Playlist
Show Playlist
Hide Playlist
Anti-HIV Agents: Nucleoside and Nucleotide Reverse Transcriptase Inhibitors (NRTIs) – Antiviral Drugs


-
Slides Anti-HIV Agents NsRTIs Antiviral Drugs.pdf
-
Reference List Pharmacology.pdf
-
Download Lecture Overview
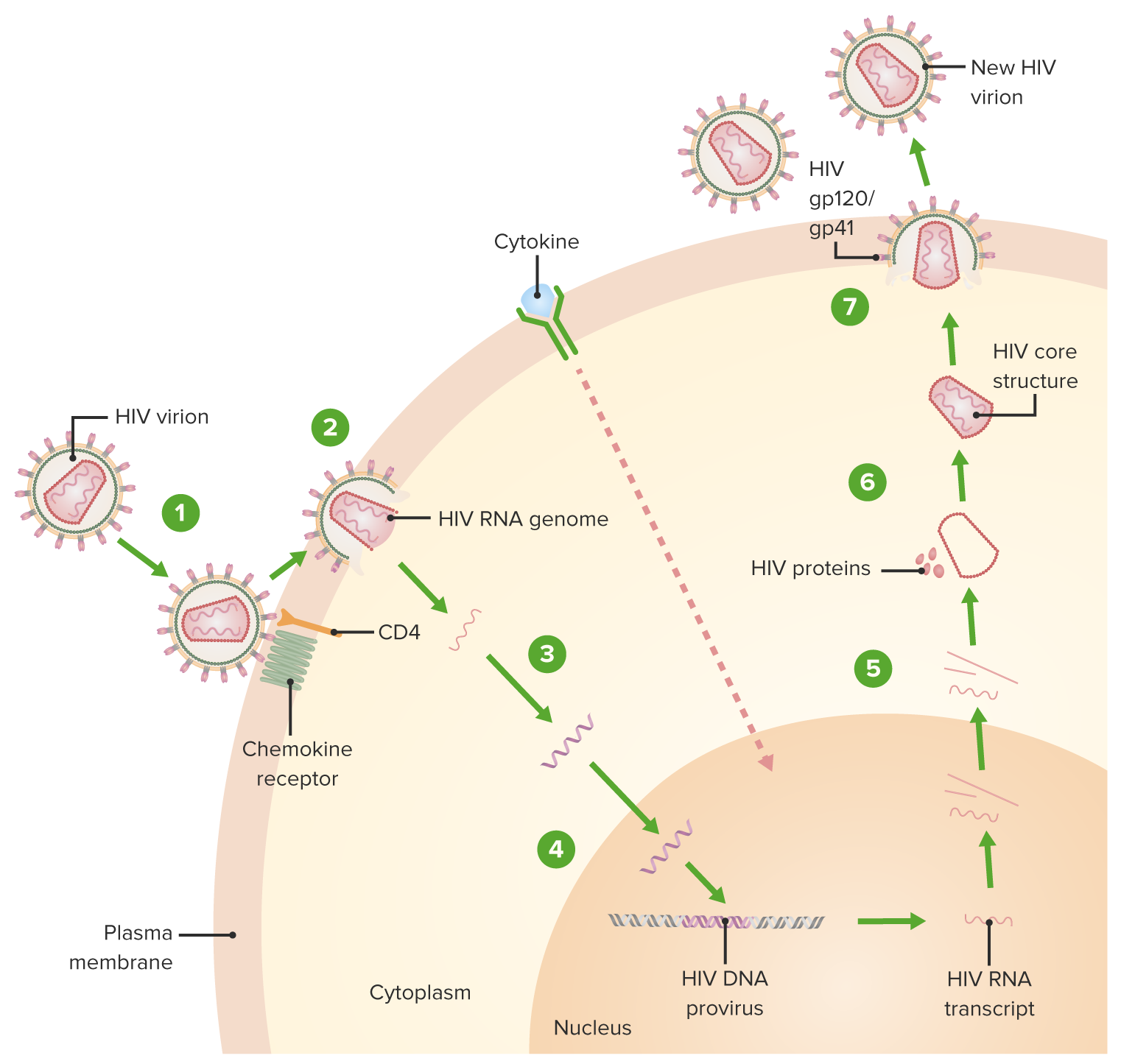
00:01 Today we're focusing on the foundation of HIV treatment. 00:05 The NRT, or nucleoside reverse transcriptase inhibitors. 00:11 Let me first emphasize two critical points about HIV therapy one we start treatment immediately after diagnosis, regardless of Cd4+ count. 00:21 Two modern HIV treatment follows a standard approach two nrtis plus an integrase inhibitor the Nrtis were discussing today are what we call the backbone of therapy. 00:34 They're always used in pairs, either tenofovir with emtricitabine or abacavir with lamivudine. 00:42 This dual NRT combination is just that essential. 00:45 It's the foundation that all other HIV medications build upon. 00:50 While there are several other drug classes, including integrase inhibitors. 00:56 And protease inhibitors, these NRT pairs remain constant in our treatment regimens. Currently, our preferred approach is to combine this nrti backbone with an integrase inhibitor like Dolutegravir or bictegravir, chosen for its excellent efficacy and safety profile. 01:15 Think of HIV treatment like building a house. 01:18 The NRTI backbone is your foundation and everything else builds upon that base. Let me explain. Nucleoside tide reverse transcriptase inhibitors, or NRTIs. These are fundamental to HIV treatment, and here's why. 01:33 We call them the backbone. 01:35 They're always used in pairs as the foundation of HIV therapy. 01:40 The most common pairs you'll see are tenofovir plus emtricitabine or abacavir plus lamivudine. 01:47 Think of these as inseparable partners in HIV treatment. 01:51 Their mechanism is straightforward. 01:53 They're phosphorylated inside the cell where they block reverse transcriptase and stop viral DNA chain elongation. 02:01 Here's something important. 02:02 Three of these drugs pulled double duty. 02:05 Lamivudine, emtricitabine, and tenofovir. 02:08 Don't just treat HIV. They also treat hepatitis B virus. 02:13 Finally, you must know the side effects, particularly mitochondrial toxicity. This can show up in several ways. 02:21 Lactic acidosis, for which there is a black box warning, peripheral neuropathy and pancreatitis. 02:28 And there's one specific warning for tenofovir. 02:31 Watch for Fanconi syndrome a problem with kidney tubule function. 02:36 Remember these drugs are always the foundation of HIV treatment. 02:40 That's why we call them the backbone. 02:43 Today, let's examine how two key drug classes work to stop HIV one replication. Looking at this elegant diagram, we can follow both the viral process and our therapeutic intervention points. 02:57 When HIV one enters a cell, it undergoes uncoating to reveal what we call the ball shaped nucleocapsid. 