Playlist
Show Playlist
Hide Playlist
Types of Ovarian Tumors: Mature Teratoma


-
Slides Ovary Female Repro.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
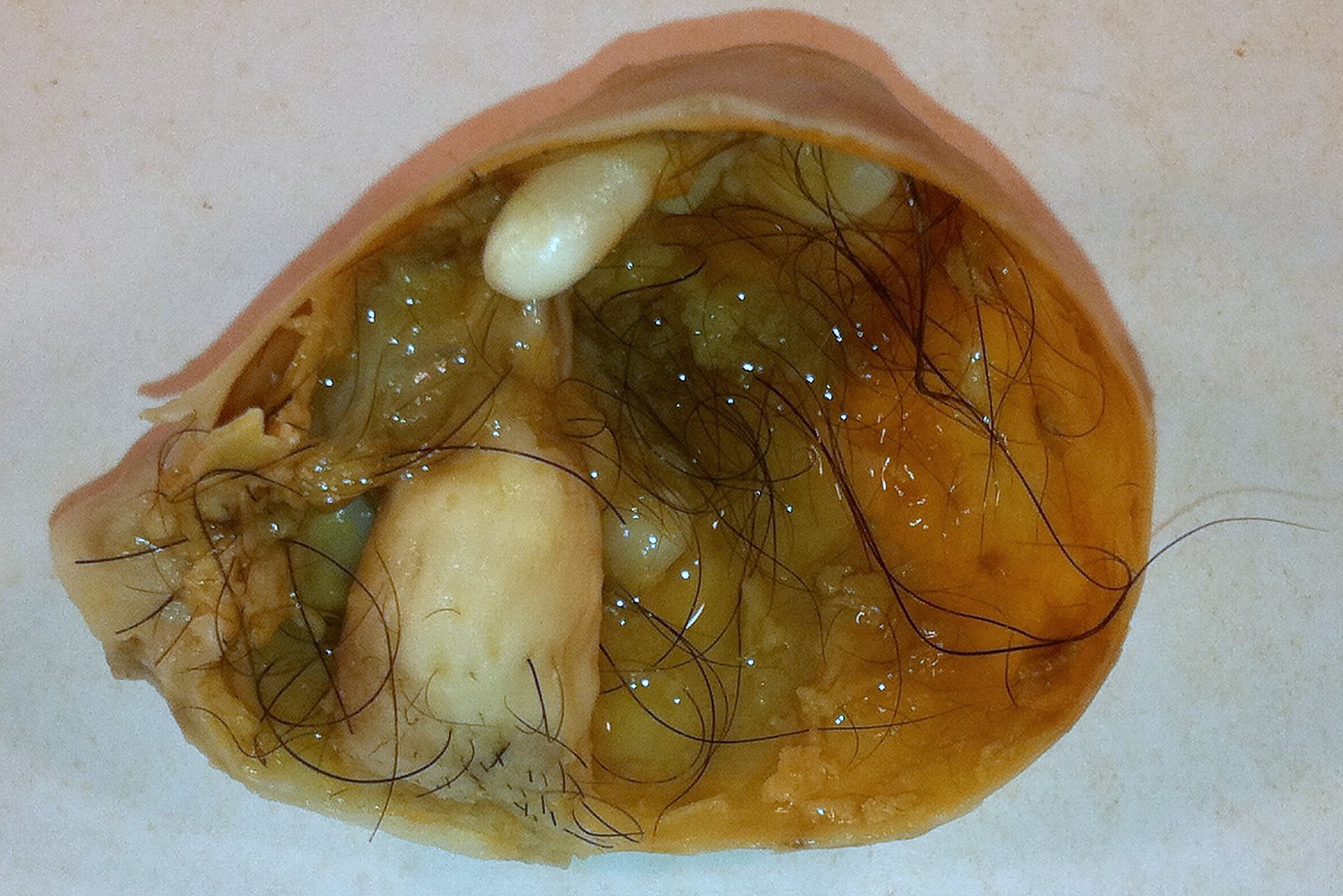
00:01 Let’s go ahead and talk about that mature teratoma. 00:04 A cystic neoplasm made up of tissue elements from two or more embryonic layer. 00:10 In other words, we’re talking about a tumor in which it’s a driving your different germ layers, mesoderm, ectoderm, endoderm. 00:18 You can see skin, hair, bone, all kinds of issues. 00:21 The most common type of germ cell tumor in a female. 00:24 Female. 00:25 The most common germ cell tumor in a male, once again, I sound like a broken record, seminoma. 00:31 Also known as dermoid cyst. 00:33 I would know both names, absolutely know both names. 00:36 A mature teratoma in a female tends to be benign whereas teratoma in a male will be malignant. 00:43 That’s important. 00:44 What does that mean? Next step of management. 00:47 If it’s a teratoma that you would find in a testicle, you just resect it. 00:52 That’s your next step, surgery, resection. 00:54 Do not waste time conducting further investigation. 00:59 Whereas if with the female, maybe perhaps you want to do grading. 01:01 So there is a little bit of followup and such as necessary. 01:07 10 to 15% of these tend to be bilateral. 01:09 1% may then go onto malignant transformation. 01:12 Usually, it will be squamous cell cancer. 01:16 The subtypes of teratoma will contain only thyroid. 01:19 That’s interesting. 01:21 Our topic here, we did endocrinology and we did thyroid. 01:25 There is struma ovarii. 01:27 So you have a teratoma here. 01:28 T – teratoma – will produce T3, T4. 01:35 Notice I did not say TSH. 01:38 So there might be actual thyroid tissue in the ovarian teratoma, directly producing T3 or T4. 01:47 You tell me, does that behave like primary or secondary hyperthyroidism? Very good. 01:54 Primary. 01:55 If it’s a directly producing T3 and T4 with struma ovarii, you’d expect the TSH levels to be low, just as you would with primary. 02:05 Always unilateral would be struma ovarii. 02:08 Make sure you know this subtype. 02:09 Make sure you know the name and what it’s doing. 02:14 A mature cystic teratoma, upon gross examination, maybe it’s combing its hair. 02:19 Maybe it’s giving you a wink You know maybe it’s smiling at you. 02:22 So this is a tumor that produces every single type of tissue, cartilage, retina, maybe hair. 02:29 Get the point. 