Playlist
Show Playlist
Hide Playlist
Normal Hemostasis Pharmacologic Anticoagulants

-
Slides NormalHemostasis.pdf
-
Download Lecture Overview
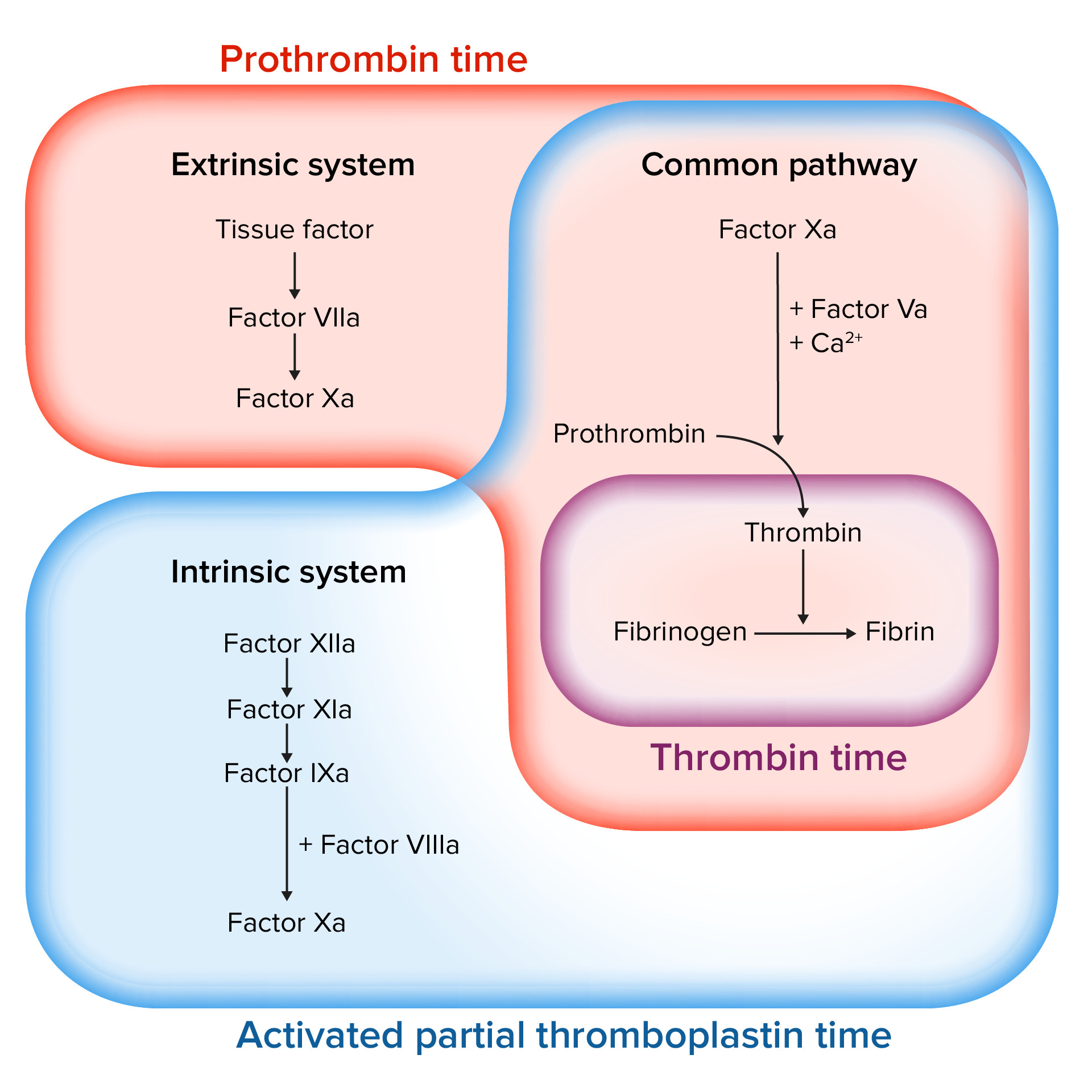
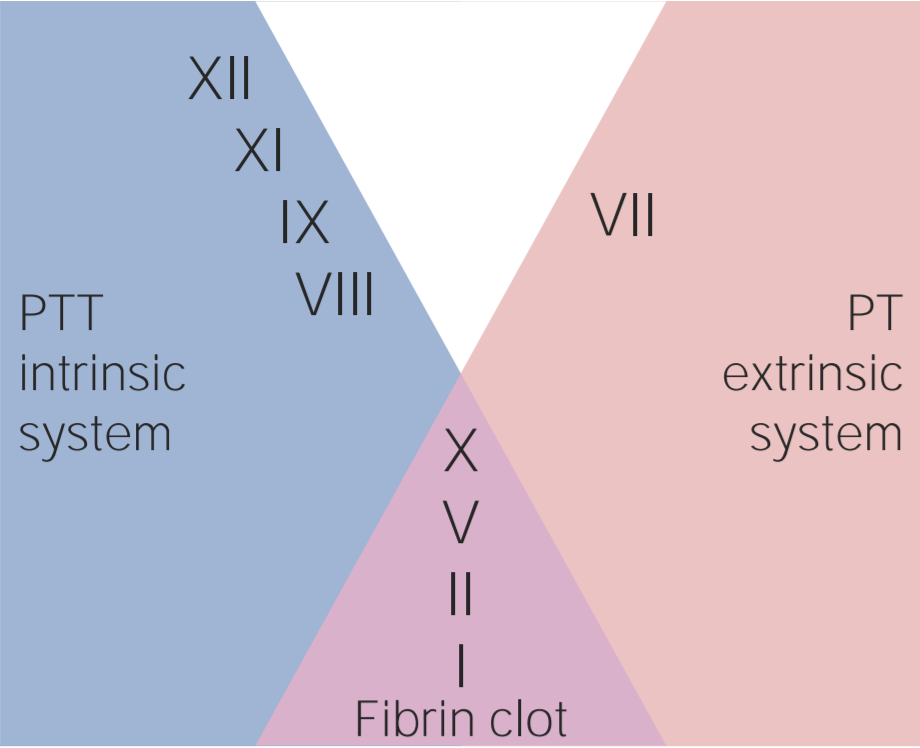
00:00 Let's take a look at some pharmacologic anticoagulants for us. 00:05 First, we'll take a look at heparin. 00:08 Remember, heparin will never be given for you, clinically, will never be given outside of the hospital. 00:14 Heparin will only be given parenterally, not orally. 00:18 Heparin can be given either in the form of IV or it could be given in the form of subcutaneous. 00:24 Heparin, can it be given during pregnancy? Yes, it can. It is not teratogenic. 00:32 Warfarin, however, cannot be given during pregnancy. It must be removed. 00:35 Warfarin will wage war upon the child, the fetus. 00:39 You can't do that. Heparin can be given, if need be. How quickly does heparin work? Like that. Like that, because heparin works upon antithrombin III. 00:53 What factor is thrombin? T, as in thrombin, T, as in two. 00:59 It's a heparin, like this, activates antithrombin III, in which it knocks up your thrombin. 01:07 So, if you don't have the thrombin, guess what you cannot do? You can't form or reform a plug. It works within seconds, heparin does. 01:16 And there is a small population in which, look for this, at the site of injection of your heparin, a patient may then form a clot. Excuse me? Yes. There's a subset of population who will develop autoantibodies that will activate platelet factor IV on your platelet and instead of inhibiting platelet activation, it actually activates a platelet forming a thrombi at the site of injection. 01:49 Now, here's a scenario that you'll be given. 01:53 If this condition we call heparin-induced thrombocytopenia, HIT, heparin-induced, what did it do? In that subset of population, it formed a thrombi. 02:06 Where? At the site of injection, number one, and number two, it activate a platelet so much that you form so many thrombi, that the platelet count would decrease. 02:16 Heparin-induced thrombocytopenia. 02:19 If that's the case, I want you to give me a drug or a classification of drugs that will be an alternate for giving heparin. 02:29 It's called dabigatran or maybe argatroban. 02:35 Dabigatran is the only oral direct-acting thrombin inhibitor, or dabigatran. 02:40 We'll talk a little bit more as we proceed. 02:43 What about warfarin? Warfarin, completely different. Warfarin can be given orally. 02:49 Another name for warfarin is Coumadin. 