Playlist
Show Playlist
Hide Playlist
Trauma: Epidural and Subdural Hematoma


-
Slides 06 Trauma Neuropathology I.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
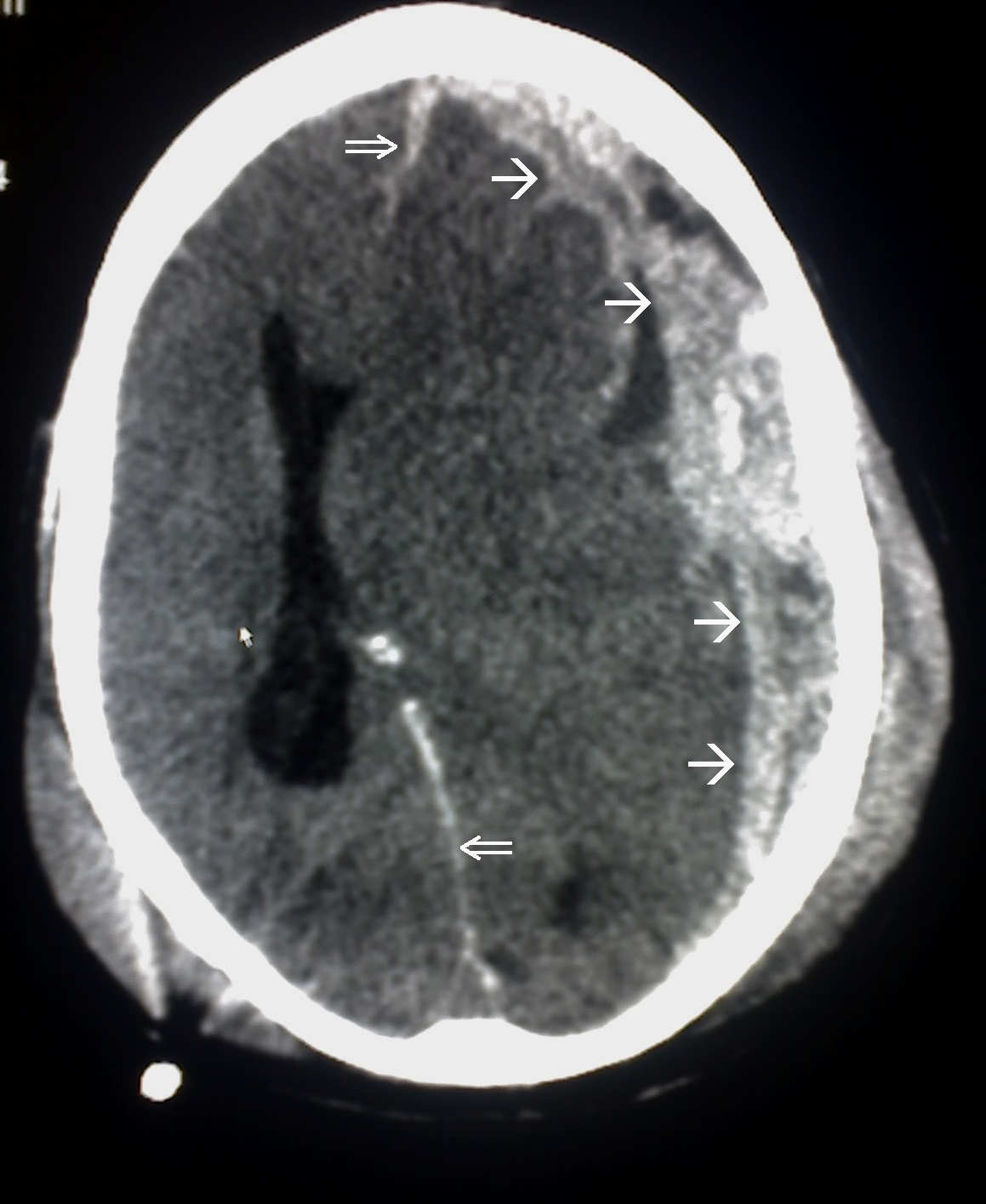
00:01 Let’s begin by looking at epidural. 00:03 I’m going to let you take a look at the CT. 00:05 A beautiful CT of a biconvex structure. 00:10 Obviously, that huge structure over -- Well, that the right side of the brain. 00:14 And on the right side of the skull, you will then notice what? It looks like the lens of the eye. 00:20 But obviously, it is not the lens. 00:22 It is actually accumulation of blood. 00:23 Hence, this is called hematoma. 00:25 This is epidural. 00:28 So what happened? It’s the fact that upon injury to the brain, you have the middle meningeal artery, which then ruptured, resulting in accumulation of blood. 00:36 Hema-, -toma. 00:39 What does lucid interval mean? This is sad. 00:42 It really is sad. 00:44 The child gets hit by a ball and the father rushes out onto the field and says, “Son, son, son, are you okay?” The child gets up and says, “Yeah, daddy. I’m great! Let’s go get some ice cream. 00:53 Lucid. 00:55 Clear. 00:56 What happens next? They go get some Italian ice. 01:00 Next time the child falls, the child never gets back up. 01:04 The child is dead. 01:06 This is epidural hematoma. 01:08 This is called walk and die syndrome. 01:10 Literally, everything’s lucid. 01:13 And then, next time the child or the patient falls, dead. 01:17 Now, you’d think that you get hit by whatever, trauma, and if there’s such trauma that’s been sustained resulting in epidural hematoma, do you not think that this hematoma is then compressing upon the brain? Of course it is. 01:32 So what do you think happens to intracranial pressure? It is going to increase. 01:36 What else may occur? Well, depending as to the site of the hematoma, there’s every possibility that you might then be pushing the brain tissue to the wrong spot. 01:47 Remember that description? “Wrong spot.” Herniation. 01:52 And depending as to where, what if it was by the temporal lobe, which could occur? And then you have the uncus, which is then pressing upon the brainstem. 02:01 What is this called? Transtentorial herniation. 02:04 You see as to how you must be able to put everything together. 02:08 And it’s a very possible that all of this is occurring at the same time. 02:12 Why wouldn’t it? Deficit: Where do you find issues? Contralateral hemiparesis. 02:19 Ipsilateral pupillary dilation. 02:21 The words, we’re talking about your cranial type of issues. 02:25 Contralateral hemiparesis, motor Ipsilateral, cranial nerve, pupillary dilation. 02:31 Why do think? Why do think this is occurring? Well, in this picture actually, the epidural hematoma is then causing herniation of your temporal lobe or the uncus against the third cranial nerve, resulting in the loss of your parasympathetic pupillary constriction. 02:50 And therefore, resulting in ipsilateral pupillary dilation. 02:54 First, with subdural hematoma, this would be the most common of the hematomas. Okay. 03:00 And here in this case, maybe the child was shaking unbeknownst to the father. Okay. 03:07 So happy shaking the baby. 03:08 Or maybe you have a patient that fell down the stairs, Or as we get older, what happens the size of the brain? Gets smaller. Just go see now atrophy. 03:20 As the brain gets smaller, and smaller, smaller or shaking the baby, not good, huh. 03:26 You're shaking the baby or the brain gets smaller, what happens? You're going to pull, on what? Bridging veins. 03:34 You pull the bridging veins enough, what happens? Rupture. 03:37 Now, what do we end up resulting in, please? a subdural hematoma. 03:42 I need you to be careful with this picture here. 03:45 What I want you to focus upon is where that arrow, you see there, that is not a biconvex structure. Okay. 03:54 In fact, with the subdural hematoma, which you want to do here, I need you to go back and refer to epidural hematoma, Will you find that huge biconvex lens like accumulation of blood, versus here, it's that entire structure over that's the left side of the brain. 