Playlist
Show Playlist
Hide Playlist
Myxedema Coma with Case

-
Slides Thyroid Disease.pdf
-
Reference List Endocrinology.pdf
-
Reference List Thyroid Disorders.pdf
-
Download Lecture Overview
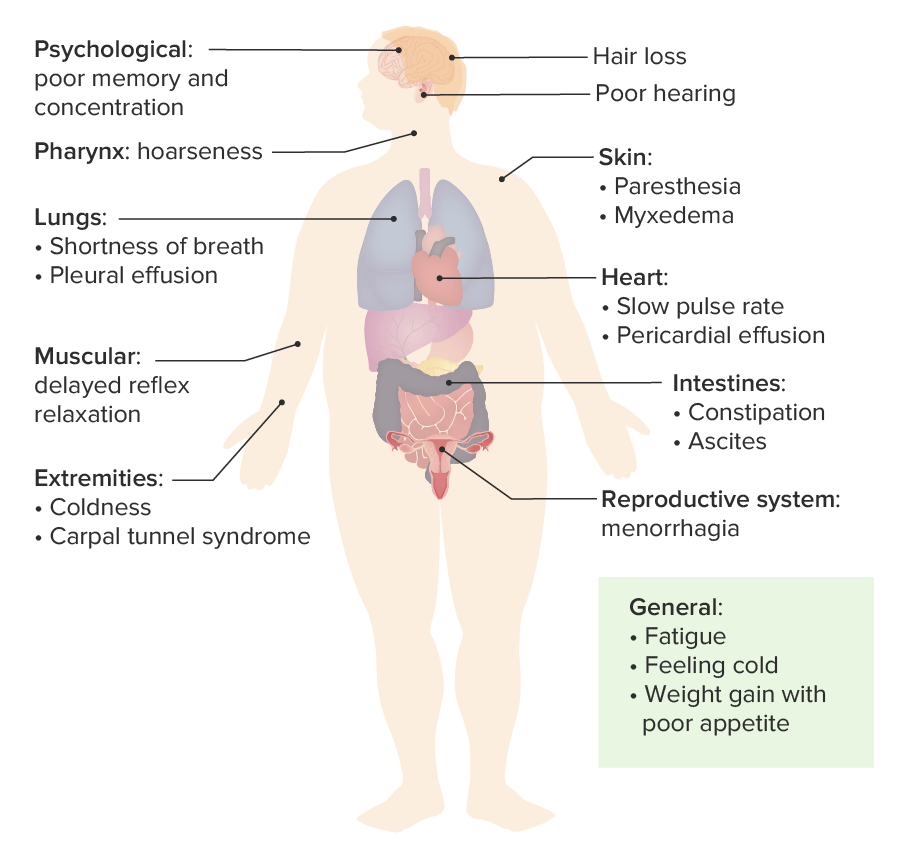
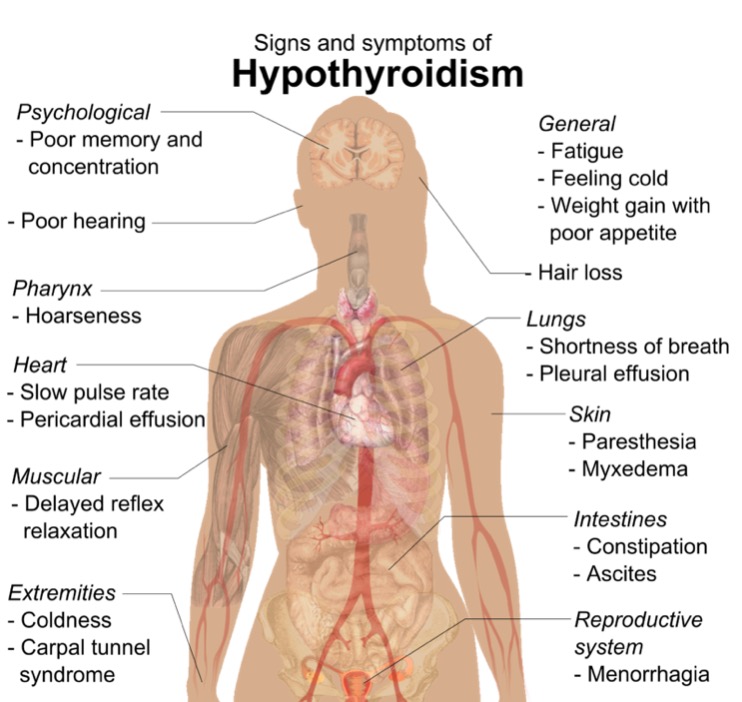
00:01 In this case, a 78 year old woman presents to the emergency department unresponsive. 00:07 Per her family, she has become progressively more lethargic and confused. 00:12 She lives alone and has not taken her medications for some time. 00:16 She had a thyroidectomy 4 years ago for a multinodular goiter. 00:20 On exam, we find a temperature of 36 degrees celsius, a blood pressure of 77/40 and a heart rate of 50 beats per minute accompanied by a respiratory rate of 8 breaths per minute. 00:34 Her BMI is 28. 00:36 She is arousable to painful stimuli, skin color is cool and dry and she is diffusely edematous. 00:44 Her deep tendon reflexes display delayed relaxation phase. 00:50 Her serum sodium and glucose are both low. 00:53 What is the most likely diagnosis in this patient? This is an elderly woman who manifest with progressive lethargy, confusion and then ultimately, unresponsiveness. 01:05 She is known to be hypothyroid and has not taken her medications. 01:11 On exam, she is hypotensive, bradycardic and has a low respiratory rate. 01:16 Her skin is cool, dry and edematous and her neuro exam is notable for delayed relaxation phase of the deep tendon refelxes Her labs are real hyponatremia and hypoglycemia. 01:31 Putting this all together, this most likely fits with a condition known as myxedema coma. 01:37 This presentation is also very similar to hypoadrenalism or low cortisol. 01:43 Myxedema coma, although a rare condition is an extreme presentation of hypothyroidism and can lead to life-threatening secondary systemic decompensation. 01:53 Mortality rates are as high as 20-25%. 01:57 Precipitating factors include myocardial infarction, significant infections, strokes, trauma, gastrointestinal bleeding, metabolic derangements and cold exposure. 02:11 Myxedema coma is much more common in elderly women and patients with a history of hypothyroidism. 02:18 How does one treat myxedema coma? First of all, because of the similarities in presentation, always rule out adrenal insufficiency. 