Playlist
Show Playlist
Hide Playlist
Introduction to Infectious Myopathies with Case

-
Slides Infectious Myopathies.pdf
-
Download Lecture Overview
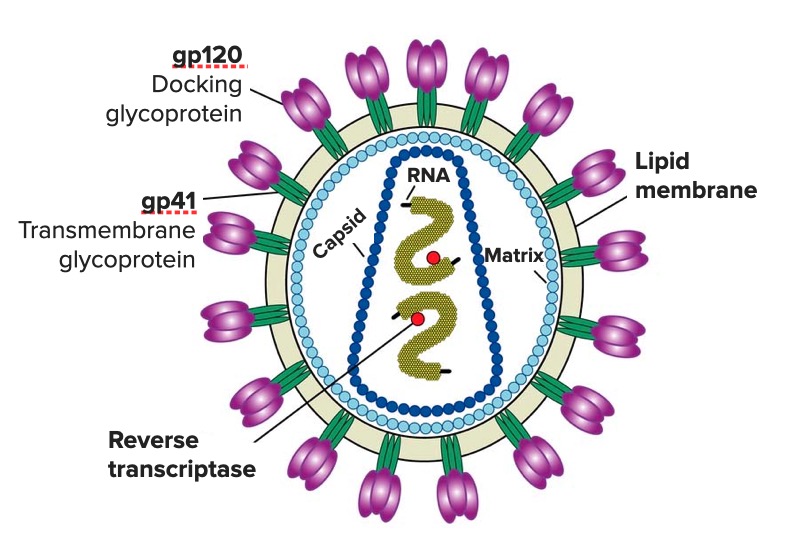
00:00 In this lecture, we're going to review Infectious Myopathies, a rare cause of muscle disorders but important in selected patients. So let's start with a case. This is a 43-year-old man who presents with weakness, and again weakness is a common chief complaint for muscle disorders. This 43-year-old male has a past medical history of migraines and HIV. The HIV was diagnosed 3 months ago, just recently, and he has just started on treatment as you can see. 00:31 He presents for referral for weakness which began about 1 month ago. He describes a slowly progressive proximal symmetric weakness of the legs more than the arms. He also has moderate to severe soreness of the muscles with myalgias. In addition to the muscle complaints, the patient has neuropathic symptoms with mild stocking- glove distribution of numbness, tingling, and burning pain that is worse at night. On examination, he has proximal weakness in the bilateral muscles in the arms and legs that's symmetric. Deep tendon reflexes are reduced 1+ throughout except he has absent reflexes at the bilateral ankle jerks. The sensory examination shows decreased pinprick, temperature, and vibration in a stocking-glove distribution bilaterally and propioception is normal. So we have a myopathic presentation with what seems like superimposed neuropathy given the reduced deep tendon reflexes that's absent at the ankles and the sensory findings. So what's the diagnosis? Let's walk through some of the key features of this case and focus on those key findings that we evaluate for patients with peripheral nervous system disorders. What's the distribution to sensory findings and the reflex exam for this patient? Well, the distribution is primarily proximal. His weakness is proximal involving primarily the legs as well as somewhat the arms. That proximal distribution points us in the direction of muscle. What about sensory findings? Well we do have sensory findings. The patient complains of mild numbness, tingling, and paresthesias and we see those on exam. That we don't expect from a muscle disorder and suggest that there may be superimposed neuropathy or that this proximal distribution of the weakness could be from something other than muscle. How about the reflex exam? Well, the reflex exam shows reduced deep tendon reflexes and absent ankle jerks. That's also a distribution that we see with a nerve complaint. So in summary, it sounds like we have both a myopathic and neuropathic presentation. Workup is performed to evaluate potential causes of this and we see that the HIV viral load is undetectable, his CD4 count is 350. We like to see a CD4 count of greater than 200 or 300. Age is defined as a CD4 count of less than 200. The absence of an HIV viral load suggests that the medication that had just been initiated is likely to be working and is reduced to the total HIV viral load. CK is performed to evaluate for an inflammatory muscle disorder and we see that the CK is elevated to 1200, again with normal being 50-160. And then there's a range of other testing that was performed to look at muscle conditions and neuropathy conditions that could be causing this, serum chemistry, vitamin B12, folate, syphilis testing, thyroid studies, hemoglobin A1c, hepatitis screen, and a serum protein electrophoresis both looking for myopathic and neuropathic causes. All of which are normal. So what's the diagnosis for this patient? Is this an HIV-associated myopathy with distal sensory polyneuropathy, is this dermatomyositis, CIDP or chronic inflammatory demyelinating polyneuropathy, or is this polymyositis? Well this doesn't sound like dermatomyositis. A dermatomyositis that we have discussed presents with prominent rash, either rash on the knuckles or in the face or a shawl sign and we don't see those typical dermatologic findings and dermatomyositis is not strikingly associated with HIV. What about CIPD? CIPD is a neuropathic condition. This is inflammation of the nerve that presents chronically over time. This presentation is not consistent with CIDP. CIDP starts with distal weakness and some sensory findings and progresses proximally. In the condition for our patient began proximally with some distal neuropathic findings. Polymyositis. Polymyositis is a diagnosis of exclusion. That's a myopathic presentation that has no other explanation. And this patient with newly diagnosed HIV, the diagnosis that it suggested is associated with the patient's HIV. So this is a classic presentation of HIV-associated myopathy with a superimposed distal sensory polyneuropathy. So let's think more about some infectious causes of myopathies. Infections in the muscle is uncommon, but we can see many types of infections in this area. We can see bacterial infections or pyomyositis, viral infections or viral myositis, and we'll talk about some of the causative organisms for those. The things I'd like you to focus on in this lecture is HIV-associated myositis, trichenosis-associated myositis because it has a really cool and neat presentation and is sometimes tested on examinations, and then Lyme is another infection that can affect the muscle. We're going to walk through each of these briefly focusing on those conditions that are particularly relevant that you'll see in patients or that sometimes show up on test questions and that you want to be familiar with how to approach the vignette.
About the Lecture
The lecture Introduction to Infectious Myopathies with Case by Roy Strowd, MD is from the course Acquired Neuromuscular Diseases.
Included Quiz Questions
Which of the following clinical features is associated with HIV-associated myopathy?
- Distal sensory neuropathy
- Symmetric distal muscle weakness
- Hyperactive deep tendon reflexes
- Shawl sign
- Loss of pupillary light reflex
Which of the following is diagnosed through the process of exclusion?
- Polymyositis
- Dermatomyositis
- Vitamin B12 deficiency
- HIV-associated myopathy
- Syphilis
Which of the following tests would be abnormal in patients with HIV-associated myopathy?
- Creatine kinase
- Folic acid
- Serum creatinine
- Alkaline phosphatase
- Alanine aminotransferase
Author of lecture Introduction to Infectious Myopathies with Case

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
