Playlist
Show Playlist
Hide Playlist
Malignant Breast Diseases

-
Slides MalignantBreastDiseases Surgery.pdf
-
Download Lecture Overview
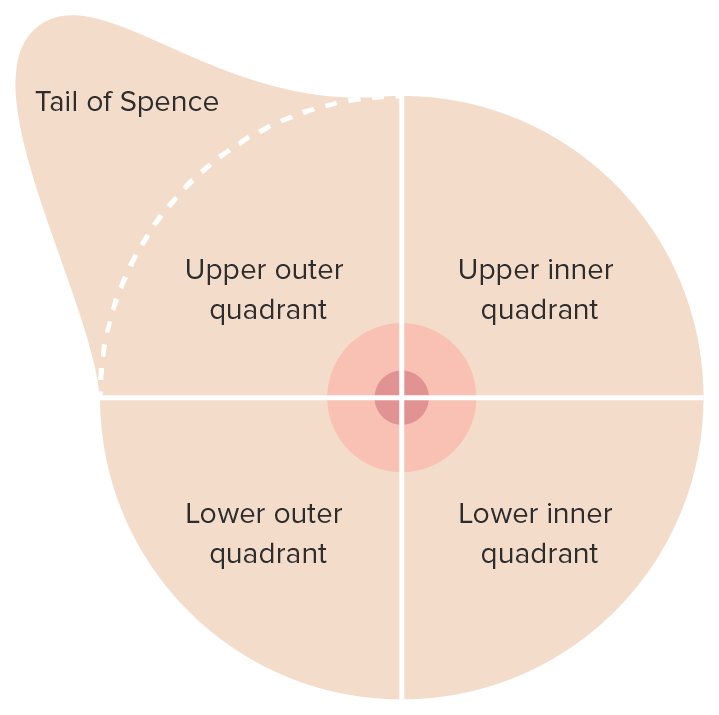
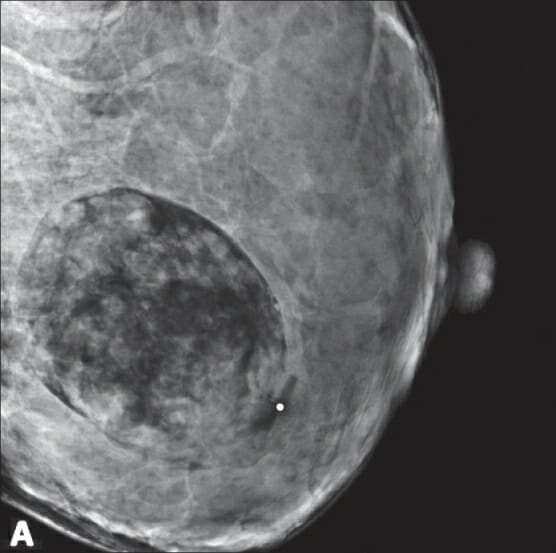
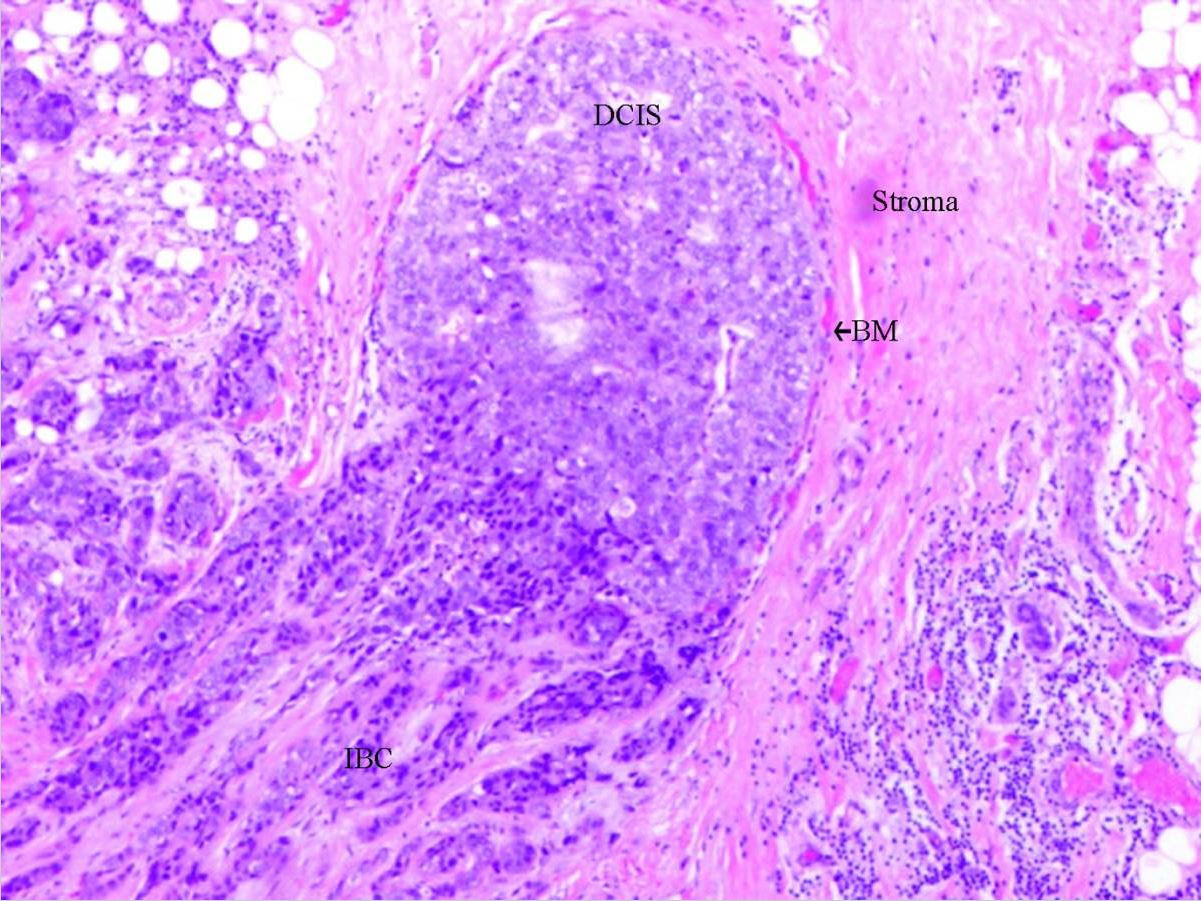
00:01 Welcome back. 00:02 Thanks for joining me on our discussion on malignant breast disease in this section of general surgery. 00:07 Much like we discussed in the benign lecture, breast masses are typically thought of as either benign or malignant. 00:16 We discussed benign breast masses in a different module. 00:20 In this one we’ll discuss malignant. 00:23 It’s important to focus on both in situ disease and invasive disease and there's also the special presentation of inflammatory breast cancer. 00:31 Remember the most important decision in breast masses is whether it’s benign or malignant. 00:36 As a review, we always wanna start by obtaining a careful history. 00:42 This is particularly important with patients that had family histories of breast cancer. 00:47 We’ll perform a thorough examination of both the breast bilaterally as well as on lymph node draining basins. 00:54 Then we obtain age appropriate diagnostic imaging whether it's an ultrasound or a mammogram. 01:01 Remember, obtaining this imaging before disturbing the anatomy with the tissue biopsies. 01:07 Then, we obtain tissue biopsies to guide the next step in management. 01:12 We put all these information together and we introduce an optimal treatment plan to the patient. 01:18 For palpable lesions biopsies are easy, but for non-palpable lesions, biopsies may require additional image guidance. 01:30 Physical findings are important in physical examinations important. 01:35 We wanna disrobe the patient and examine both breasts for symmetry as well as for masses and now we wanna look up the draining lymph node basins focusing particularly on the supraclavicular, behind the pectoralis muscles as well as in the armpit. 01:52 Again, laboratory values routine in nature are usually not very helpful. 