02:52 Now, warfarin could be given -- now, when would you even think about giving these drugs, by the way? Will the thrombi be located more so on the arterial side or would it be located more on the venous side? That's an interesting topic, isn't it? Who's the patient that I gave you earlier, who said, "Doc, I have pain?" Where? My calf region, lower legs. Especially, when I dorsiflex. 03:15 I gave you a female and I told you maybe she was obese or maybe she was pregnant and maybe she was on a long plane trip. 03:23 I gave you all of those risk factors because she's developing what kind of thrombi, please? A venous thrombi. What is it in that female that is prothrombotic, that hormone? Estrogen. Now, wait, step back for a second. Estrogen is quite interesting. 03:38 Cuz you should know that estrogen on the arterial side for thrombi formation protects the lady, right? That's why a lady who develops coronary artery disease will be much later than it would be for a male, in which we don't have estrogen. 03:56 But that protects you on the arterial side, fascinating. 03:59 And it's mostly because on the arterial side, the thrombi that you're forming, you call it -- you've heard of atheroma and such, of course. 04:06 We've had that discussion. 04:07 Whereas in the venous side, it's going to be purely a coagulation issue. 04:11 So therefore, heparin, antithrombin, and warfarin, works via? Warfarin works through vitamin K-dependent factors. 04:20 Here we go, what are they? II, VII, IX, and X. Clotting or non-clotting? Clotting factors, prothrombi. And what are the other two? Protein C and protein S. 04:31 Those are anticoagulants, naturally acting. Next, remind me about the short half-life? Which one has a short half life? Protein C and S. 04:41 Remind me these vitamin-K dependent factors. 04:44 What's the name of that carboxylation? Gamma carboxylation. 04:47 Therefore, you don't activate or you don't synthesize new II, VII, IX, and X from the liver, correct? But what made them disappear in your patient? Protein C and S. Why? Because its half life is so incredibly short in such patients where it might still be circulating. 05:06 II, IV, IX, and X. Forming what, maybe? Microthrombi up and down the body, resulting in widespread skin necrosis. 05:16 If you don't get that point, make sure you repeat that cuz it's key that you understand the difference between the necrosis that will take place with HIT, with heparin, the site of injection, versus the skin necrosis that may take place with warfarin. 