Playlist
Show Playlist
Hide Playlist
Labor Stage 1: Fetal Heart Rate Tracing

-
Slides FetalHeartRateTracings Obstetrics.pdf
-
Download Lecture Overview
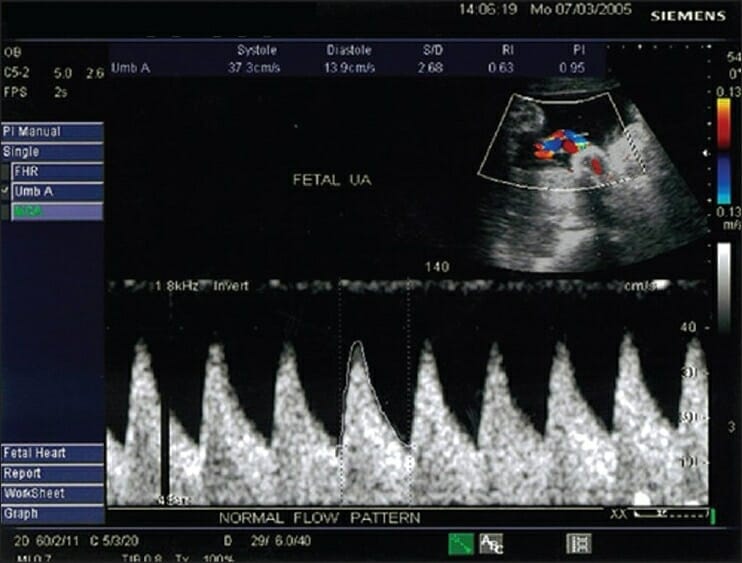
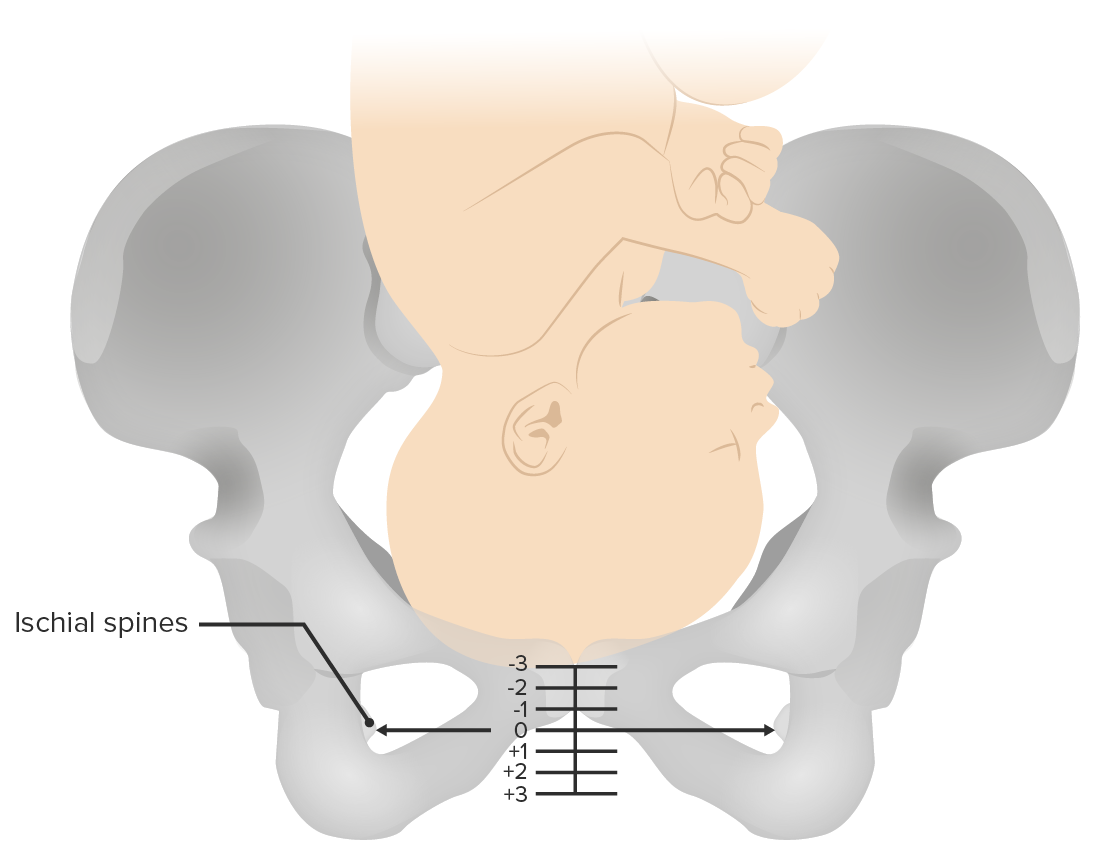
00:01 Now let's discuss the interpretation of fetal heart rate tracings. 00:06 So let's go over some terminology and some nomenclature. 00:09 When we talk about the fetal heart rate tracing, we talk about the baseline, the variability and accelerations. 00:17 When we talk about contraction, the bottom part of this example we discuss if the contractions are normal and what tachysystole means. 00:26 Let's start with baseline. 00:28 So a normal baseline is between 110 beats to a 160 beats per minute. 00:33 And this is for the fetal heart rate. 00:37 Tachycardia is considered to be 160 beats per minute sustained for a 10 minute time frame. 00:43 And bradycardia is considered to be less than 100 beats per minute when it's sustained for a 10 minute time frame. 00:52 So variability talks about the ability of the fetal heart rate to change above or below baseline. 00:59 When the variability is absent that means there's no change in the baseline. 01:04 When it's minimal, it means it's less than 5 beats per minute. 01:08 Moderate is 6 to 25 beats per minute. 01:11 And marked is greater than 25 beats per minute. 01:14 In our example here, we would call this moderate variability. 01:19 For accelerations, we divide them into two categories. 01:23 After 32 weeks, it is an increase in fetal heart rate by 15 beats per minute for 15 seconds before 32 weeks, and increase in fetal heart rate by ten beats per minute for 10 seconds is considered an acceleration. 01:37 Now remember, if the increase in heart rate occurs for over 2 minutes is called a change in baseline. 01:44 Now, contractions. 01:47 A normal amount of contractions are 5 or less contractions in a 10 minute time frame. 01:53 Uterine tachysystole means greater than 5 contractions in 10 minutes. 01:58 Now there's something called Montevideo Units. 02:02 When normally a patient is monotronant labor they have an external fetal monotron. 02:07 Because it sits at top of the abdomen, it only tells us how often a patient is contracting. 02:13 It doesn't tell us how strong those contractions are. 02:17 Within intrauterine pressure catheter we're able to determine the strength of the contractions. 02:22 Now how do we do this. 02:24 We take a 10 minute strip or a 10 minute tracing. 02:28 We look at the contractions during that time and we measure the area under the curve. 02:33 Now a normal amount of contraction or strength of contraction would be between 180 to 220 Montevideo units. 02:43 That's considered to be adequate contractions to allow labor to progress. 