02:00 These include chemistries and CBCs. 02:04 Here’s an image of an ultrasound. 02:07 Again, ultrasounds are especially useful in young patients. 02:10 Anechoic lesions on an ultrasound mean that it’s likely to be fluid field and potentially just a benign cyst. Here’s a mammogram. 02:22 In these series of three images you see microcalcifications in a suspicious mass. 02:28 Mammograms are assigned a BI-RADS classification for it’s suspicion for a breast cancer. 02:35 Let's move on to a discussion of ductal carcinoma in situ, also known as DCIS. 02:43 DCIS is considered a neoplastic process but importantly it is confined to the ducts alone. 02:50 It is one of the most common diagnoses and due to the increase detection rates since the introduction of mammography for screening. 02:58 It may be shocking to you but screening mammograms is not used to be the standard of care. 03:03 On mammograms, DCIS like these two images, may show itsekf as microcalcifications. 03:15 It is however difficult to distinguish these from invasive cancers based on imaging alone, therefore biopsies are necessary, again, to differentiate between a palpable versus a non-palpable. 03:30 In the vast majority of cases DCIS will not present itself as a palpable lesion. 03:36 However, if you do have a palpable mass, it is amenable to a needle core biopsy. 03:42 And of course with non-palpable masses, we can perform a stereotactic biopsy with 3D reconstruction image-guided biopsy. 03:51 This lessens the need for a surgical excision of biopsy. 03:55 Excision is recommended for DCIS if it’s obtained on pathology. 04:02 Patients with DCIS are absolutely candidates for breast conservation therapy. 04:08 Breast conservation therapy involves partial mastectomy, removing a portion of the breast potentially also assessing the lymph node and this needs to be followed up with radiation and chemotherapy. 04:22 Postoperative endocrine therapy is usually offered to the patients with DCIS. 04:27 This may include Tamoxifen. 04:30 Once again, breast conservation therapy involves a local excision to include negative margins. 