking about the arms. 00:06 We're going to talk about the shoulder first, the elbow, the wrist, and the hands. 00:11 We're going to cover anatomy, pathologies, diagnosis, and management. 00:15 I want to start with the shoulder because it's a complicated joint. 00:19 There are a lot of problems that happen with the shoulder girdle. 00:22 It's actually four joints. But let's talk about the scapula (the wing bone), the humerus (the arm), the clavicle, and the sternoclavicular joint that all come together to form the shoulder girdle. 00:36 That joint has a lot of problems, a lot of pain, and is a complicated one to assess. 00:43 So besides the four joints, the bones, there are also four muscles. 00:48 We call them them the rotator cuff muscles. 00:51 It's the supraspinatus, infraspinatus, teres minor, and subscapularis. 00:56 Those are the four muscles that make up the rotator cuff and move the shoulder in all the directions. 01:03 The supraspinatus will cause abduction, moving it away from the body. 01:08 The infraspinatus will cause external rotation. 01:12 The teres minor also helps in external rotation. 01:16 The subscapularis does internal rotation. 01:20 So those are the four main muscles. 01:24 But you also have a contribution for shoulder motion from the biceps because the long head of the biceps is going to go into the subglenoid region. 01:34 The short head is going to go into the coracoid process and move the shoulder. 01:40 So, if you go back and look at the shoulder one more time and think of it as a strut, it's important to realize that the coracoid process that comes out under the clavicle is part of the scapula. 01:55 The scapula is connected to both the arm and to the acromion bone. 02:04 So it's going to have multiple connections which makes it complicated and difficult to manage because one problem is going to cause other problems. 02:14 Having the four muscles and the four tendons there can cause problems with motion. 02:22 The long head of the biceps is going to have its origin in the subglenoid tubercle. 02:28 The short head of the biceps is going to have its origin in the coracoid process and insert in the radial tuberosity in the bicipital aponeurosis. 02:39 So these are the basic areas to think about. 02:43 The boundaries of the shoulder are the clavicle, the first rib which is deep to the clavicle, the subclavian muscle, and the anterior and posterior scalene muscles that you can see, the subclavian vein which is deep and able to be cannulated, the subclavian artery even deeper, and the brachial plexus of nerves which is coming underneath the muscles. 03:09 Shoulder pathologies: We are going to see shoulder dislocation particularly with trauma. We’ll see shoulder separation. 03:18 We'll see adhesive capsulitis. Those are the three main shoulder pathologies you'll see in a general practice. 03:25 A shoulder joint location is typically anterior and inferior. 03:30 It's from a smack, or a hit, or a fall, kind of when playing contact sports. 03:35 It's when the humeral head, the top of the arm, gets pulled out of the glenoid fossa and inhibits motion because it's no longer pulled accurately, pulled efficiently by the muscles involved. 03:49 If you want to test for it, it's a tough test because somebody who dislocates their shoulder is in a lot of pain. 03:57 They're protecting their arm. They don't want to move it. 04:00 What you want to do is to have them go to 90 degrees and lift up. 04:04 But if you try and separate it and it's got an anterior and inferior dislocation, they're not going to let you. 04:10 If you do get there and you see the grimace, you understand there's a dislocation. 04:14 If you can't get it externally rotated, there's a good chance it's dislocated. 04:20 If you can't get it to 90 degrees, there's a good chance it's dislocated. 04:24 Some of the issues to worry about are joint instability and assessing for the arm being out of the shoulder joint and unable to function. 04:36 So if a person cannot externally rotate because the supraspinatus is unable to abduct, that's a good sign. 04:45 If they can't move their arm and they're protecting their arm, that's a sign you may have a shoulder joint dislocation. 04:51 The management of a shoulder dislocation is a reduction, put it back into joint. 04:57 The problem is when you dislocate the shoulder, you're going to have some hypertonicity. You're going to have some contraction. 05:04 As the hours go on, the contraction of the muscle is going to get tighter. 05:08 Pulling the arm to where it can go back in the joint is going to get more difficult. 05:14 From an osteopathic perspective, you can deal with the hypertonicity. 05:18 You can treat the hypertonicity as a prelude to putting the arm back into place. 05:23 So while muscle strengthening is a long-term treatment, flexion and extension muscle energy techniques and fatiguing the muscle will help with the hypertonicity and help you put a dislocated shoulder back into joint. 05:37 Shoulder separation is also trauma-related when the AC joint is pulled. 05:45 It could be simple or complex. It could be one ligament or two. 05:50 Because ligaments connect bone to bone, they will connect the sternoclavicular joint and the AC joint, acromioclavicular joint. 06:00 The management of an AC separation is going to be medical: rest, ice, analgesia, immobilization, and if it is severe, surgery. 06:11 But most of the time we're letting it heal on its own, giving it time to see what's going to happen. 06:16 In the osteopathic treatment realm, you have indirect techniques and passive techniques to deal with the discomfort and to help the body heal itself as much as possible. 06:27 Adhesive capsulitis is a loss of motion, a restriction in the shoulder usually secondary to inflammation. 06:36 Autoimmune disease, diabetes, hypothyroidism can all cause an adhesive capsulitis more common later on in age. 06:44 An adhesive capsulitis is a loss of motion from an autoimmune disease or other etiology. 06:50 The test is called the Apley's Scratch test to see if you have a loss of motion in the shoulder joint. 