Playlist
Show Playlist
Hide Playlist
Anti-HIV Agents: Non-nucleoside Reverse Transcriptase Inhibitors (NNRTIs) – Antiviral Drugs


-
Slides Anti-HIV Agents NNRTIs Antiviral Drugs.pdf
-
Reference List Pharmacology.pdf
-
Download Lecture Overview
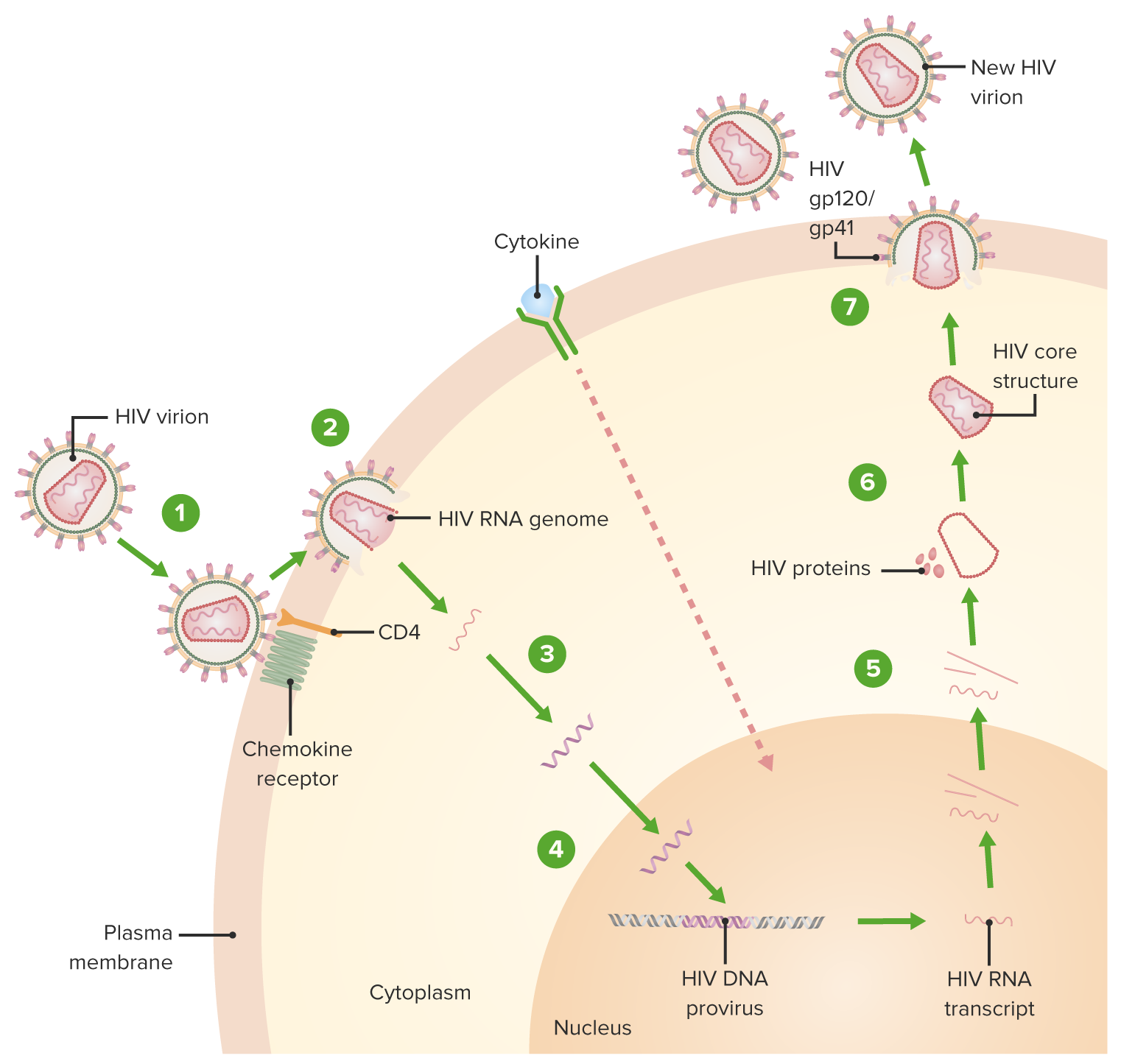
00:01 Today we'll discuss HIV treatment, focusing on how different drug classes target specific steps in the HIV life cycle. 00:08 Understanding this is crucial because modern HIV therapy relies on combining drugs that work at different stages of viral replication. 00:15 Hiv has six key life cycle steps. 00:18 It starts with viral entry, then moves through reverse transcription, integration into host DNA replication, assembly, and finally budding and maturation. 00:28 We have drugs that target each of these steps. 00:30 Let's start with the foundation of HIV treatment the NRTIs, or Nucleoside Reverse Transcriptase Inhibitors. 00:38 We call these the backbone because they're the base of most regimens. 00:42 They're always used in pairs. 00:44 Common combinations include tenofovir with emtricitabine or abacavir with lamivudine. To this backbone we add a third agent. 00:51 Today, the preferred choice is usually an Integrase Inhibitor or INSTI. 00:56 Drugs like bictegravir and dolutegravir have become first line options because they're both powerful and well-tolerated. 01:03 There's even a new monthly injectable option combining cabotegravir with rilpivirine. Non-nucleoside Reverse Transcriptase Inhibitors or NNRTIs, now represent another important class. While efavirenz, rilpivirine, and doravirine can be used first line. 01:21 We keep etravirine in reserve for resistant cases. 01:25 This lecture will focus on this class of drugs. 01:27 Protease Inhibitors remain important, especially in treatment failure. 01:32 One key point they always need a boosting agent, either ritonavir or cobicistat, to achieve effective levels. 01:39 Finally, for multi-drug resistant HIV, we have newer agents targeting different parts of the viral life cycle. 01:46 Drugs like lenacapavir targeting the capsid and attachment inhibitors like fostemsavir and ibalizumab. 01:52 We also have some older agents like maraviroc and enfuvirtide, though these are rarely used today. 01:59 The key takeaway is that modern HIV treatment relies on combining these agents strategically, typically using two NRTIs as a backbone plus a third agent, usually an integrase inhibitor. 02:11 Let's move on to the NNRTIs, which represent a different category within the reverse transcriptase family. 02:17 These NNRTIs bind to a site other than the nucleoside-based or nucleotide-based reverse transcriptase inhibitors. A key distinction that sets them apart from NRTIs. 02:30 They don't require phosphorylation to be activated, which is an important difference between this class and NRTIs. 02:37 There's no cross-resistance with NRTIs, but if NNRTIs are used as monotherapy, resistance can occur rapidly via mutation in the pol gene. 02:49 The image illustrates the mechanism of action of Non-Nucleoside Reverse Transcriptase Inhibitors, NNRTIs, in inhibiting the replication of HIV. NNRTIs function by binding directly to the reverse transcriptase enzyme, which is responsible for converting viral RNA into DNA, a critical step in the HIV replication process. By binding to the reverse transcriptase. 