04:10 And it is where you're looking at the entire area, which more or less has a concave type of appearance. 04:19 Here brain atrophy as we get older, ripping and tearing the bridging vein, and coagulopathy. 04:26 It all may result in what's known as subdural type of hematoma. 04:30 It's the most common can present sub-acutely or chronically. 04:34 Meaning to say that here, you don't have that lucid interval that we talked about quite dramatically in that child in epidural hematoma. 04:46 Fast facts of hematoma or summary epidural trauma: Almost always with focal deficit, contralateral hemiparesis ipsilateral type of pupillary issues. 04:58 Most requiring drainage. 05:00 You need to get in there, I need to bore a hole to decompress because the pressure is so incredibly high. 05:07 Subdural: Alcoholics, elderly, why? The brain is getting smaller. 05:13 What's it doing? It is pulling upon the bridging vein. 05:16 Acceleration-deceleration injury. 05:19 We've seen this twice. 05:22 The first time we saw it, acceleration deceleration. 05:25 I told you about rollercoaster rides or accidents causing diffuse axonal injury, or twisting and swelling of the axon, or you shake a baby, and what may happen? Tearing now the bridging veins. 05:37 Both could occur at the same time. Can't say that it's just one. 05:43 Subtle signs possible. 05:45 Drainage not always necessary. Why? Because the amount of blood that's accumulating here is not going to be as extensive as what we saw with epidural.
About the Lecture
The lecture Trauma: Epidural and Subdural Hematoma by Carlo Raj, MD is from the course Trauma. It contains the following chapters:
- Epidural Hematoma
- Subdural Hematoma
- Hematoma: Summary
Included Quiz Questions
Which of the following statements regarding traumatic brain injuries is TRUE?
- Elderly alcoholics are at risk of developing a subdural hematoma.
- Lucid interval is associated with a subarachnoid hemorrhage.
- Drainage is not required for an epidural hematoma.
- An epidural hematoma shows a crescent-shaped collection of blood on MRI.
- An epidural hematoma can be chronic.
A head CT of a patient who was brought to the ED after a traumatic brain injury shows a lens-shaped accumulation of blood on the left side of the skull. What is a probable physical finding on their exam?
- Left pupillary dilation
- Left hemiparesis
- Right pupillary dilation
- Left pupillary constriction
- Right pupillary dilation and left paraparesis
A patient accidentally hit by a baseball bat did not lose consciousness and felt fine after the incident. He collapses suddenly after a few hours. A physical examination shows left-sided pupillary dilation and weakness on his right side. What is the mechanism of his pupillary dilation?
- Uncal herniation causing injury to the oculomotor nerve
- Subfalcine herniation causing injury to the oculomotor nerve
- Uncal herniation causing injury to the optic nerve
- Transtentorial herniation causing injury to the optic nerve
Author of lecture Trauma: Epidural and Subdural Hematoma

Carlo Raj, MD
Customer reviews
4,5 of 5 stars
| 5 Stars |
|
3 |
| 4 Stars |
|
0 |
| 3 Stars |
|
1 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Clear and Concise. Very Nice. On different point, it was hard to find using search. Perhaps add the "contre" "contrecoup" "coup" but not "chicken coup" as search terms might help other others find this gold.
Good talk on the topic but could be improved by discussion management and when you may consider surgical evacuation vs watch and wait. Also no mention of chronic subdural haematoma.
I really liked this lecture and learned a lot. He broke it down and explained things simply without being condescending, and I found his examples to be easy to remember.
1 customer review without text
1 user review without text