03:05 This is where our drug therapy comes into play, and it's fascinating how two distinct approaches were discovered to interfere with viral replication. The backbone of our therapy relies on NRT eyes. These are nucleoside analogs. 03:21 Notice I say start because some are nucleosides like emtricitabine, while others are nucleotides like tenofovir. 03:30 These drugs are cleverly designed imposters. 03:33 See in the diagram how they require cellular kinases for phosphorylation. 03:38 Once activated, they compete with natural Des and terminate the viral DNA chain, essentially creating a dead end in viral replication. The second approach, using NNR, is one option for our third agent or anchor drug, rather than mimicking building blocks. 03:59 These drugs find a hydrophobic pocket on the reverse transcriptase enzyme. 04:03 Think of it as throwing a wrench in the machinery. 04:06 It changes the enzyme's shape through allosteric inhibition. 04:10 Both approaches prevent viral RNA from becoming DNA. 04:13 But remember, in modern therapy, nrtis form our essential backbone. While nrtis are just one option for our anchor drug alongside integrase inhibitors and protease inhibitors. 04:27 Let's discuss the backbone of HIV therapy, our NRT. 04:32 This is high yield material for your boards, so listen carefully. 04:37 First, understand that these drugs are nucleoside or nucleotide analogs. Looking at our structures here tenofovir is unique. It's the only nucleotide analog meaning it already has a phosphate group. The others emtricitabine, lamivudine and abacavir are nucleoside analogs. 04:58 Now the side effects one for tenofovir. 05:02 Remember, renal issues, especially Fanconi syndrome two emtricitabine and lamivudine are generally safe. 05:10 But remember skin hyperpigmentation for emtricitabine, four for lamivudine know it can cause HBV flare if stopped. When used to treat hepatitis B infection with abacavir, you must know two things hlab5701 testing is required. Fatal hypersensitivity can occur if this is positive three finally, remember the class effects. 05:35 All can cause lactic acidosis and hepatic steatosis. 05:40 This is due to mitochondrial toxicity. 05:42 These drugs are always used in pairs, either tenofovir emtricitabine or abacavir lamivudine. 05:50 Remember, this is just the backbone. 05:52 You'll add a third drug from a different class. 05:55 The next one is commonly known as DDE. 05:59 It's it's used quite extensively. 06:01 Um, remember, with DDE you have to reduce the dose based on the kidney function of the patient. 06:08 Resistance. Again, unlikely because it requires several point mutations on the part of the DNA. 06:15 Sorry, the RNA of the, uh, of the virus. 06:19 Adverse events. There's a high degree of pancreatitis, up to 30%. So this point's going to be, uh, crucial on your exam. Pancreatitis DDE. 06:29 Watch carefully for signs of pancreatitis in your patients. 06:34 You can also get a peripheral neuropathy with this particular drug. 06:39 Other drugs include stavudine. 