02:31 Upon your histologic examination, you would expect to find different types of histology because you might have derivation from ectoderm, endoderm, mesoderm. 02:43 An immature malignant teratoma. 02:47 You’d find this to be interesting. 02:48 Immature teratoma known as a dermoid cyst is almost always benign. 02:54 Immature. 02:55 Our topic here is im-mature. 02:58 Automatically going to malignancy, these patients are found prepubertal, adolescents and young women. 03:04 Varying amounts of immature tissue, differentiation towards cartilage, gland, bone, muscle, nerves. 03:10 Yes, you can have different types in both. 03:12 But this tends to be more confusing or more abundant of all kinds of tissue. 03:19 And more importantly, this is malignant. 03:22 Immature tissue. 03:23 Immature. 03:25 We have a dysgerminoma next. 03:27 A dysgerminoma is equivalent to a seminoma in a male. 03:32 Extremely important. 03:33 A tumor consisting of large cells with clear cytoplasm and well-defined borders. 03:39 Dysgerminoma.
About the Lecture
The lecture Types of Ovarian Tumors: Mature Teratoma by Carlo Raj, MD is from the course Ovarian Diseases.
Included Quiz Questions
Which of the following tumors is MOST likely to be malignant?
- Immature teratoma
- Mature teratoma
- Dermoid cyst
- Struma ovarii
- Cystic adenoma
Which of the following statements about struma ovarii is CORRECT?
- It is always unilateral.
- It behaves like secondary hyperthyroidism.
- T3/T4 levels are likely to be decreased.
- TSH levels are likely to be elevated.
- It is a type of epithelial cell tumor.
Which of the following statements about mature teratomas is INCORRECT?
- In men, they are most often benign.
- One percent will undergo malignant transformation, usually squamous cell carcinoma.
- In women, they are most often benign.
- They contain at least 2 embryonic layers.
- Ten percent to 15% are bilateral.
Which of the following BEST describes the tumor found in a patient with dysgerminoma?
- Large cells with clear cytoplasm and well-defined borders
- A solid tumor composed of endometrial-like glands
- Cystic tumor filled with mucinous/gelatinous material
- Cystic tumor filled with at least 2 or 3 embryological layers
- Cystic tumor lined by tall, columnar epithelial cells
Author of lecture Types of Ovarian Tumors: Mature Teratoma

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