02:49 Now that we've talked about the fetal heart rate tracing and some of the terminology, let's talk about the nomenclature. 02:56 So why do we even look at fetal heart tracing. 02:59 Well, fetal heart rate tracing provides an information to us to tell us about the current acid-base status of the fetus. 03:06 Now we have 3 categories. 03:08 Category 1 which is normal. 03:11 Category 2 which can be indeterminate. 03:13 And Category 3 which we consider abnormal. 03:16 Let's see what makes each of those categories. 03:21 So a category 1 tracing. 03:23 In order for a tracing to be considered Category 1, such as this one, the fetal heart rate has to be between 110 to 160 beats per minute. 03:33 There must be moderate variability. 03:35 And there are no late or variable decelerations. 03:41 Now, a Category 2 tracing. 03:44 Again this is indeterminate to determine the acid-base status of our fetus. 03:51 So the fetal heart rate can be between 110 to 160 beats per minute. 03:56 But it can also be 100 beats per minute which remember that means bradycardia. 04:01 But variability must be present. 04:04 It can be greater than 160 beats per minute which again that means tachycardia. 04:09 But again variability must be present. 04:14 As far as the variability it can be minimal or moderate. 04:18 Or if it is absent, such as in this case, there can be no late or variable deceleration for it to be considered a Category 2 tracing. 04:28 Acceleration should be present. 04:32 And if there are decelerations which again those can be late or variable, they can be present if there is minimal or moderate variability present. 04:44 Now, Category 3 tracing. 04:46 This is considered abnormal. 04:47 And this would mean that the acid base fetal status is abnormal. 04:55 So, Category 3. 04:56 What makes a Category 3 tracing. 04:58 As far is variability it is absent with late or variable decelerations. 05:03 Such as in this tracing. 05:07 There can be bradycardia which again is less than a 100 beats per minute. 05:11 Or something called as Sinusoidal Pattern. 05:13 You also see this called a see-saw pattern. 05:15 And that actually shows fetal anemia. 05:19 Now let's talk about the different types of decelerations that we can see on a fetal heart rate tracing. 05:24 We have early decelerations. 05:26 These decelerations particularly mirror the contractions and these are physiologic. 05:31 They are due to the head compression and due to stimulation of the vagus nerve. 05:35 Because they are physiologic, there's nothing that we need to do about them. 05:41 Variable decelerations, you can see there's a sharp decline in the fetal heart decline and there's a sharp incline back to the baseline. 05:50 Variable decelerations are due to cord compression. 05:54 Now, they can be released by doing amino infusion which is placing fluid inside the uterus through the intrauterine pressure catheter. 