Playlist
Show Playlist
Hide Playlist
Mycoplasma Pneumonia in Children

-
Slides Pneumonia Alverson.pdf
-
Download Lecture Overview
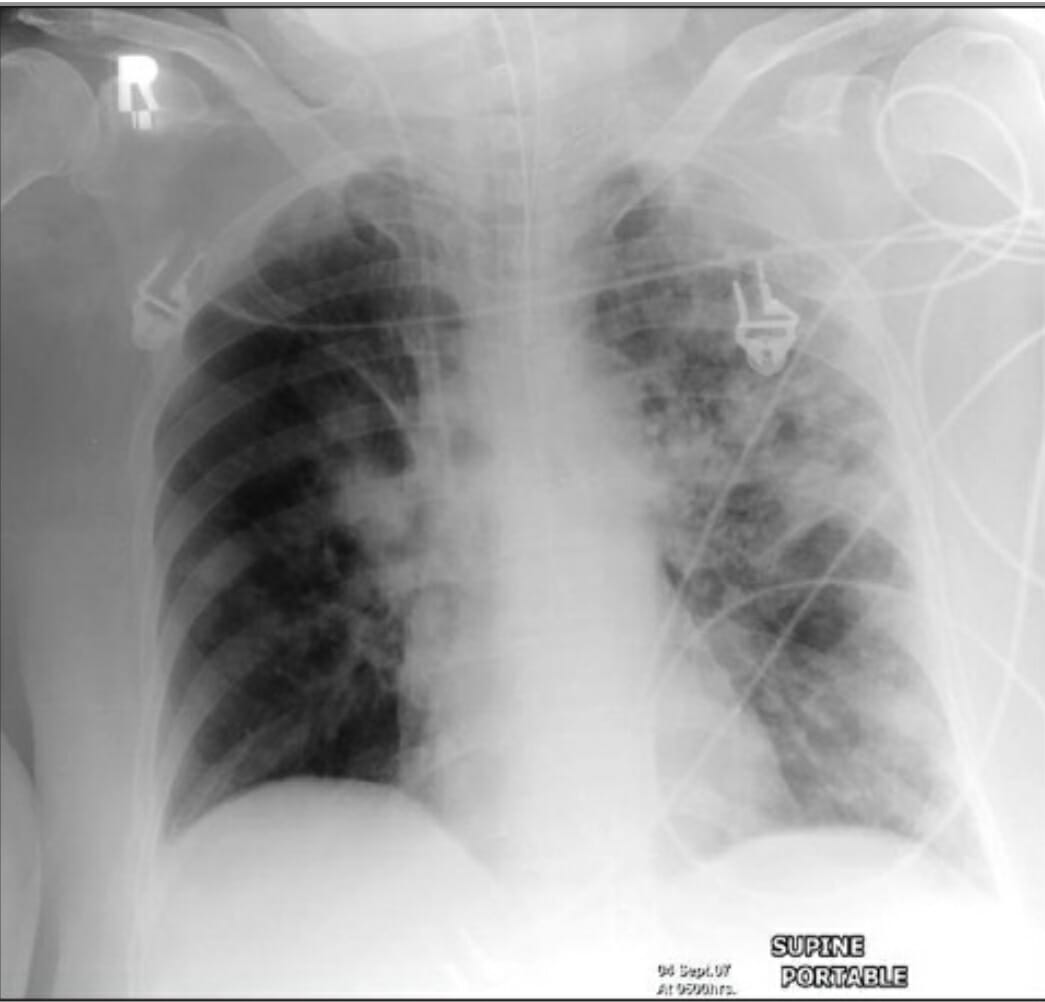
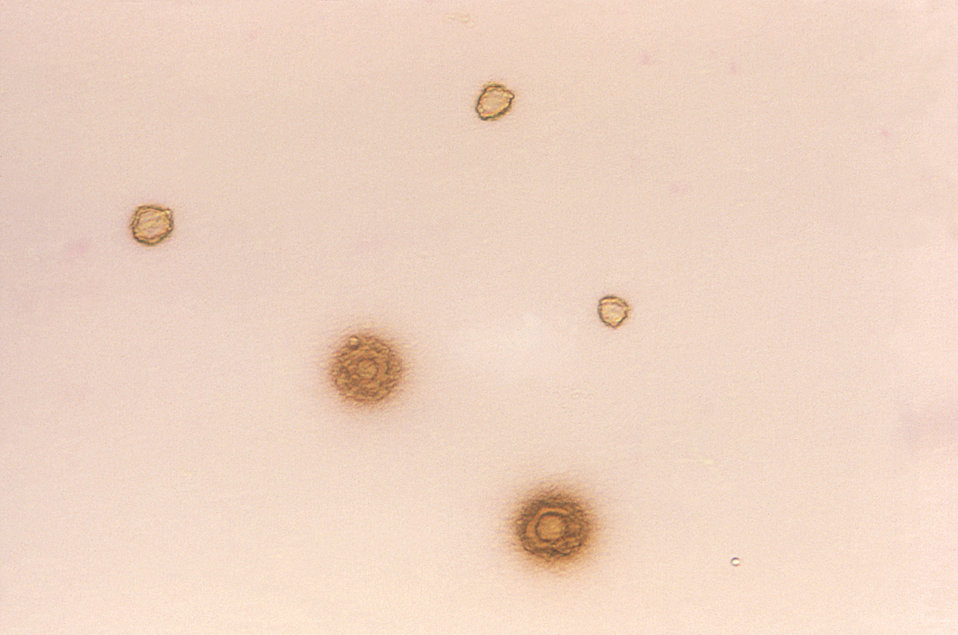
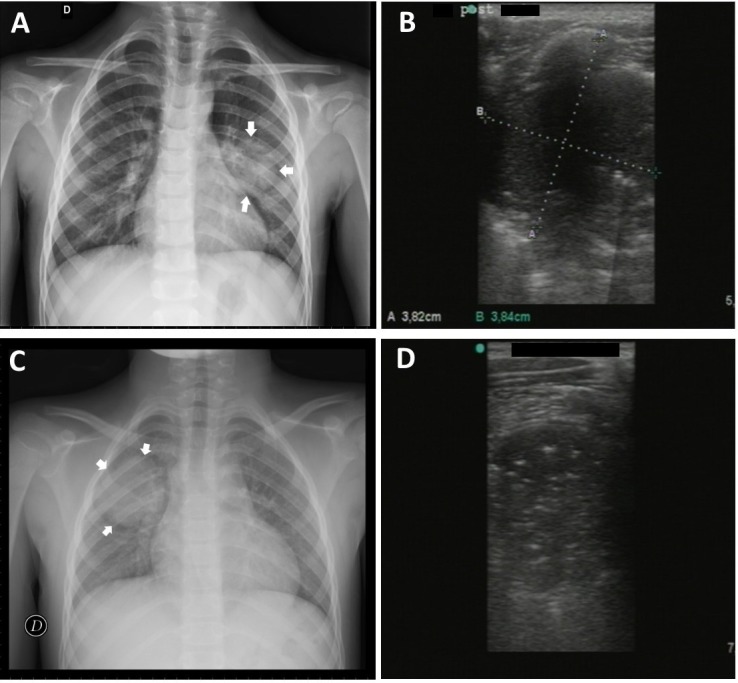
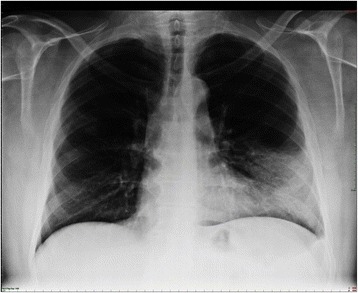
00:00 Let's shift gears and talk a little bit about Mycoplasma Pneumonia and I think this is a confusing area and an area where the evidence in pediatrics is only just starting to getting generated and it's maybe showing that this isn't as big a problem as we might have suspect it. First, you will have heard children under 5 don't get Mycoplasma. That's not true. They do but at a lower rate and there have been outbreaks where they get them at the same rate. So, it really depends on what's going on. Next, you may have heard that Mycoplasma pneumonia causes walking pneumonia. 00:36 So if they're walking around that's probably Mycoplasma. Okay, yes, but it also causes, for example, asthma exacerbations where there is no pneumonia at all or it can cause a lobar pneumonia. So you really don't know what's a Mycoplasma pneumonia and what's not based on history. Next, you may have heard that Mycoplasma pneumonia has a typical diffuse patterned x-ray appearance. Simply not true. Can look any way at once, in fact in 1 study 10% of pneumonias with <i>Mycoplasma</i> had an effusion. Next, there's a myth and I am saying this that it responds to azithromycin. We have no evidence that Mycoplasma pneumonia gets better with azithromycin in children. It may well be that it gets better because of anti-inflammatory properties of azithromycin. So it's unclear that even treating <i>Mycoplasma</i> makes a difference. The reality is <i>Mycoplasma</i> largely gets better on its own. It follows up having more typical of viral illness. It's less likely to actually need antimicrobials. <i>Mycoplasma</i>, if you do wish to test it, is best tested in most centers by simply checking for a rise in titers but the problem is you need a second set of titers, something like 6 weeks later. So what's the point in making a diagnosis 6 weeks after you've already treated the illness? There is a rapid viral PCR that is available and it seems to roughly correlate with the