Playlist
Show Playlist
Hide Playlist
Introduction – Hypothyroidism

-
Slides Hypothyroidism EndocrinePathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
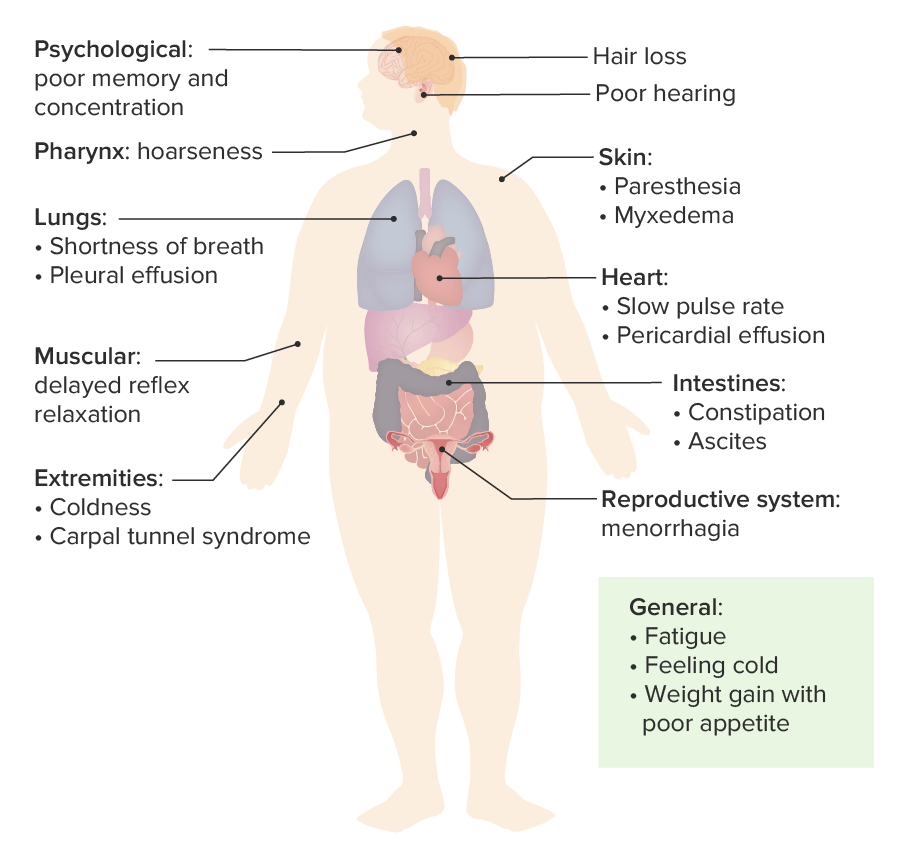
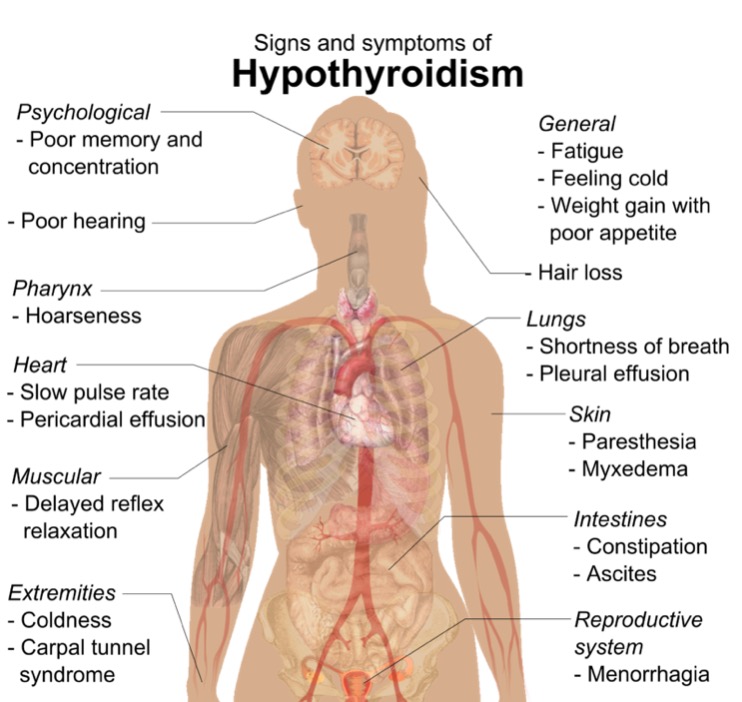
00:01 In this discussion, we will take a look at hypothyroidism. 00:04 Generally speaking, a patient walking through the door will have decreased basal metabolic rate, tired fatigued, constipated, gaining weight without necessarily consumption of too much food. 00:20 Hypothyroidism defined by insufficient circulating thyroid hormone levels for normal cellular functioning, extremely common especially in women due to Hashimoto, a chronic lymphocytic type of thyroiditis. 00:35 At this juncture, you should be able to integrate your complete picture of Hashimoto to the point where initially you may have in a female is experience-is experiencing Hashitoxicosis. 00:46 point where initially you may have a female experiencing Hashitoxicosis. 00:50 Some point in time, with that lymphocytic infiltration may result in hypothyroidism primary type. 00:59 Your patient with hypothyroidism will have puffy face, puffy hands; eye, periorbital region will be puffy. 01:12 Differentiate this from Graves’ disease. 01:15 This is not exophthalmos; mixed edema in all parts of the body. 01:22 There is no pathognomonic sign or symptoms for hypothyroidism. 01:26 Typical patient is lethargic, fatigued, multi… mild constipation, cold intolerance, dry skin, dulled facial expression, puffiness of the face, around the eyes, coarse hair. 01:44 The complexion is going to be yellow because of decreased conversion or decreased metabolism of carotene. 01:54 Do not confuse this with jaundice; this is vitamin A that is not being properly metabolized due-due to decreased T3, T4. 02:05 Loss of lateral eyebrows and that’s an interesting symptom, isn’t it? There will be delayed DTR or delayed relaxation of deep tendon reflexes, growth failure in children because of lack of long bone growth, yellowing of the skin, why? Because of increased carotene accumulation, short stature, extreme, extremely low IQ, galactorrhea, a decrease in T… a decrease in T3, T4 result in increase in TRH and TSH, galactorrhea, a decrease in T… a decrease in T3, T4 result in increase in TRH and TSH, thus resulting in hyperprolactinemia and galactorrhea. 02:42 Hypercholesterolemia, especially LDL, type 2 hyperlipidemia, why? Because if you have decreased T3, T4, the LDL receptors aren’t working properly. 02:55 By definition, what is type 2 hyperlipidemia? It is the fact that the LDL receptors aren’t working properly and one that you are also familiar with is the familial type autosomal dominant where the LDL receptors aren’t working or it could the acquired type, right? Your T3, T4 plays a pivotal role in receptor activity. 03:17 Hoarseness, hypoventilation, dyspnea, sleep apnea, pleural effusion all seen with hypothyroidism. 03:27 Everything is slowed down, there is going to be ileus, the tongue is going to be enlarged called macroglossia. 03:32 Once again, think of that infant with congenital hypothyroidism who is going to then have an enlarged tongue. 03:38 Myalgias, arthralgias, non pitting edemas, depression, psychosis, carpal tunnel syndrome. 