06:02 That allows the fetus to get off of the cord and to release these variable decelerations. 06:08 Now late decelerations are little bit more ominous. 06:11 These are due to the utero-placental insufficiency. 06:15 These we do have to address and we do want to correct. 06:18 So how do we address them. 06:20 1. We give oxygen to the moms so there's more oxygen going to the fetus. 06:24 2. If we are given pitocin to make contractions happen, we want to stop the pitocin. 06:30 3. We want to give IV fluids because that will allow more fluid to go to the placenta. 06:36 And then 4. We want to commonly place the patient in left lateral decubitus. 06:41 So that means we roll them on to the left side. 06:44 That will rotate the uterus off of the inferior vena cava. 06:48 So we have increased venous return to the placenta. 06:53 Now let's take a case. 06:55 You are called to the bedside of a 23 year old Gravida 1 Para 0 female who was admitted in active labor. 07:04 On her most recent cervical exam she was 5/90 and -1. 07:09 She received an epidural approximately 10 minutes ago. 07:13 Her fetal heart rate tracing which was Category 1, is now shown to be this. 07:19 How would you describe this tracing? What nomenclature would you use? Now would you say that, A. The patient is having early decelerations, most likely from rapid cervical change. 07:37 B. Patient is having late decelerations most likely from rapid cervical change. 07:43 C. Patient is having late decelerations most likely from hypotension related to recent epidural placement. 07:50 or D. Patient demonstrates at Category 1 fetal heart tracing. 07:57 The answer is C. 07:58 We would describe this fetal heart rate tracing as a Category 3. 08:02 We can see that the patient is having a large late deceleration. 08:06 Now it's important to remember that when the epidural is placed, a lot of times moms will suffer from hypotension. 08:12 This causes utero-placental insufficiency. 08:15 And the fetus will compensate by having late decelerations.
About the Lecture
The lecture Labor Stage 1: Fetal Heart Rate Tracing by Veronica Gillispie, MD, MAS, FACOG is from the course Intrapartum Care. It contains the following chapters:
- Fetal Heart Rate Tracing
- Fetal Heart Rate Tracing – Categories
Included Quiz Questions
What is the range for a normal baseline fetal heart tracing?
- 110-160 beats per minute
- 100-150 beats per minute
- 130-160 beats per minute
- 100-130 beats per minute
- 135-145 beats per minute
Which of the following describes an acceleration in the fetal heart tracing in a fetus with a gestational age greater than 32 weeks?
- An increase in fetal heart rate by 15 beats per minute for 15 seconds over a 2-minute tracing.
- An increase in fetal heart rate by 10 beats per minute for 15 seconds over a 2-minute tracing.