03:15 The NNRTI induces a conformational change that denatures the enzyme, rendering it unable to produce viral DNA. 03:23 This effectively halts the replication of the virus. 03:27 The image highlights key components such as the viral RNA, reverse transcriptase and the binding of the NNRTI to the enzyme, emphasizing the disruption of the enzyme's function. 03:38 Now, I want to emphasize that this is not a category of drugs that's used on its own. 03:42 It tends to be used as part of a regimen. 03:45 The first generation NNRTIs include efavirenz, nevirapine, and delavirdine. 03:53 Let's start with efavirenz, which can be given once a day. 03:58 It's metabolized by cytochrome P450 enzymes, and drug interactions are common with this medication. 04:04 Be aware of that. Toxicity and side effects can occur, including neurological symptoms such as CNS dysfunction, vivid dreams, and dizziness. 04:14 Peripheral neuropathies and skin rashes can also occur. 04:17 Efavirenz should be avoided in pregnancy, especially in the first trimester, due to potential teratogenic effects. 04:24 Efavirenz can also increase serum cholesterol levels, so you'll need to monitor lipid panels regularly. 04:30 Nevirapine is another first-generation NNRTI, often used in three-drug regimens and for preventing vertical transmission from mother to child. 04:39 However, toxicity and side effects are significant concerns, especially skin reactions like rash and the rare but severe Stevens-Johnson syndrome. And if you go back to our early pharmacology lectures, you'll realize that t3A4 and 2D6 comprise the majority of drug metabolism pathways in the human body. 05:00 Blood levels are increased, with drugs like ketoconazole or the azole antifungal agents, and some antibiotics, including the macrolides as well. 05:12 Blood levels are decreased by by taking oral antacids, by DDI, by drugs like Dilantin or phenytoin, rifampin and others. So you have to be very aware of drug interactions when you're giving this medication. The other problem with this pill is that it will affect your warfarin levels through the 2D6 pathway. 05:34 So you have to monitor your INRs if they are also on warfarin. 05:39 Toxicity can include skin problems such as skin rash, and that can occur in up to a fifth of patients. 05:45 And of course, in terms of patients who are pregnant, this can be a potentially teratogenic agent. 05:50 So you cannot use it in patients who may get pregnant. 05:55 Drug interactions are also a major concern with nevirapine, as it is metabolized by both CYP3A4 and CYP2D6. 06:04 Now let's move on to the second generation NNRTIs, which have a different resistance profile. 06:10 These second generation agents were specifically designed to overcome common resistance mutations that limit the efficacy of first generation NNRTIs, like efavirenz and nevirapine. 06:21 Etravirine is especially useful for patients with drug-resistant HIV. 06:25 It’s a substrate and inducer of cytochrome P450 enzymes, so drug interactions are significant. 06:31 Toxicity of Etravirine can include skin rash, which is generally mild but can be severe in rare cases. 06:38 Diarrhea is another potential, though less common, side effect. While Etravirine is not classified as a teratogenic agent, caution is advised when prescribing it to pregnant women. 