02:27 This can be done by checking the cortisol level. 02:30 While the cortisol level is pending, always provide an empiric dose of hydrocortisone because hypoadrenalism is a significant condition and should be treated early. 02:41 Supportive care and mechanical ventilation with vasopressors may be required as well as the patient is unresponsive or comatose. 02:50 Also find the precipitating event. 02:52 Send off labs, do other investigations to try to make that diagnosis. 02:57 Restoration of the euthyroid state should be achieved by giving thyroid hormone to the patient. 03:04 And then finally, warmed intravenous fluids and a space blanket will help with the hypothermia.
About the Lecture
The lecture Myxedema Coma with Case by Michael Lazarus, MD is from the course Thyroid Disorders. It contains the following chapters:
- Case 1.7
- Myxedema Coma
Included Quiz Questions
Which of the following features in a patient's history or physical examination is most suggestive of myxedema coma?
- History of previous thyroidectomy
- Hyponatremia
- Altered mental status
- Age > 65 years
- Bradycardia
When myxedema coma is suspected based on history and physical exam, what is the best next step?
- Check cortisol level and give a dose of hydrocortisone
- Check ADH levels
- Give IV epinephrine
- Obtain an MRI of the brain
- Obtain CT of the chest, abdomen, and pelvis
What is the most likely diagnosis in the case described below? A 78-year-old woman presents to the ED unresponsive. She has become progressively more lethargic and confused, lives alone, and has not taken her medications for some time. Medical history: Thyroidectomy 4 years ago for multinodular goiter. Physical examination: temperature of 36°C (96.8°F), blood pressure of 77/40 mm Hg, HR of 50 beats/min, respiratory rate of 8 breaths/min, BMI of 28 kg/m2. She is arousable to painful stimuli and is diffusely edematous, her skin is cool and dry, and deep tendon reflexes display delayed relaxation phase. Laboratory test results: low serum sodium and glucose levels.
- Myxedema coma
- Adrenal insufficiency
- Thyroid hormone resistance
- Thyroid storm
Author of lecture Myxedema Coma with Case

Michael Lazarus, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