05:32 So therefore, it's extremely important, remember, heparin, what clinical test are you gonna use to measure the activity of heparin? Clinically, it's PTT. Warfarin, if you want, the mnemonic is cute. 05:47 I'm not usually a mnemonic man, but at times, I think they're fun. 05:50 WEPT. W-E-P-T. W, warfarin, E, extrinsic system, primarily, granted every single resident and student asks me this question. 06:05 Dr. Raj, factor II, it's thrombin, that's part of both intrinsic and extrinsic, I get it. 06:11 Factor VII, okay, I get it, that's part of extrinsic, but then, IX and X, X is part of both and IX is part of intrinsic. 06:22 What am I trying to get at? Interesting enough, II, VII, IX, and X, they're components of both intrinsic and extrinsic, aren't they? But clinically, what test are you gonna measure only? PT/INR, period. WEPT, if it's not warfarin, it's heparin. If it's not extrinsic, it's intrinsic. 06:42 If it's not PT, then it's PTT. It's just the opposite. 06:45 There you have it, two of the major drugs. 06:47 Now, warfarin is teratogenic, you can't use it, not in pregnancy. 06:52 Now, warfarin, we'll talk about this in a bit, I have to give you a new drugs. 06:56 Warfarin has been proven over and over for about 50 years now, to be extremely effective in preventing prophylactically, an emboli, from the left side of the heart, that's a secondary to Afib, going up in the carotid, resulting in a cerebrovascular accident, aka, stroke. 07:18 Effectively. However, there are new drugs that you must know that could be a substitute for warfarin for such embolization from the left atrium. 07:29 These drugs include direct-acting thrombin inhibitors. Imagine this a few times, dabigatran, the oral agent, or maybe a factor X inhibitor, called apixaban, rivaroxaban, it has a letter X in it. Interesting. 07:46 Let's talk about that PT. I gave you the mnemonic WEPT. 07:52 W, warfarin, E, extrinsic, oh, PT. We can go through this quickly now. 07:57 Take a look at the picture here. 07:59 Over to the far right, the extrinsic system begins with which coagulation factor? Factor VII, there you go, and there is PT. 08:07 A drug care primarily would be your warfarin. Take a look at this. 08:11 Step back for a second and take a look at the picture. 08:14 You formed an X, it's about the extrinsic and intrinsic will converge upon factor X. 08:20 PT, your gamma carboxylase vitamin K-dependent factors from the liver. 