06:41 Now this is a renally eliminated medication as well. 06:45 You have to adjust your dose based on the renal function. 06:48 And side effects can include peripheral neuropathy. 06:51 Uh, of course this drug is well known to possibly increase the risk of lactic acidosis. You can also get some steatohepatitis. 07:01 And this is a more common reaction, the steatohepatitis, than it is in the other nrti's. 07:08 Zidovudine used to come under another name that's utterly unpronounceable. 07:12 It's distributed to most tissues. 07:14 It's limited via via both the kidney and via the liver. 07:19 Toxicities of this medication include bone marrow suppression. 07:23 And this is a particular concern in patients with HIV. 07:26 Anemia is also seen in patients on this drug and of course neutropenia. 07:31 In terms of your side effects usually gastric distress is something that we are concerned about. Um, one thing I want to mention is a disease called Fanconi syndrome. 07:41 If you can burn this into your memory, the Fanconi syndrome and this particular drug, you will get at least one question. 07:49 Right. Um, on your exams. 07:52 Neuro includes headache, insomnia, and fatigue.
About the Lecture
The lecture Anti-HIV Agents: Nucleoside and Nucleotide Reverse Transcriptase Inhibitors (NRTIs) – Antiviral Drugs by Pravin Shukle, MD is from the course Antimicrobial Pharmacology.
Included Quiz Questions
Which findings are most consistent with the side effect profile of nucleoside reverse transcriptase inhibitors?
- Lactic acidosis and hepatic steatosis
- Respiratory acidosis and acute kidney injury
- Metabolic acidosis and cholestasis
- Respiratory acidosis and heart failure
- Lactic acidosis and obstructive uropathy
What best describes highly active retroviral therapy (HAART)?
- Co-administration of different drugs that inhibit viral replication by several mechanisms
- Single antiretroviral drug therapy to reduce the chances of drug resistance
- Sequential introduction of multiple drugs to increase the likelihood of treatment success
- Use of antiretroviral medications that are also active against tuberculosis
- Use of at least 2 drugs from the same group of antiretroviral medications
Which nucleoside reverse transcriptase inhibitor is most likely associated with a severe hypersensitivity reaction?
- Abacavir
- Didanosine
- Emtricitabine
- Lamivudine
- Zidovudine
What is the primary mechanism by which NRTIs inhibit HIV replication?
- Competitive binding to reverse transcriptase, leading to chain termination
- Inhibiting protease enzyme activity
- Preventing viral RNA from binding to the host cell
- Inhibiting the integration of viral DNA into the host genome
- Blocking the assembly of viral proteins
Author of lecture Anti-HIV Agents: Nucleoside and Nucleotide Reverse Transcriptase Inhibitors (NRTIs) – Antiviral Drugs

Pravin Shukle, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
good lecture explaining everything about: Anti-HIV Agents: Nucleoside Reverse Transcriptase Inhibitors (NsRTIs) – Antiviral Drugs