- An increase in fetal heart rate by 15 beats per minute for 10 seconds over a 2-minute tracing.
- An increase in fetal heart rate by 10 beats per minute for 10 seconds over a 20-minute tracing.
- An increase in fetal heart rate by 20 beats per minute for 15 seconds over a 20-minute tracing.
A 27-year-old female G1P0 at 42 weeks comes for induction of labor. The woman is on Pitocin, and her last cervical exam: 5 cm/ 80% effaced/ -2 station with a category I fetal heart tracing with contractions every 5-6 minutes. Pitocin infusion was increased. 20 minutes later, she is having one contraction every minute. FHR tracing has a baseline of 165 with absent variability and two late deceleration over a 20-minute strip. What describes the category of FHR tracing and best management?
- Category 3 and Pitocin must be stopped.
- Category 2, the patient has tachysystole, and the Pitocin should be stopped.
- Category 1, it is ok to continue the current course of management.
- Category 2, the patient is likely not taking deep breaths due to pain from regular contractions and should get oxygen supplementation.
- Category 2, the patient should be rotated to relieve cord compression.
Which of the following fetal heart tracings is a category II tracing?
- Baseline 135 with moderate variability, accelerations present, and minimal decelerations over a 20-minute strip.
- Baseline 145 with no variability and late decelerations over a 20-minute strip.
- Baseline 165 with no variability and variable decelerations over a 20-minute strip.
- Baseline 180 with no variability and no accelerations over a 20-minute strip.
- Baseline 80 with no variability and a few late decelerations over a 20-minute strip.
Which of the following is true of sinusoidal category III tracing?
- It indicates fetal anemia.
- It is a sign of maternal polycythemia.
- It indicates cord compression.
- It indicates head compression of the fetus.
- It is a sign of fetal death.
A 29-year-old G4P3 woman at 40 weeks gestational age was admitted to the labor ward in spontaneous active labor. Her last cervical exam was 7 cm dilation/90% effacement/-2 station with a bulging bag of water (intact membranes) and fetal heart tracing was unremarkable with a baseline heart rate of 140 beats per minute and moderate variability without any decelerations. 30 minutes later she felt a large gush of fluid and the fetal heart tracing showed regular early decelerations with each contraction. What occurred to cause this finding?
- Physiologic response to fetal head compression after rapid descent of the fetal head in the pelvis
- Cord compression due to prolapse of the cord
- Uteroplacental insufficiency due to maternal intravascular volume depletion
- Fetal anemia resulting in a sinusoidal fetal heart tracing pattern
- Fetal bradycardia due to uteroplacental insufficiency
Which of the following is NOT true of a sinusoidal pattern on a fetal heart tracing?
- It represents cord compression.
- It indicates fetal anemia.
- It is a category III FHR tracing.
- It requires immediate intervention.
- It suggests abnormal fetal acid/base status.
Which of the following statements is true of tachysystole?
- It is defined as more than 5 contractions over 10 minutes.
- It can only be determined by an internal uterine pressure catheter.
- It can be monitored without intervention as long as the fetal heart tracing is not category III.
- It is defined as more than 2 contractions in 10 minutes.
- It is defined as overlapping contractions without any uterine relaxation in between contractions.
Author of lecture Labor Stage 1: Fetal Heart Rate Tracing

Veronica Gillispie, MD, MAS, FACOG
Customer reviews
3,5 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
1 |
| 1 Star |
|
0 |
I personally do not think that there was not enough of necessary depth taken for this topic that I had to rely on what I learned in medical school or look up information on external sites, which is FINE, but I thought the whole point of these videos were for review and the topics that needed review were not covered. I think the basic concept that of comparing the fetal heart tracing to the maternal tracing is missed. The explanation of the categories was so confusing. It should have just been Category I is this, Category III is this, and Category II is anything not above - this is so plain and simple. Instead, the lecture slide made it look like there were certain criteria that needed to be met for Category II. I do not think this was the best lecture by Dr. Gillispie and I recommend looking for outside sources to review this topic.
Thanks so much for making this complex topic clear and simple.