08:28 So, if a patient has liver disease, whatever type hepatitis, NASH, autoimmune, alcoholic, viral, whatever it may be, you would expect there to be an elevated PT. 08:42 Warfarin, obviously, an increase in PT. Then over to your left, there's intrinsic. 08:50 How do I know? The intrinsic, you have memorized at this point, begins with which factor? Factor XII. It'll be measured by PTT. What's the time here for PTT? 25-40 seconds. 09:04 Please remind me what the drug here that primary works or you will be measuring with PTT? If it's not warfarin, then it will be heparin. 09:14 Couple of other things here, exclusively. See, where it says, hemophilia. 09:18 Remind me, A before B, so therefore, VIII before IX. 09:24 In other words, if the patient is factor VIII deficient, then you find an elevated PTT only and that patient has hemophilia A. 09:34 How do you know? It might be a child and such, you might have severe gingival bleeding. 09:38 Might add bleeding into the joints called hemarthrosis. 09:40 Is that understood? Where is if the patient's deficient of factor IX, then that would be hemophilia B. 09:48 We're all doctors here. So, we don't get 12 days of Christmas, we're gonna get 9 days of Christmas. What am I getting at? Another name for factor IX deficiency is Christmas disease, hemophilias.
About the Lecture
The lecture Normal Hemostasis Pharmacologic Anticoagulants by Carlo Raj, MD is from the course Hemostasis: Basic Principles with Carlo Raj.
Included Quiz Questions
Heparin affects which of the following components of the clotting cascade?
- Antithrombin 3
- Plasminogen
- Von Willebrand factor
- Vitamin K
- Protein C
Which of the following medications may be used as an alternative to heparin in patients with heparin-induced thrombocytopenia (HIT)?
- Argatroban
- Enoxaparin
- Aspirin
- Unfractionated heparin
- There are currently no alternatives to heparin in patients with HIT.
Which of the following tests is commonly used for monitoring warfarin therapy?
- International normalized ratio
- Bleeding time
- Activated partial thromboplastin time
- Clotting time
- Complete blood count
Which of the following coagulation factors is NOT affected by warfarin?
- Antithrombin 3
- Factor II
- Factor VII
- Factor IX
- Factor X
An acquired deficiency of which of the following agents is the cause of warfarin-induced skin necrosis?
- Protein C
- Antithrombin 3
- Factor VIII
- Fibrinogen
- Plasminogen
Author of lecture Normal Hemostasis Pharmacologic Anticoagulants

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Thank you Dr. Raj! Super helpful and follows First Aid like a charm!