06:56 The Apley’s Scratch test is when you touch your scapula, touch your scapula, and touch your scapula and see how far a person can go to touch their scapula. 07:06 If you get to about the same area, you're in good shape. 07:09 If you can't get close, you're starting to have some trouble. 07:12 We'll do a separate short video on the Apley’s Scratch test just so you're aware of how to do it and when to do it. 07:20 Management of adhesive capsulitis is local with heat, ice, analgesics. 07:26 Occasionally, you can get a corticosteroid injection or anti-inflammatory. 07:30 Surgery is an option as well. 07:33 From the osteopathic medical world, we will do some muscle energy. 07:37 We will work on the external rotation in order to help enhance motion. 07:41 There's something called the 7 Steps of Spencer. 07:45 The Spencer techniques will help enhance motion, maintain motion, and is a treatment for adhesive capsulitis. 07:51 Other shoulder issues we worry about are rotator cuff tears, impingement syndromes, and biceps tendonitis, biceps rupture, and biceps issues. 08:02 Starting with the rotator cuff tear, a rotator cuff tear is a tear of one of the four muscles of the rotator cuff: the supraspinatus, infraspinatus, teres minor, or subscapularis. 08:13 You will know if you tear a portion of the rotator cuff by having a loss of use or a loss of motion. 08:20 The test for the rotator cuff muscles are simple tests. 08:24 It's drop arm. Can you lift your arms all the way up and do they fall? Can you lift them above 90 degrees? The empty can test is basically holding a can and spilling it over. 08:34 If you can do that, your rotator cuff is intact, all three things. 08:37 Generally, you will know when you have a rotator cuff tear. 08:42 It is painful. People will hear a snap or a pop. 08:45 Again, they've lost the ability to do something they were doing before. 08:49 They may not always try and empty a can but they know if they can't beforehand. 08:54 Management of rotator cuff tears is very difficult. 08:58 We treat it locally at first symptomatically with rest, ice, analgesics, and surgery. 09:03 We do offer myofascial release and facilitated positional release to help enhance motion. But if you have a loss of anatomic motion, you're also going to have a loss of physiologic motion. 09:19 So, you're going to get some benefit but not total benefit. 09:23 Impingement syndrome, this is an inflammation of the tendons of the rotator cuff. 09:28 Usually, the supraspinatus is the most common impingement syndrome but it can occur with any of the rotator cuff muscles. 09:37 We'll talk about the tests later. 09:40 The Neer’s sign and the Hawkins-Kennedy test are different ways of looking for impingement syndromes. 09:49 Again, there'll be short videos on Neer’s sign and Hawkins-Kennedy test. 09:53 Management of an impingement syndrome is medical at first with rest, ice, analgesia, a corticosteroid injection or analgesics. 10:01 We will do strain counterstrain for impingement syndromes. 10:04 We'll do myofascial release as well and muscle energy. 10:09 The counterstrain point is around the area of shoulder flexion with supination of the forearm. 10:16 So, you're going to find the counterstrain point and then find the position of ease. 10:21 Muscle energy can also be done to help with impingement syndrome. 10:24 Biceps tendonitis: When you have inflammation, or degenerative changes, calcification surrounding the long head of the biceps. 10:33 We'll talk about the different tests for bicep tendonitis. 10:37 There's the Yergason's test and Speed’s test, both of which we'll have short videos showing you how to do these tests as well. 10:44 Treatment of impingement syndrome is local at first with rest, ice, analgesia, and question of steroids. 10:51 We will do counterstrain and myofascial release. 10:55 This is to both the long head of the biceps and the short head of the biceps. 11:00 When the shoulder neurovasculature is interrupted or hurt, it may be a medical emergency and it needs to be taken care of right away. 11:11 When someone has severe pain, or numbness and tingling in the vascular or neurovascular area, it could be due to a compression of the neurovascular structures of the shoulders. 11:22 This needs to be paid attention to. 11:25 The test for neurovascular compromise is called Adson's test. 11:31 You can evaluate this and we'll go through that test in a separate video as well. 11:36 But if you have a loss of pulse when you're doing the test, that's something to worry about. 11:41 When you talk about osteopathic management of thoracic outlet, we will treat the first rib. 11:47 We will treat the sternocleidomastoid muscles as well as the thoracic outlet. 11:54 You can use muscle energy or balanced ligamentous tension to treat these areas.
About the Lecture
The lecture Osteopathic Considerations of the Upper Extremity by Tyler Cymet, DO, FACOFP is from the course Osteopathic Treatment and Clinical Application by Region. It contains the following chapters:
- Osteopathic Considerations of the Upper Extremity
- Shoulder
- Shoulder Girdle – Shoulder Joint Dislocation
- Shoulder Girdle – Shoulder Separation
- Shoulder Girdle – Adhesive Capsulitis
- Shoulder Musculature – Rotator Cuff Tears
- Shoulder Musculature – Impingement Syndrome
- Shoulder Musculature – Biceps Tendonitis
Included Quiz Questions
Which of the following muscles are considered part of the rotator cuff of the shoulder? (Select all that apply.)
- Supraspinatus
- Infraspinatus
- Teres minor
- Subscapularis
- Teres major
Which of the following special tests is part of the evaluation for shoulder instability?
- Apprehension test
- Empty can test
- Yergason's test
- Spurling's test
- Adson's test
Which of the following is the most common direction of a glenohumeral shoulder dislocation?
- Anterior-inferior
- Posterior
- Posterior-inferior
- Superior
Which of the following special tests is part of the evaluation for thoracic outlet syndrome?
- Adson's test
- Empty can test
- Yergason's test
- Apley scratch test
Author of lecture Osteopathic Considerations of the Upper Extremity

Tyler Cymet, DO, FACOFP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