03:43 Bunch, a bunch of symptoms and signs that you can expect with hypothyroidism, cannot miss it. 03:51 With hypothyroidism, there might be amenorrhea, anemia, platelet defects, dry skin, and once again, accumulation of carotene. 03:59 This is not jaundice, delayed puberty might occur. 04:03 Continue discussion of signs and symptoms of hypothyroidism. 04:07 You would expect there to find increased systemic vascular resistance. 04:14 Remember that if you did have thyroid hormones normally then as far as your cardiovascular system is concerned, everything is working in sync and you would have the normal effects of the catecholamines. 04:27 The beta 2 receptors normally located on your blood vessels would then cause dilation. 04:32 However, in hypothyroidism, due to lack of your norepinephrine working upon your beta 2 receptors may result in increased systemic vascular resistance. 04:45 This is then confirmed by diastolic hypertension. 04:51 Because the receptors aren’t working properly, you can expect your beta 1 receptors to be not functioning. 04:56 Therefore, there will be decreased anatropy and decreased cardiac output, therefore you would find there to be decreased systolic function. 05:05 Any time there is decreased systolic function, eventually you will also find decreased diastolic function because you cannot properly fill up your heart and that’s a huge physiologic concept, isn’t it? If the receptors aren’t working properly, beta 1 in the heart, your heart rate here would be decreased, bradycardia, and there is a possibility of accumulating fluid in the pericardial cavity, pericardial effusion. 05:32 Let us now talk about hypothyroidism and the different causes. 05:37 The most common is the one that we should cover initially. 05:41 Chronic lymphocytic infiltration of a thyroid gland known as Hashimoto. 05:46 We have silent thyroiditis, there is quite a bit of overlap that will be taking place between a hyper and hypothyroidism in these topics, especially when dealing with thyroiditis and the reason for that is initially you could find hyperthyroid symptoms, may slowly start dropping the T3, T4 into euthyroid phase and then eventually getting into your hypothyroid phase. 06:21 Some may result in permanent hypothyroid or there is a possibility that if it is a viral or your bacterial that we talked about earlier that there might be a recovery phase. 06:34 Hashimoto permanent hypothyroidism. 06:37 The subacute thyroiditis, the reason that we have the term transient is because with subacute, let’s say that is a granulomatous and the viral infection preceded by an upper respiratory tract infection, initially hyperthyroid, exactly the spectrum that I had walked you through just a few minutes ago. 06:59 Acquired causes of hypothyroidism. 07:02 The patient came in with Graves’ disease, the Graves’ disease was then dealt with by radiation therapy. 07:12 There might have been excess thyroid destruction or excess thyroid removal. 07:22 When there is excess destruction of your thyroid gland, this may then result in acquired hypothyroidism, the patient is now placed on thyroid replacement or thyroid hormone replacements. 07:35 Following head and neck radiation therapy and iodine deficiency, much less seen in developed countries, maybe perhaps a patient coming from a developing country where iodine excess might be limited, therefore resulting in acquired type of hypothyroidism. 