06:48 Routine monitoring of serum cholesterol levels is not specifically required for Etravirine. Rilpivirine is an important antiretroviral drug for HIV treatment. There are several critical points that determine its success or failure in clinical practice. First, patient selection is crucial. 07:05 Rilpivirine can only be used in patients with viral loads less than 100,000 copies per milliliter. 07:12 This is a firm restriction that you must remember. 07:15 The most critical aspect of Rilpivirine therapy is how it's taken. 07:20 It absolutely must be taken with food because it requires stomach acid for absorption. 07:25 In fact, this is so important that treatment will fail if patients take it on an empty stomach. Following from this, we can't use it with drugs that reduce stomach acid. So PPIs and other acid reducers are contraindicated. 07:38 For side effects, remember three key ones which can lead to dangerous heart arrhythmias like torsades de pointes, depression, and rash. 07:46 When comparing it to other drugs in its class, the key comparison is with Efavirenz. 07:51 Rilpivirine has fewer CNS effects, making it a better choice for patients concerned about neurological side effects. 07:58 Like many HIV medications, it's metabolized through the CYP3A4 pathway, so watch for drug interactions. 08:06 The good news is it's a once daily medication which helps with adherence. 08:10 Just remember always with food. 08:12 Let's discuss Doravirine one of our NNRTIs for HIV treatment. 08:19 Let's start with the basics. 08:21 Doravirine is a once daily medication that works through the CYP3A4 pathway. Most patients tolerate it well, with only mild side effects like nausea, dizziness, and headache. Where this drug really shines is in comparison to other NNRTIs. 08:38 Compared to rilpivirine, Doravirine has three key advantages. 08:42 First, you can use it regardless of viral load. 08:45 There's no upper limit like rilpivirine less than 100,000 copies per milliliter restriction. Second, patients don't need to take it with food. 08:53 Third, you can use it with PPIs is. 08:55 This is a big advantage for patients who need acid reducers. 08:59 When we compare it to efavirenz, the main advantage is neurological. 09:03 Doravirine has fewer CNS side effects, making it a better choice for patients concerned about neuropsychiatric symptoms. 09:10 In summary, think of Doravirine as the more flexible NNRTI with fewer restrictions and better tolerability.
About the Lecture
The lecture Anti-HIV Agents: Non-nucleoside Reverse Transcriptase Inhibitors (NNRTIs) – Antiviral Drugs by Pravin Shukle, MD is from the course Antimicrobial Pharmacology.
Included Quiz Questions
Which drug is a non-nucleoside reverse transcriptase inhibitor?
- Efavirenz
- Lamivudine
- Zalcitabine
- Tenofovir
- Emtricitabine
What is a significant concern when using first-generation NNRTIs like efavirenz?
- Low barrier to resistance, often requiring only a single mutation
- Risk of renal toxicity
- Requires specific food conditions for absorption
- Ineffectiveness against HIV-1
- High risk of hepatotoxicity
Coadministration of which drug will increase blood levels of delavirdine?
- Macrolides
- Phenytoin
- Rifampicin
- Haloperidol
- Carbamazepine
Author of lecture Anti-HIV Agents: Non-nucleoside Reverse Transcriptase Inhibitors (NNRTIs) – Antiviral Drugs

Pravin Shukle, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