04:38 Patients have to have a postoperative radiation. 04:42 In fact, if the patient is not candidate for radiation therapy or does not want postoperative radiation therapy, they are not candidates for breast conservation therapy. 04:53 The results or in outcomes are equivalent to mastectomy - in the choice of mastectomy, maybe a personal one. 05:00 We certainly have patients who are diagnosed with DCIS or breast cancer but chose to have a mastectomy rather than breast conservation therapy.
About the Lecture
The lecture Malignant Breast Diseases by Kevin Pei, MD is from the course General Surgery.
Included Quiz Questions
What constitutes an appropriate physical exam for a patient with a primary complaint of a breast lump?
- Evaluation of both breasts and bilateral lymphatic basins for the breast, including bilateral axillary, subpectoral and supraclavicular nodes
- Evaluation of the affected breast only
- Evaluation of the affected breast and the axillary lymph nodes
- Obtain imaging prior to performing a physical examination
- Evaluation of both breasts only
Which of the following describes the appearance of a cyst on ultrasound?
- Anechoic lesion
- Hyperechoic lesion
- Pulsatile lesion
- Rim-enhancing lesion
- Microcalcifications within the lesion
How does ductal carcinoma in situ usually present?
- As microcalcifications on screening mammography
- As a palpable mass
- As a hypoechoic lesion on ultrasound
- As breast pain
- As abnormal breast discharge
Which of the following is not part of breast conservation therapy for ductal carcinoma in situ?
- Total mastectomy
- Partial mastectomy
- Radiation therapy
- Chemotherapy
- Postoperative endocrine treatment
Author of lecture Malignant Breast Diseases

Kevin Pei, MD
Customer reviews
3,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
0 |
| 3 Stars |
|
1 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
It would have been good to talk about LCIS as well as DCIS particular as the management differs. Also no discussion of the choice between FNAs and CNB in regards to sensitivity and specificity.