disease so if you have that you could certainly get it. But the typical clinical picture of <i>Mycoplasma</i> is largely unproven and most children have viruses and get better while on azithromycin because the viruses got better and kids who aren't treated probably get better on its own so it's not clear that <i>Mycoplasma</i> is as big a deal as we think it is and you probably can miss the diagnosis just fine. Azithromycin, you generally will treat for a 5-day course. Azithromycin is not effective against other bacterial causes. So if you think this might be <i>Pneumococcus</i> you'd be wiser to treat the <i>Pneumococcus</i> than the <i>Mycoplasma</i>. It's unclear who we should treat and who we should not treat and whether azithro even affects the course of illness. It does kill bacteria in vitro but in vivo the infection seems to be more of a post infectious inflammatory condition in many settings of <i>Mycoplasma</i> especially ADEM and other diseases that happen after the disease. The lung disease, it may be beneficial or not and there actually is some evidence that maybe steroids would be effective for Mycoplasma pneumonia. That really hasn't been a study, I wouldn't recommend it but keep in mind that might be on the horizon.
About the Lecture
The lecture Mycoplasma Pneumonia in Children by Brian Alverson, MD is from the course Pediatric Infectious Diseases.
Included Quiz Questions
Which of the following is true about mycoplasma pneumonia?
- Children under 5 can have mycoplasma pneumonia.
- Mycoplasma most commonly causes walking pneumonia.
- Mycoplasma causes a diffuse pattern on chest x-rays.
- Mycoplasma pneumonia rapidly responds to azithromycin in children.
- Mycoplasma pneumonia does not exist in children.
Which of the following test has a rapid response time and is reliable in providing the diagnosis of mycoplasma pneumonia?
- PCR
- Mycoplasma antibody rise in titres
- Sputum culture
- Chest x-ray
- Gram stain on sputum sample
Author of lecture Mycoplasma Pneumonia in Children

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excellent lecture. Really helps to dispel all the myths around M. pneumoniae. It does really seems like management is going to change in the upcoming years regarding this disease.