07:55 Drugs that may cause hypothyroidism include Lithium, Amiodarone, anti-thyroid drugs such as Propylthiouracil, Methimazole or centrally acting such as Sunitinib and Bexarotene. 08:07 Central hypothyroidism arises from issues within the brain's control of the thyroid gland. 08:13 Specifically, there are two types: secondary and tertiary. 08:18 Secondary hypothyroidism occurs when the pituitary gland fails to secrete enough thyroid-stimulating hormone (or TSH), which is critical for prompting the thyroid gland to produce thyroid hormones. Without sufficient TSH, the thyroid doesn't get the signal to produce these hormones, leading to hypothyroidism. 08:38 Moving up the control chain, we encounter tertiary hypothyroidism, which is less common. 08:44 Here, the problem lies with the hypothalamus, which doesn't produce enough thyrotropin-releasing hormone (or TRH). 08:52 TRH is the chemical messenger that tells the pituitary gland to make TSH. 08:58 So, if there's not enough TRH, the entire hormone production process is compromised. 09:04 Congenital hypothyroidism refers to hypothyroidism present at birth and is due to one of several events. 09:12 Thyroid dysgenesis, which can be due to the complete absence of the gland, an underdeveloped gland, or a gland that's not located where it should be, with the latter being the most common of these issues. 09:24 There may be a defect in the synthesis of thyroid hormones due to genetic mutations affecting the hormonal production pathways. 09:31 Lastly, though quite rare, some individuals are producing normal thyroid hormone, yet their body's cells don't respond to the hormone. 09:41 This may be due to mutations, particularly in the thyroid hormone receptor beta gene in target tissues. 09:48 At this point, you broaden your differentials for hypothyroidism beyond Hashimoto’s and we are looking at drugs and secondary, tertiary and congenital. 09:57 Let’s continue.
About the Lecture
The lecture Introduction – Hypothyroidism by Carlo Raj, MD is from the course Thyroid Gland Disorders.
Included Quiz Questions
What is the most common cause of hypothyroidism?
- Chronic lymphocytic thyroiditis (Hashimoto's thyroiditis)
- Pituitary adenoma
- Silent thyroiditis
- Graves' disease
- Iatrogenic causes
Which of the following is NOT a symptom of hypothyroidism?
- Orbital bulging
- Weight gain
- Fatigue
- Constipation
- Yellow complexion
On physical examination, which sign would not be found in a patient with hypothyroidism?
- Hyperventilation
- Delayed relaxation of deep tendon reflexes
- Stunted growth (children)
- Intolerance to cold
- Pleural effusion
What is indicated by the presence of increased systemic vascular resistance in hypothyroidism?
- Diastolic hypertension
- Increased norepinephrine sensitivity
- Decreased diastolic function
- Normal functioning of beta 1 receptors
- Enhanced metabolism of Vitamin A
Where is the source of pathology in secondary hypothyroidism and tertiary hypothyroidism, respectively?
- Pituitary; hypothalamus
- Pituitary; liver
- Hypothalamus; liver
- Hypothalamus; pituitary
- Liver; adrenal glands
Author of lecture Introduction – Hypothyroidism

Carlo Raj, MD
Customer reviews
4,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
1 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I love Dr. Raj videos. They are very engaging and informative.
You should have added histopathology in pathology videos and explain that histopathology
